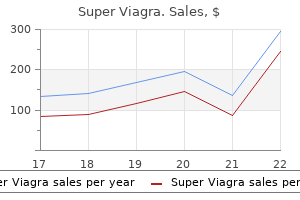
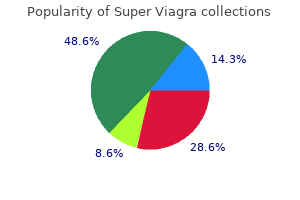
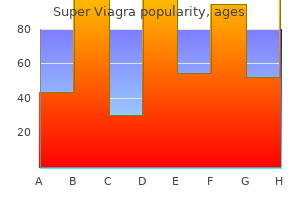
Super Viagra
Super Viagra
Super Viagra dosages: 160 mg
Super Viagra packs: 10 pills, 20 pills, 30 pills, 60 pills, 90 pills, 120 pills, 180 pills

Avoid repeated and aggressive makes an attempt to cut back an incarcerated groin hernia; immediate surgical session ought to be obtained erectile dysfunction uk generic super viagra 160 mg mastercard. No try ought to be made to cut back a hernia with overlying inflammatory adjustments that suggest an underlying strangulated hernia erectile dysfunction vitamin order 160 mg super viagra free shipping. Obturator hernias may be difficult to diagnose unless they prolong onto the thigh or could be palpated via the vagina smoking and erectile dysfunction causes discount 160 mg super viagra with amex. Alternatively, they may manifest with intermittent signs of pain and thigh paraesthesias. The peritoneal sac of an indirect inguinal hernia emerges lateral to the epigastric vessels via the interior inguinal ring (where they may turn out to be incarcerated) and travels along the testicular vessels or round ligament. Spigelian hernias originate a few centimetres below the umbilicus alongside the lateral fringe of the rectus abdominis muscle on the site of its intersection with the arcuate line. Sliding inguinal hernias comprise viscera as part of their wall and should contain the caecum, sigmoid colon or urinary bladder. Costly imaging is typically reflexively ordered for these patients solely to reveal � several hours later � a analysis that could have been elucidated with proper scientific assessment, such as an incarcerated hernia. On the other hand, when stomach pathology is recognized early, steps for further remedy could be expedited. For instance, a patient may be referred to a surgeon more urgently and, if needed, the appropriate radiographic test can be ordered and prioritized over elective research. Thus, strong history and physical examination abilities are important in the outpatient as properly as the emergency room setting. The goal of this chapter is to evaluation the symptoms and physical signs associated with main non-acute belly situations that each one healthcare providers ought to be ready to respect. The patient is asked to lie in the supine position with the knees prolonged and the head of the mattress as flat as can be tolerated. A sheet can be utilized to briefly cover the decrease extremities and genitalia, and the anterior belly wall should be fully exposed. A giant or protuberant abdomen might replicate marked obesity or belly distension from a dilated bowel, a large intra-abdominal mass or ascites. A decrease midline laparotomy scar in a woman could recommend a past hysterectomy or caesarean section, particularly if she has lived in a developing nation. Given the rising use of laparoscopy, you will need to actively search for any small, 1�2 cm scars that could be hidden in the umbilicus, bikini line or elsewhere on the abdomen. Dilated superficial veins coursing along a protuberant stomach are prone to characterize a caput medusae, a mark of portosystemic venous shunting in response to portal hypertension. Skin erythema should be identified as this could be an ominous marker of necrotic underlying bowel. Indeed, erythema over an incarcerated inguinal or ventral hernia is an indication for immediate operative intervention without attempts at discount. Blowing out the stomach demonstrates any limitation of movement as a end result of tenderness and supplies a nice deal of info without any handbook contact. Auscultation During auscultation, place the stethoscope gently on every of the 4 quadrants. It is helpful to simply place the bell on the abdomen and launch the hand in order that solely abdominal sounds are transmitted. Patients with non-acute belly pain could also be discovered to have regular bowel sounds in all quadrants. High-pitched sounds may be heard in the presence of a small bowel obstruction, whereas low-pitched sounds are more common in impending giant bowel obstruction. A affected person who presents with new, extreme belly pain and a very silent stomach in which no sounds are heard over 10 minutes raises issues of a surgical emergency such as a perforated viscus. Listen rigorously for vascular bruits, indicating the presence of turbulent blood flow. Such bruits are clues to vascular pathology similar to renal artery stenosis or aortic disease, or large vascular abdominal tumours. In sufferers with acute stomach ache, lack of dullness over the liver suggests pneumoperitoneum from a perforated viscus. In people with obstructive signs, drum-like tympanic sounds over a distended abdomen suggests a high-grade small or giant bowel obstruction. To additional assess for ascites, ask the affected person to roll barely onto to their left facet, and percuss the left side of the abdomen laterally from the umbilicus. Then have the patient flip to the supine place and repeat the percussion manoeuvre. If ascitic fluid is present, the change from resonant to boring happens more anteriorly and/or medially as the fluid level modifications. Alternatively, have an assistant examiner or the patient place the aspect of their hand vertically over the umbilicus and apply mild strain in path of the backbone. Finally, estimate the scale of the liver by first percussing over the right anterior chest wall, the place there should be resonance from air within the lungs. Mark this level and (b) roll the patient through 30�: when fluid is present, the percussion notice changes at a unique location as a result of fluid movement. At the interface between the decrease edge of the liver and the bowel, resonance might be heard once more. Patients with peritonitis may not tolerate percussion; mild percussion is one approach to elucidate peritoneal signs (see under and Chapter 36). Take care to not frighten the affected person with cold hands, poking movements or sudden, deep palpation. Gentle actions keep away from voluntary muscle guarding, which may be confused with indicators of peritonitis or make it tough to detect intra-abdominal lots. Examine the area of reported ache last to keep away from putting the patient in misery for the majority of the examination. Keep in thoughts that the aim of the examination is to detect indicators of intra-abdominal pathology. Patientreported complaints of ache in the course of the examination must be famous however always compared with the target findings. When these indicators are limited to one quadrant, they mirror localized peritonitis, as in instances of uncomplicated appendicitis or diverticulitis. When these indicators are elicited over the entire anterior abdominal wall, diffuse peritonitis is present. Diffuse involuntary guarding to gentle palpation with related diffuse rebound tenderness raises the suspicion of a perforated viscus or bowel ischaemia, though non-surgical situations such as acute pancreatitis can mimic these findings. A full dialogue of acute surgical circumstances is available elsewhere in this guide. As the affected person inhales deeply, the sting of an enlarged liver will move down to touch the analyzing hand. The fringe of a � An epigastric bulge with out an related scar reflects a congenital or acquired epigastric hernia. An enlarged liver may replicate early cirrhosis, cumbersome metastatic illness or other liver issues. On deep inspiration, the lower fringe of an enlarged spleen can be detected below the left costal margin. This methodology can also be used to palpate enlarged kidneys or assess for tenderness. Always assess the stomach aorta in sufferers with acute or persistent abdominal pain. Gently press down within the centre of the abdomen until the aortic pulsation is felt. Immediately refer patients with an enlarging aortic width or tenderness over a identified aortic aneurysm to a vascular surgeon. The stomach and colon may also be appreciated on bodily examination in some sufferers. A agency, palpable mass within the epigastrium might characterize a transverse colon or gastric malignancy. Hard stool could also be palpated inside the transverse or sigmoid colon in patients with severe constipation. Finally, at all times carry out a rectal examination in any patient with belly ache to evaluate for rectal plenty and occult blood. In girls, a devoted pelvic examination can exclude a gynaecological cause of non-acute stomach ache. Combined inspection and palpation of the belly wall floor and each groins allows for the detection of any hernias, abscesses or other plenty.
Patients can present throughout the first few days of life with a delayed passage of meconium erectile dysfunction treatment london super viagra 160 mg buy cheap line, belly distension and Meconium Ileus and Meconium Plug Syndrome An lack of ability to pass meconium within the first few days of life could be indicative of useful obstruction of the distal bowel erectile dysfunction viagra free trials super viagra 160 mg order with visa. Rectal examination with the passage of a rubber catheter is useful to determine the presence of meconium erectile dysfunction doctor mn purchase super viagra 160 mg mastercard. A contrast enema exhibits filling defects within the colon and a reflux of distinction into the extra proximal dilated bowel. Meconium ileus is associated with cystic fibrosis and is characterized by inspissated meconium throughout the distal small bowel that causes an obstruction. These infants can turn out to be quite distended, and the abdomen may have a doughy consistency because of the presence of small bowel loops distended with thick meconium. A distinction enema will present a small colon with a reflux of distinction into the world of the terminal ileum, thereby excluding potential atresia. Water-soluble contrast enemas can help with the evacuation of meconium to relieve the obstruction without the need for surgical procedure. Alternatively, if the phase of aganglionic colon is short, infants might present later in life. In instances of enterocolitis, the stool could appear greyish in color and unusually foul-smelling. Enterocolitis can lead to demise and requires prompt remedy with antibiotics, intravenous fluid resuscitation and evacuation of the retained stool with saline rectal irrigations. A contrast enema may demonstrate a transition level between the proximal, dilated, ganglionated bowel and the distal decompressed, aganglionated bowel. In early shows, the transition level could not but be apparent on such studies. The diagnosis is confirmed with a rectal biopsy to look for the presence of ganglion cells. These may be distinguished based mostly on the extrusion of stomach organs, the presence of a overlaying membrane and the place of the umbilical cord insertion. An omphalocele is characterised by extruded belly contents covered by a sac composed of amnion. Physical examination at birth reveals meconium output from a fistula tract located extra anteriorly on the perineum and the absence of a wellformed anus within the regular location. In instances where the rectum is high in the pelvis, the fistula tract might join with the genitourinary tract as an alternative of the perineal skin. Infants with options of Down syndrome and an absent anus often have well-formed perineal muscles and not utilizing a perineal fistula and characterize a special class of anorectal malformation. Failure of the abdomen to empty because of the hypertrophied pylorus results in an overdistended abdomen and retained feedings. Parents typically report the forceful projectile emesis of curdled milk of volumes in extra of the volume of their most up-to-date feeding. These infants often appear dehydrated with a sunken fontanelle, and produce less urine. In the calm infant, the hypertrophied pylorus could be palpated just under the liver edge. Ultrasound is usually used to measure the length of the pyloric channel and the thickness of the muscle to verify the analysis. This is frequently associated with a prodrome of gastroenteritis when lymphoid aggregates with the bowel wall hypertrophy and serves as lead factors for the intussusception. The presence of blood within the stool is indicative of mucosal ischaemia and is a late sign. Abdominal examination is usually unremarkable besides in advanced instances during which a perforation has occurred and signs of peritonitis may be current. If the intussusception has progressed distally, the intussusception may be palpated by digital rectal examination. Abdominal examination can range from fully benign to indicators of peritonitis or emesis and belly distension attribute of small bowel obstruction. Clinically, this process manifests with stomach distension, bloody stools and/ or emesis. Symptoms usually progress rapidly, with neonates exhibiting lethargy, apnoea, bradycardia and hypotension. In male neonates with hernias, the scrotum could turn out to be discoloured, indicating the presence of free air (bluish) or free meconium (dark) inside the abdomen. Abdominal radiographs might reveal pneumatosis throughout the bowel wall or portal venous gas. In cases of full-thickness ischaemia, free air signifies the presence of a perforation. Acute Appendicitis Acute appendicitis can happen at any age, however the presentation is usually delayed in youthful children. Abdominal examination is characterized by right lower quadrant tenderness however can also demonstrate diffuse tenderness and abdominal wall rigidity attribute of peritonitis. Omphalomesenteric Duct Remnant the omphalomesenteric duct exists as a connection between the yolk sac and the mesentery throughout embryological development and is then obliterated by 9 weeks of gestation. On examination, sufferers have icterus, obvious jaundice and a firm, palpable liver edge. While the precise aetiology of biliary atresia stays unknown, this may be a progressive inflammatory process of the biliary structure, and the result is greatest when the illness is identified and handled before eight weeks of age. Key Points the differential analysis of neonatal bowel obstruction can be narrowed down primarily based on the onset and type of the presenting symptoms. Bilious emesis within the neonatal period should prompt quick concern for malrotation with midgut volvulus and is a paediatric surgical emergency. Common paediatric surgical ailments are greatest distinguished by the age of presentation and the abdominal examination. Neonatal jaundice that persists for longer than 2 weeks, is progressive or is associated with acholic stools ought to immediate analysis for biliary atresia. A 4-week-old toddler, feeding well prior to presentation, has a sudden onset of brilliant green emesis with out belly distension. Bilious emesis is the hallmark presentation of midgut volvulus and is a surgical emergency. An incapability to handle oral secretions points to obstruction at the oesophageal degree. Infants with duodenal obstruction can deal with oral secretions but normally have emesis shortly after feeding. Meconium ileus causes bowel obstruction on the level of the terminal ileum and is associated with the development of marked belly distension. A 1�month-old premature infant, weighing 750 g, has been tolerating feeds and develops bradycardia, bilious emesis, belly distension and stomach erythema. Bilious emesis ought to always prompt concern for midgut volvulus, and this analysis have to be excluded. However, given the scientific historical past, necrotizing enterocolitis is the most probably diagnosis. A perforated appendicitis may be associated with fever and a palpable proper lower quadrant inflammatory mass. Intussusception happens in toddlers, and the intussusception can typically be palpated in the best lower quadrant. A bloody stool indicates mucosal ischaemia from recurrent or persistent intussusception. Pyloric stenosis is characterised by non-bilious emesis in infants aged 2�8 weeks. In the relaxed baby, the thickened pyloric muscle is palpable in the best higher quadrant just below the liver edge. If the diverticulum incorporates gastric mucosa, acid manufacturing causes small bowel ulceration and painless bleeding with blood in the stool. Match the physical findings with the appropriate belly wall defect: 1 Covered defect 2 Herniated liver 3 Herniated bowel four Defect to the proper of the umbilicus 5 Umbilicus inserts throughout the defect a Gastroschisis b Omphalocele Answers a three, 4. Omphaloceles are lined by a membrane, with the umbilical cord inserting instantly onto the membrane. Despite advances in diagnostic know-how, the cornerstone in the analysis of the urology affected person remains a radical medical history and bodily examination. The utility of these primary scientific expertise usually results in an correct prognosis or, if not, to a differential prognosis that guides the choice of essentially the most appropriate laboratory and radiological studies. It is important to assess the color and odour of the urine, and the presence of blood and sediment.
Graft administration An arthroscopic switching rod erectile dysfunction shake ingredients super viagra 160 mg on-line, positioned through the posteromedial portal between the graft and the posterior tibial cortex impotence quit smoking super viagra 160 mg online buy cheap, can facilitate graft passage by reducing friction erectile dysfunction drugs and alcohol generic 160 mg super viagra fast delivery. Avoid penetrating gentle tissue with the Beath pin while passing by way of the anterolateral portal to stop the graft from getting caught within the soft tissue. An anterior tibial pressure ought to be utilized during fixation to stop posterior subluxation. The affected person is woke up and taken to the recovery room, where ache and neurovascular status are reevaluated. Patients could additionally be saved overnight for pain management and to monitor their neurovascular standing. Patients are given instructions for exercises (quadriceps units, straight-leg raises, and calf pumps) and crutch use. The brace is unlocked after 4 to 6 weeks, and usually is discontinued after eight weeks. Symmetric full hyperextension is achieved, and passive inclined knee flexion, quadriceps sets, and patellar mobilization workouts are carried out with the assistance of a bodily therapist for the first month. Mini-squats are performed from 0 to 60 levels after the primary week and from zero to 90 degrees after the third week. The objectives for achievement of flexion are 90 degrees at four weeks and a hundred and twenty degrees at eight weeks. Residual laxity can also happen because of graft positioning or failure to handle concomitant ligamentous harm. The thigh and calf ought to be routinely palpated to ensure no compartment syndrome develops from fluid extravasation into the gentle tissues. Posterior cruciate ligament reconstruction: double-loop hamstring tendon autograft versus Achilles tendon allograft: clinical results of a minimum 2-year follow-up. Posterior cruciate ligament reconstruction using single-bundle patella tendon graft with tibial inlay fixation: 2- to 10-year follow-up. Arthroscopic reconstruction of the posterior cruciate ligament using tibial-inlay and double-bundle technique. Comparison of tibial inlay versus transtibial methods for isolated posterior cruciate ligament reconstruction: minimal 2-year follow-up. Long-term results of nonoperative therapy of isolated posterior cruciate ligament accidents in the athlete. Clinical outcomes after isolated arthroscopic single-bundle posterior cruciate ligament reconstruction. The pure history of acute, isolated, nonoperatively handled posterior cruciate ligament accidents. Conservative remedy for rugby football players with an acute isolated posterior cruciate ligament damage. Loss of motion (usually decreased flexion) can result from errors in graft positioning or excessive tensioning throughout graft Chapter forty five Repair of Acute and Chronic Knee Medial Collateral Ligament Injuries Christian Lattermann and Darren L. It inserts roughly four to 6 cm distal to the medial joint line and could be divided into an anterior and a posterior portion. The anterior portion tightens in flexion; the posterior portion tightens in extension. The posteromedial nook provides rotational stability to the medial aspect of the knee. A thorough examination of the knee ought to always embody the following assessments: Meniscus: tenderness instantly on the joint line is a delicate sign for a meniscus injury. Patella: the apprehension sign and localized tenderness on the lateral or medial aspect of the patella or the lateral trochlea signifies a possible patella dislocation, which can go hand-in-hand with an intra-articular effusion. The location of the acute or persistent damage -femoral or tibial-also can be evaluated. In athletes, a return to sport-specific training is secure as soon as 80% of the maximum operating velocity is achieved. The joint area opens greater than 10 mm and permits full passage of the arthroscope into the again of the medial compartment. A proximal meniscal lift-off suggests a tibial-sided tear, whereas a distal lift-off suggests a femoral-sided tear. Examination beneath anesthesia should embrace a full ligamentous examination (ie, Lachman test, pivot shift take a look at, varus/valgus stress take a look at, dial test, anteromedial drawer test). The procedure additionally can be carried out on an everyday operating desk with the affected person within the supine place with a bolster positioned beneath the knee. In case of a proximal extension, the incision should be slightly curved posteriorly over the medial femoral epicondyle. Retraction of the skin exposes the sartorius fascia, which must be split in a longitudinal or T fashion. This incision can be carried down through the capsule to expose the meniscal attachments. Three or 4 double-loaded suture anchors are then placed along the medial border of the tibial plateau about 5 mm under the joint line. In the Bosworth reconstruction, a semitendinosus tendon is harvested utilizing the open or closed tendon stripper. Once the isometric web site is identified, the semitendinosus may be routed round a screw and washer femorally and can be connected distally using a staple or bone tunnels. A double anterior tibialis tendon or a split Achilles or patella tendon can be used for this technique. Fixation may be achieved in various ways-bone tunnel utilizing a delicate tissue screw fixation, bone block using an interference screw fixation, bone trough, or screw and washer fixation. The allograft may be anchored anteriorly and posteriorly along the anatomic attachment sites using an interference screw (as depicted), a screw and washer, or a staple. This attachment can be utilized within the reconstruction if the length is sufficient; if not, it could be sutured to the reconstruction. The common time to return to athletic activities is between 19 and 23 days, on average, for grade 1 and a pair of injuries, respectively. Either early surgical treatment or repetitive scientific examination to assess the gradual return of valgus stability over the course of four weeks is advisable. Medial collateral ligament reconstruction with allograft using a double-bundle technique. The non-surgical management of isolated medial collateral ligament injuries of the knee. Treatment of isolated medial collateral ligament accidents in athletes with early practical rehabilitation: a five-year follow-up examine. Insufficiency in the posterolateral constructions of the knee can lead to a varus-thrust gait and the feeling of instability, especially when the knee is in extension through the toe-off section of strolling. The superficial layer is made up of the iliotibial tract anteriorly and the biceps femoris posteriorly. The widespread peroneal nerve lies deep and posterior to the biceps femoris on this layer on the level of the distal femur. The popliteofibular ligament exists as a direct static attachment of the popliteus tendon from the posterior fibular head to the lateral femoral epicondyle. The arcuate ligament is a Y-shaped ligament that reinforces the posterolateral capsule of the knee and runs from the fibular styloid to the lateral femoral condyle. In radiographs, the arcuate fracture reveals an avulsion of this ligament off of the fibular styloid. This ligament is the primary static restraint to varus stress from zero to 30 levels of knee flexion. This complicated acts as a "sling" of static and dynamic restraint to rotation of the lateral tibiofemoral articulation. This mechanism may be brought on by blunt posterolaterally forced trauma to the medial proximal tibia, such as a helmet to the knee in football. The deep layer of the posterolateral corner consists of the joint capsule and the coronary ligament, the popliteofibular ligament, the arcuate ligament, the lateral collateral ligament, and the fabellofibular ligament. Other mechanisms of injury include hyperextension alone, hyperextension with an external rotation drive, a extreme varus pressure alone, or a severe exterior rotation torque to the tibia.
Massive uncontrolled gastrointestinal bleeding can lead to exsanguination and demise erectile dysfunction 38 cfr 160 mg super viagra overnight delivery. Compensatory mechanisms could additionally be inadequate in the aged and in sufferers with cardiovascular and other medical comorbidities erectile dysfunction protocol pdf download free super viagra 160 mg buy with mastercard, in whom deterioration occurs rapidly erectile dysfunction fun facts discount super viagra 160 mg on line. The administration of gastrointestinal bleeding is set by its aetiology and the placement of its supply. Predisposing components embrace obesity, feminine gender, parity and a food regimen high in animal fats. Brown stones develop secondary to bacterial colonization of the biliary tract and may develop in both the bile ducts or the gallbladder. The commonest symptom is an assault of biliary colic, which often develops 1�2 hours after a fatty meal. Gallbladder contractions pressure the stone in opposition to the orifice of the cystic duct, causing a rise in intraluminal strain and pain. The ache is usually severe and described as a uninteresting pressurelike discomfort in the best higher quadrant or epigastrium that may radiate to the again and proper shoulder. In some patients, the ache may be unrelated to meals and have a circadian sample, peaking within the evening. Similar signs may develop in sufferers with biliary dyskinesia within the absence of stones. The pain of biliary colic is visceral, and the physical findings are minimal and limited to delicate right upper quadrant tenderness. Acute Cholecystitis the persistence of biliary colic for over a quantity of hours may be a manifestation of the event of acute cholecystitis. The symptoms of acute cholecystitis are unremitting and extra extreme than those of colic. With inspiration, the gallbladder moves downwards, and if it is infected the resulting contact along with your hand will cause ache and the affected person will generally hold their breath. The omentum often seals off the area of irritation, inflicting a tender and generally palpable mass in the proper upper quadrant. On the opposite hand, if the inflammation resolves but the obstruction persists, old bile may be absorbed and the gallbladder will fill with clear fluid (hydrops of the gallbladder), producing chronic right higher quadrant tenderness. Acute acalculous cholecystitis might develop in the absence of gallstones in some critically ill sufferers. The differential diagnosis of acute right upper abdominal ache additionally contains acute appendicitis, hepatitis, hepatomegaly, pyelonephritis, nephrolithiasis and the perforation of a peptic ulcer. Intrathoracic situations include myocardial infarction and right decrease lobe pneumonia. Right-sided coronary heart failure could lead to symptomatic enlargement of the liver and dyspnoea. Choledocholithiasis Stones might pass from the gallbladder into the frequent bile duct or develop there de novo. Small stones can move via the ampulla into the duodenum, inflicting self-limiting signs of biliary colic. Impaction of the stone in the common bile duct produces persistent symptoms and obstructive jaundice. Obstruction of the bile ducts usually causes ascending cholangitis and systemic sepsis. Other aetiologies are less widespread and embrace drugs, metabolic causes (hyperlipidaemia and hypocalcaemia), trauma, endoscopic retrograde cholangiopancreatography, pancreas divisum, viral infections, vascular causes (ischaemia and vasculitis) and tumours. Pancreatitis typically presents with severe acute upper belly pain with radiation to the again. Sitting up and leaning forwards, or mendacity on the facet in the knee�chest position, may convey some aid. Tenderness is limited to the higher abdomen and is often not associated with indicators of peritoneal irritation. In instances of severe pancreatitis, tachycardia, hypotension and oliguria might happen secondary to hypervolaemia. Abdominal distension might develop due to ileus, resulting in hyperresonance, and later be augmented by ascites, resulting in dullness on percussion. Computed tomography demonstrates oedema of the pancreas and surrounding tissues (arrow). The administration of the other severe pathologies that will mimic pancreatitis (gastrointestinal perforation, rupture of an abdominal aortic aneurysm, acute mesenteric ischaemia) is an emergency operation. Chronic Pancreatitis Unless necrosis develops, the irritation and the injury to the gland brought on by acute pancreatitis are reversible. Chronic pancreatitis, secondary to repeated insults (usually alcohol), leads to atrophy of the pancreatic parenchyma and stricturing of the ducts. Intra-abdominal Abscess Intra-abdominal abscesses may develop as the results of an infectious course of. Patients have non-specific signs of systemic inflammatory response with variable degrees of sepsis, including an intermittent spiking fever. Examination of the abdomen usually elicits tenderness in the space the place the abscess is positioned. With an intraperitoneal abscess, the severity of guarding and rebound tenderness depends on the scale of the abscess and its relation to the belly wall. Abscesses underlying the abdominal wall are accompanied by signs of local peritoneal irritation. Occasionally, a large gas-filled abscess might produce hyperresonance on percussion. Patients with a subphrenic abscess often complain of higher abdominal or again pain, which may radiate to the ipsilateral shoulder. Diaphragmatic irritation could cause hiccups: subcostal and decrease thoracic wall tenderness is current. On examination and imaging, the indicators of pleural effusion and atelectasis are characteristic. Exquisite tenderness could additionally be present on rectal and vaginal examination, the place the bulging, fluctuant area may be palpated. In these instances, belly tenderness may be minimal, with flank and costovertebral angle tenderness predominating. Amoebic Liver Abscess Entamoeba histolyticum occurs worldwide, with an increased prevalence in counties with low sanitation ranges. Primary intestinal infection may result within the spread of parasites by way of the portal circulation into the liver. The indicators and signs are just like these of a pyogenic liver abscess however are much less distinguished and may be current for an extended time period. If inadequately handled, the abscess could rupture into the peritoneal cavity or erode into adjacent organs. The granulomatous reaction from colonic infection might produce a focal mass lesion. Acute Pyogenic Liver Abscess An intrahepatic abscess might mimic a subphrenic abscess. The two major sources are direct spread from a biliary infection and portal vein spread from any intra-abdominal an infection. Haematogenous unfold is possible from distant sources (endocarditis, pyelonephritis). Local spread might result from penetrating injuries, a subphrenic abscess or an empyema. The underlying trigger is obstruction of the lumen by hyperplasia of the lymphoid follicles, faecoliths, parasites or tumour. The omentum is underdeveloped in younger children, resulting in a higher morbidity on this group. The classic presentation is the gradual improvement of mid-abdominal visceral ache over a interval of lower than 24 hours. The onset of obscure colicky pain is adopted by anorexia and, in most sufferers, nausea and vomiting. As transmural irritation develops and irritation of the parietal peritoneum occurs, the fixed ache localizes to the right decrease quadrant and is exacerbated by motion and coughing. This is because of a displacement of bowel loops and motion of the inflamed appendix. Simultaneous palpation of the best lower quadrant with the left hand and of the left lower quadrant with the best hand may help to higher establish delicate variations and the involuntary guarding of early disease (the Butov manoeuvre). The tenderness could also be higher and simulate acute cholecystitis if the anatomical position of the caecum is unusually high.
Severe ischaemia often requires surgical embolectomy with or without thrombolysis erectile dysfunction doctor el paso generic super viagra 160 mg mastercard. If the subclavian artery has a brief affected phase impotence at 55 buy super viagra 160 mg without a prescription, resection and primary anastomosis may be carried out erectile dysfunction treatment in lucknow 160 mg super viagra buy amex. Distal vascular occlusions because of persistent embolization might require a distal bypass. Haemangiomas normally turn out to be evident within the early neonatal interval; approximately eighty per cent are single tumours and 20 per cent happen at multiple sites. The tumour proliferates in the superficial dermis, and the skin turns into raised, bosselated and a vivid crimson color. If the haemangioma lies within the deeper dermis or the subcutaneous tissue, the overlying pores and skin is slightly elevated with a bluish hue. The old phrases cavernous haemangioma to describe a deep lesion and capillary haemangioma for a superficial one are complicated and finest avoided. Palpation makes it easier to differentiate a haemangioma from a venous malformation. By contrast, a venous malformation is delicate and easily evacuated by compression; it enlarges with dependency and disappears with elevation of the involved limb. A typical haemangioma grows quickly over the primary 6�8 months of life and reaches a plateau by 1 yr. After this, indicators of involution appear � the colour fades from vivid crimson to a dullish purple hue, the skin progressively gets paler, the tumour is less tense on palpation and its measurement slowly diminishes. Infants with limb haemangiomas have a excessive danger of visceral lesions, mainly intrahepatic haemangiomas. Platelet trapping � Kasabach�Merritt syndrome � is another complication of cutaneous haemangiomas. The concerned skin becomes deep reddish-purple, tense and shiny, and petechiae and ecchymoses are often seen overlying and adjoining to the haemangioma. Severe thrombocytopenia carries a risk of haemorrhage, both gastrointestinal, peritoneal, pleuropneumonic Table 32. For example, a small haemangioma within the eyelid can distort the growing cornea, producing astigmatism and amblyopia, and a subglottic haemangioma may be potentially life-threatening, presenting insidiously as biphasic stridor at 6�8 weeks of life. Vascular Malformations Congenital vascular malformations are medical syndromes that present with a big selection of characteristics such as naevi (see p. [newline]They are the end result of an interaction between genetic and environmental components, and these elements are included into the Hamburg classification (Table 32. This abandons much less descriptive phrases such as Klippel�Trenaunay and Parkes�Weber syndromes. Although cutaneous vascular malformations are present at start, not all are essentially apparent: � A capillary malformation, or port wine stain, is seen in a neonate. These lesions grow in parallel with the kid but sometimes all of a sudden increase, as seen, for example, with a lymphatic lesion complicated by a viral or bacterial infection. This also happens when a venous lesion thromboses, or when venous and arteriovenous lesions are affected by hormonal adjustments. In basic, the lesions are macular and sharply demarcated, ranging from pale pink to deep red in colour. The overlying skin is regular in texture, and varicosities, ectasias or localized spongy plenty may be evident. In the early phases, a pink stain and an elevated temperature of the surrounding skin are the only indicators suggestive of an arteriovenous malformation. Malformations with arteriovenous fistulae are associated with hypertrophy, whereas atrophy is usually seen with arteriovenous fistulae. Pathophysiologically, the diversion of blood from the arterial to the venous circulation via the fistulae results in distal hypoxia. Hypoxia and venostasis enhance the precipitation of calcium phosphate, enhancing osteoblastic activity. In a congenital arteriovenous fistula, the lower extremity is the most typical web site, followed by the upper extremity, the head and the neck in reducing order of frequency. This is sometimes known as a scorching ulcer as a outcome of the surrounding skin feels hotter than regular due to the diversion of blood. Care have to be taken not to attribute the inequality of limb lengths � and the scoliosis that follows � to shortness of the unaffected leg. The extremity is appreciably hotter and often moister than that on the unaffected aspect. Proximal shunting has triggered distal ischaemia requiring amputation of the center and ring fingers. Using a stethoscope utilized over the fistula, a steady high-pitched bruit with systolic accentuation is pathognomonic. There are two kinds of congenital arteriovenous fistula � localized and diffuse. In the diffuse selection, which is comparatively common, the arteriovenous communications are deep and clinically indiscernible, probably being sited in the bone. Acquired arteriovenous fistulae result from injuries, normally stab wounds or through-and-through gun shot wounds. Pain, an offensive odor, time off work, lack of a job and social isolation are only a few of the problems these patients encounter. It is essential to take a detailed history as ulceration has a large variety of causes (Table 32. Note the arterial dilatation, the early venous filling and the residual metallic fragments from the unique shrapnel injury. The ulcer is associated with swelling, skin pigmentation and induration, all suggestive of venous hypertension. A history of intermittent claudication or rest ache, with an absence of palpable arterial pulses, is suggestive of ischaemic arterial illness. Loss of hair, dystrophic nails and pale and cold skin with poor capillary filling are additionally present. However, a swollen leg with pores and skin induration may be present if the affected person keeps the leg dependent for pain aid in profound ischaemia. Ischaemic ulcers tend to be dry, painful and deep, exposing tendons, fascia and bones. Mixed ulcers, with coexisting arterial and venous elements, make up 12 per cent of all ulcers and add to the problem of prognosis. Venous hypertension and cardiac failure enhance the pressure within the postcapillary venules, leading to a backdiffusion of fluid into the interstitial tissues. Hypoproteinaemia reduces plasma osmolarity, with an increase in capillary diffusion. Examples are coronary heart failure, renal failure and hypoproteinaemia (from liver failure or malnutrition). A painless ulcer situated over the metatarsal heads on the sole of the foot with heat skin on the foot and palpable pedal pulses is more prone to be purely neuropathic in origin. Sensory impairment in the foot, mainly related to pain and temperature change, could be very more probably to be evident. However, ischaemia should be suspected in ulcers that present no proof of healing after 2 weeks of antibiotic therapy and native care. Features that suggest this prognosis are unusual or overabundant granulation and rolled irregular edges. Artefactual (fictitious) ulcers are self-induced lesions from which the affected person benefits, maybe through elevated attention or being the subject of litigation. They are usually produced on exposed sites by scratching with the nails or with various implements, or by cigarette burns. They must be suspected when ulcers are of bizarre or artefactual shapes, present delayed therapeutic or have a good healing edge and underlying granulation, or when uncommon organisms are recognized. When the oedema is generalized and symmetrical, the cause is a systemic abnormality, whereas in localized swelling a local cause ought to be suspected. In basic, oedema represents an imbalance between capillary filtration and lymphatic drainage. One operate of the lymphatic system is to compensate for will increase in capillary filtration; it due to this fact has a considerable function in the improvement of oedema. Swelling current in each lower limbs or in both upper limbs and the face signifies inferior or superior vena cava syndrome as a end result of native disease in the abdomen or chest causing obstruction of the venous outflow.

Epilobium angustifolium (Fireweed). Super Viagra.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96440
The second pin is positioned with the use of an angled information erectile dysfunction treatment without medication order super viagra 160 mg overnight delivery, fluoroscopy impotence with beta blockers 160 mg super viagra order with visa, or each close to the tip of the higher trochanter and directed into the femoral head at a 90-degree angle to the femoral shaft once the fracture has been decreased and the neck�shaft angle restored what food causes erectile dysfunction super viagra 160 mg purchase amex. The chisel is inserted parallel to the 2 guide pins, simply distal to the second pin. Care must be taken to keep the right alignment of the chisel with the shaft of the femur because this determines the flexion-extension of the fracture, which is fixed once the blade plate is inserted. The chisel is aimed to pass via the center of the neck and seat in the inferior portion of the femoral head. Because of the anterior translation of the femoral head on the shaft, the insertion website is in the anterior half of the trochanter. The position of the chisel must be continuously checked with fluoroscopy before and through its insertion. The chisel is carefully removed and the appropriatelength blade plate is inserted and gently seated into the proximal fragment. The insertion must be incessantly checked with biplanar fluoroscopy to make certain that the blade follows the trail made by the chisel. Once the blade is seated, essentially the most proximal screw is placed through the implant into the medial cortex of the proximal femoral neck, rigidly securing the implant to the proximal fragment. Fracture reduction is now achieved by bringing the plate to the shaft and controlling size and rotation. A femoral distractor may be used on the lateral facet of the femur, with the proximal pin within the head and neck fragment and the distal pin placed distal to the tip of the plate. Distraction is applied across the fracture to gain fracture alignment and size via gentle tissue tensioning using an oblique discount technique. Chisel inserted after femoral head and neck and trochanteric block had been secured with lag screws. The plate is then mounted to the shaft fragments with screws in the standard manner, and lag screws are inserted where the pointed discount clamps were beforehand placed. The final fracture alignment and size, in addition to the femoral head, are examined with fluoroscopy to guarantee correct fracture discount and to make certain that there was no head penetration by the implant. Pointed reduction clamps are used to cut back comminuted fragments to the plate without stripping them of sentimental tissue attachments. If acceptable, the distraction is decreased to allow fragment settling and fracture compression. The wound is then closed in a layered style; the muscle, fascia, subcutaneous tissue, and pores and skin are repaired individually. Use of an improperly angled gadget will forestall central and deep placement of the lag screw in the femoral head and will increase the incidence of fixation failure. Many totally different device methods exist with slight variations of method and implant design. Familiarity with the selected device is important, and a trial run on a plastic bone mannequin can be helpful. Positioning of the lag screw centrally and deep inside the femoral head is probably one of the most necessary components to shield in opposition to implant cutout. Fracture of this construction throughout implant insertion could result in the next incidence of fracture collapse and poorer outcomes when a sliding hip screw is used for fracture fixation. When this pitfall is encountered, re-establishing the lateral cortex is important and may be accomplished by adding a trochanteric plate to the sliding hip screw or conversion to an intramedullary device. Gravity and muscular pull tend to the fracture into an apex-posterior or apex-anterior place, respectively, depending on the fracture pattern. Pointed discount clamps or percutaneously placed joysticks can help within the discount in this airplane whereas limiting delicate tissue disruption of the fracture. Subtrochanteric fractures in younger sufferers are often fairly comminuted and lack definitive anatomy to precisely choose rotation alignment from the fracture alone. In these circumstances rotation malalignment of the limb could be assessed by aligning the hip and knee within the anteroposterior plane. Patients are mobilized as quickly as their cardiopulmonary and mental standing will safely enable, often by postoperative day 1. Unrestricted instant postoperative weight bearing is best for the patient to adjust to, and a number of investigations have proven no improve in fixation failure as a result of this postoperative rehabilitation protocol. B Koval et al8 used gait analysis to show how sufferers successfully autoregulate their weight bearing postoperatively, with the patients who had the least-stable fracture patterns preoperatively putting the least amount of weight on their legs immediately postoperatively. Patients ought to be seen 2 weeks postoperatively to check for uneventful wound therapeutic. Follow-up radiographs should be obtained at 2, 6, and 12 weeks to examine for managed fracture impaction, exclude any fixation gadget issues, and assess fracture therapeutic. Follow-up radiograph 6 months postoperatively showing secondary fracture displacement. One-year mortality rates after fixation of peritrochanteric hip fractures vary from 7% to 27%, with most research discovering a price of 15% to 20%. Postoperative functional standing also depends on quite a few variables: Socioenvironmental useful status has been proven to be of great significance in determining the postoperative operate standing of a patient. Another 40% of sufferers have increased dependency on ambulation gadgets but remain ambulatory. Twelve % of sufferers become household-only ambulators, and 8% of patients become nonambulators postoperatively. This complication is seen in 4% to 20% of fractures, normally inside four months of surgery. The placement of the lag screw, then again, could be controlled by the physician. A central and deep place with a tip�apex distance of less than 25 mm has been proven to significantly cut back the incidence of proximal fixation loss. The low incidence is likely as a result of the well-vascularized nature of the cancellous peritrochanteric region of the hip via which these fractures develop. This is commonly seen in instances of unrecognized lateral wall fractures (either iatrogenically induced by implant placement or unrecognized from the original trauma). Use of intramedullary fixation devices and vigilant follow-up could assist keep away from this complication. The value of the tip-apex distance in predicting failure of fixation of peritrochanteric fractures of the hip. Awareness of tip-apex distance reduces failure of fixation of trochanteric fractures of the hip. Results of intertrochanteric femur fractures treated with a 135-degree sliding screw with a twohole facet plate. Weight bearing after hip fracture: a potential series of 596 geriatric hip fracture sufferers. Postoperative weight-bearing after a fracture of the femoral neck or an intertrochanteric fracture. Biomechanical evaluation of the dynamic hip screw with two- and four-hole sideplates. Peritrochanteric femoral fractures treated with a dynamic hip screw or a proximal femoral nail: a randomised research comparing postoperative rehabilitation. Treatment of unstable intertrochanteric fractures with anatomic reduction and compression hip screw fixation. Trochanteric gamma nail and compression hip screw for trochanteric fractures: a randomized, prospective, comparative examine in 210 elderly patients with a new design of the gamma nail. Nonoperative treatment of proximal femoral fractures in the demented, nonambulatory patient. For this chapter, retrograde femoral nailing will discuss with nails with an intercondylar start line that reach through the shaft region to the proximal femur. In certain fracture conditions, shortened nails (supracondylar nails) can be used with the same place to begin for fixation of distal femoral fractures. Although less widespread, femoral shaft fractures can occur in isolated sports activities injuries and in low-energy accidents related to pathologic bone, such as with osteoporosis or metastatic bone illness. The fractured limb should be intently examined to avoid missing any open wounds, particularly within the posterior facet of the thigh. Skin abrasions and apparently minor wounds must be assessed to determine if they impart with the fracture.
Syndromes
The expected result of nonoperative therapy is improved signs in 6 weeks erectile dysfunction drugs don't work 160 mg super viagra discount amex, with return to full activities by three months erectile dysfunction doctor san diego super viagra 160 mg buy cheap on-line. These may characterize loose our bodies or an unstable torn meniscus (ie erectile dysfunction after radical prostatectomy treatment options 160 mg super viagra discount visa, bucket-handle tear), which may cause significant articular injury if left untreated. With all meniscus pathology, the aim is to protect as much meniscus as attainable. Repair versus resection the potential long-term good factor about repairing the meniscus is chondroprotection. The surgeon ought to contemplate tear location, sample, vascularity, and related pathology when determining whether or not to restore or resect the meniscus. When resection is performed, all efforts ought to be made to preserve as much viable meniscus as potential. The meniscosynovial junction must be preserved because that is the place the circumferential collagen fibers kind the predominant amount of "hoop stresses. The healing potential for a meniscus repair at the side of an anterior cruciate ligament reconstruction is far superior to that of a repair alone. The surgeon should discuss with the affected person the risks and advantages of the surgery in addition to the precept of informed consent. All sufferers ought to be apprised of the potential of meniscus resection versus restore. They should understand the implications of every in terms of short- and long-term penalties and postoperative rehabilitation protocols. This could also be a very crucial conversation with an elite athlete who would prefer to undergo a resection in an attempt to return to aggressive sport quicker. The anesthesia used is usually selected by the anesthesiologist and orthopedist before entering the working room. We prefer to have the anesthesiologist present sedation in conjunction with an area anesthetic administered by the surgeon. About 30 to forty cc is injected intra-articularly, and about 5 cc is injected into each portal website. The two most popular strategies of leg support are a knee holder (thigh immobilizer) and a lateral post. The knee holder must be positioned perpendicular to the place of the femur at a degree above the patella and portals that permits for a valgus drive on the knee. The finish of the desk is dropped down under 90 degrees from horizontal to allow both legs to grasp freely from the knees. The lateral post should be positioned above the patella and angled outwardly to enable for a valgus pressure on the operative knee. The surgeon ought to verify that the knee could also be taken by way of a variety of motion by abducting the leg in opposition to the lateral post with flexion of the knee off the facet of the desk. Preoperative Planning Before the surgery, all radiologic studies should be reviewed. The knee should be examined under anesthesia earlier than beginning the surgical procedure in an try to detect related pathology. Padding of the contralateral leg is used to forestall pressurerelated injury to the bony prominences or superficial nerves. The superomedial portal is usually made proximal to the superior pole of the patella in line with the medial border of the patella (medial to the quadriceps) and is directed in an indirect manner into the joint. The anterolateral portal is created by making a small (about 6 mm) stab incision 1 cm proximal to the joint line and 1 cm lateral to the patella tendon. The anteromedial portal is taken into account the working portal for insertion of instruments. It is often made beneath direct visualization by inserting a spinal needle into the medial "gentle spot" 1 cm medial to the patella tendon and 1 cm proximal to the joint line. Rasping may be carried out with either an arthroscopic shaver or a meniscal rasp that lightly abrades both the tibial and femoral edges of the tear website, in addition to the meniscosynovial junction, to stimulate vascularity. Trephination is carried out by inserting a long 18-gauge needle both percutaneously or through the arthroscopic portals across the meniscus tear to create vascular channels. The surgeon should keep away from perforation of the meniscus surface, causing additional injury. It is greatest used for posterior horn, center third, peripheral capsule, and bucket-handle tears. Before passage of the sutures, an incision is made posteromedial or posterolaterally to capture the needles as they exit via the capsule. For passage of a needle by way of the medial compartment, the knee is placed in 20 to 30 degrees of flexion to avoid tethering the capsule. A 4- to 6-cm posteromedial incision is made just posterior to the medial collateral ligament, extending about one-third above and two-thirds beneath the joint line. Dissection is sustained anterior to the sartorius and semimembranosus musculature, deep to the medial head of the gastrocnemius. The posterolateral incision is made with the knee in ninety levels of flexion to allow the peroneal nerve, popliteus, and lateral inferior geniculate artery to fall posteriorly. A 4- to 6-cm incision is made simply posterior to the lateral collateral ligament, anterior to the biceps femoris tendon, extending one-third above and two-thirds below the joint line. Dissection is continued between the iliotibial band and the biceps tendon after which proceeds deep and anterior to the lateral head of the gastrocnemius. On exposure of the capsule, a "spoon" or popliteal retractor is positioned towards the capsule to visualize the exiting needles. A single- or double-lumen cannula is handed through the arthroscopic portals to the location of the tear. Long flexible needles are then passed via the cannula, piercing the meniscus above and below the tear web site and creating vertical mattress sutures. Care is taken to not pull both suture throughout until each needles are passed. The sutures are then tensioned and tied to the capsule while viewing the repair arthroscopically. This approach is finest performed on tears of the anterior and center third, as properly as radial tears. The needle should enter the joint through the periphery to achieve a vertical or horizontal mattress suture configuration. A second needle with a wire retriever trocar is handed by way of the tear to retrieve the suture. After tensioning of the mattress suture, a 3- to 5-mm pores and skin incision is made near the suture strands and blunt dissection carried all the method down to the capsule with a hemostat. A probe may be used to retrieve the sutures and tie them all the means down to the capsule underneath direct visualization, taking care to keep away from incarceration of any neurovascular constructions. These units are finest utilized in vertical longitudinal tears in the red-white zone of the posterior horn. They are typically made from bioabsorbable copolymers such as poly-L-lactic acid and poly-D-lactic acid. After identification of the tear website, correct measurement of the size of the meniscus is carried out with an arthroscopic measuring gadget. Insertion of the fixator must be performed perpendicular to the tear and parallel to the tibial floor. The suture fixators are designed to allow restore of the meniscus with mattress sutures with out creating an incision through the pores and skin. The units deploy two absorbable or nonabsorbable suture anchors with hooked up nonabsorbable sutures between them. The sutures can then be arthroscopically tied or they might come pretied, depending on proprietary design. After preparing the tear in the standard method, the fixator should be inserted from the contralateral portal. Use of a curved needle provides the surgeon with extra choices compared to the straight needle with regard to place and discount and insertion angles. Insertion of the needle through a sheath or insertion cannula prevents the delivery system from getting caught on free tissue.
Continuous passive motion is began immediately after surgical procedure erectile dysfunction causes in early 20s super viagra 160 mg discount with mastercard, from 0 to forty five degrees of flexion erectile dysfunction treatment methods 160 mg super viagra purchase, and is elevated by 10 degrees per day erectile dysfunction doctors raleigh nc buy super viagra 160 mg overnight delivery. From the primary postoperative day, sufferers are allowed full weight bearing as tolerated. Non-cutting and non-twisting sports such as swimming, biking, and running in a straight line are allowed at 12 weeks after surgery. Several short-term studies and a number of prospective research at present are ongoing in Japan, France, Italy, and the United States. Rotational stability was achieved in each affected person, as demonstrated by a negative pivot shift. Preliminary results have shown earlier return to full extension and symmetric flexion to the contralateral knee by 3 months after surgery. Thus far, no significant tunnel enlargement has been discovered; however, follow-up has been short-term only. Two-bundle reconstruction of the anterior cruciate ligament utilizing semitendinosus tendon with endobuttons: operative approach and preliminary outcomes. Functional anatomy of the anterior cruciate ligament and a rationale for reconstruction. The effectiveness of reconstruction of the anterior cruciate ligament with hamstrings and patellar tendon: a cadaveric research comparing anterior tibial and rotational loads. Anatomic reconstruction of the anteromedial and posterolateral bundles of the anterior cruciate ligament utilizing hamstring tendon grafts. Reconstruction of the anterior cruciate ligament of the knee utilizing a doubled tendon graft. Two failures had been sustained throughout contact injuries while playing collegiate football. The third occurred in a noncompliant affected person three months after reconstruction when she returned to enjoying highschool basketball with no brace. Bell et al2 carried out biomechanical and computer modeling research comparing single and double femoral tunnels and the danger of femoral condyle fracture. Results of these studies have proven that fracture risk increased considerably for the single tunnel versus the native condyle process, however no vital improve in fracture danger was found for one versus two tunnels. It is commonly thought that sufferers who proceed to expertise episodes of instability place the knee susceptible to further damage to the articular cartilage and menisci. While it could be possible for some sufferers to keep away from actions that lead to instability, others may proceed to take part in sports, and still others might experience episodes of instability with actions of daily dwelling. Secondary restraints to anterior translation of the tibia include the medial collateral ligament, the posterior horn of the medial meniscus, and the posterior facet of the capsule. Posterolateral instability might contain injury to the popliteus tendon and the popliteofibular and lateral collateral ligaments, and may require restore, advancement, or reconstruction of those buildings. It also is useful to know the time from the initial injury to the index reconstruction. An explanation of the postoperative remedy program and progress must be obtained, and any traumatic episodes after surgery should be famous. A copy of the operative report from the earlier restore should be obtained from the primary surgeon to notice graft kind, tunnel placement, fixation methods and materials, and situation of the articular surfaces and menisci at the time of that process. An antalgic gait might recommend persistent ache after surgery, or a current second traumatic event. A varus thrust throughout gait is extremely suggestive of incompetence of the lateral or posterolateral constructions and requires further analysis with long-film standing anteroposterior radiographs for mechanical alignment. Buckling of the knee, particularly within the preliminary phase of gait, may recommend quadriceps weak spot, and should give the affected person the subjective sensation of knee instability. Any decreases may counsel an initial dislocation of the knee and require acceptable workup to rule out a vascular damage. Common examinations to decide instability patterns of the knee include: Anterior drawer take a look at. Opening in 30 levels of flexion is in maintaining with harm to collateral ligaments alone. If opening in both zero and 30 levels, harm to collateral ligaments and different buildings, such as the cruciate ligaments or capsule, is sometimes recommended. It typically is troublesome for the affected person to loosen up within the setting of a painful knee, nonetheless. Increased posterolateral translation compared with the intact, contralateral knee might suggest posterolateral rotatory instability. The varus recurvatum take a look at reveals varus angulation, hyperextension, and exterior rotation of the tibia. Testing for concurrent intra-articular injuries ought to be performed to detect potential meniscal, articular cartilage, or patellofemoral pathology. In the revision setting, these images allow for crucial assesment of earlier tunnel placement and assesment for possible bone loss at previous tunnels, which may require further analysis and treatment. Metallic fixation gadgets could create significant artifacts on each of these imaging strategies, at times limiting their usefulness. Bone scan and serologic checks, together with full blood rely, erythrocyte sedimentation rate, C-reactive protein, and bacterial cultures of knee aspirates, should be performed in any setting suggestive of an infection, including these instances with vital osteolysis of earlier tunnels. In the setting of potential posterolateral rotational instability, varus malalignment, or vital bone loss requiring bone grafting, the patient must be conscious of the attainable want for staged procedures, and the required postoperative course should this turn into the case. Once anesthesia has been induced, a radical examination of the knee as in comparison with the contralateral extremity is important. Strengthening the dynamic stabilizers of the knee, such because the hamstrings (an antagonist to anterior translation of the tibia) might increase stability of the knee for routine actions. Bracing Approach A standard superolateral outflow and anteromedial and anterolateral portals are used for diagnostic arthroscopy. These embrace repair or d�bridement of meniscal tears, removing of free bodies, d�bridement with attainable microfracture of osteochondral lesions, and hardware removal, if necessary. A preoperative plan should include evaluation of the knee based on historical past, examination, and imaging for attainable different intra-articular pathology, similar to meniscal tears or cartilage lesions. The surgeon should be ready to address these comorbidities on the time of revision surgical procedure. After completion of the arthroscopic inspection of the knee and therapy of another intra-articular pathology, the tourniquet is inflated. The shaver also is used to remove any fats pad obstructing the view, periosteum off the lateral wall of the notch, and any scar tissue present within the notch. Careful consideration to localizing the posterior wall is important, particularly as a end result of the sides and roof of the notch typically are irregular owing to the earlier surgery. A curved curette is used to take away a small area of bone to localize the desired position of the new femoral tunnel. A tougher situation is the scenario where the femoral tunnel was properly positioned. We have found that transtibially placed femoral tunnels usually may be revised by drilling the revision tunnel by way of the anteromedial portal. Likewise, if a previously well-placed femoral tunnel was positioned by way of the anteromedial portal, it typically can be revised by drilling transtibially. A thin layer of periosteum is well visualized on the posterior wall of the notch. The femoral tunnel for the revision may be placed on the applicable location without removing the interference screw used in the major procedure. The new femoral tunnel and interference screw are placed in the applicable location without compromise from the screw used within the index process. View of femoral notch after placement of femoral tunnel and interference screw by way of anteromedial portal. Both bone plugs are reduce to a size of 25 mm, with a peak of 10 mm and width of 10 mm utilizing a micro oscillating noticed. A 2-mm drill is used to drill one hole between the proximal two thirds and the distal one third of the bone plug from the patella. Two related holes are drilled in the tibial bone plug at one- and two-thirds the length of the plug, at a 90degree angle to one another.
Great warning ought to be exercised in sufferers with a history of earlier knee trauma or dislocation impotence pump medicare super viagra 160 mg cheap with amex, as a result of the anatomy of the nerve may be aberrant impotence natural supplements 160 mg super viagra free shipping, which may result in erectile dysfunction grand rapids mi buy super viagra 160 mg with amex iatrogenic nerve harm during surgical approach and manipulation. Careful retroperitoneal decompression because of the proximity of the deep circumflex iliac artery Careful initial dissection, as a outcome of nerve can easily be mistaken for fats Recognize that the nerve may be extra superficial than expected: with a history of trauma, it tends to be more anterior and superior. Careful dissection with applicable magnification and instruments If a nerve decompression was carried out, early mobilization ought to be encouraged. If nerve reconstruction was performed, restricted ambulation or immobilization is advised. Effect of submuscular versus intramuscular placement of ulnar nerve: experimental mannequin in the primate. Part 2 Chapter 1 Chapter 2 Pelvis and Lower Extremity the Knee Trauma External Fixation of the Pelvis 462 Open Reduction and Internal Fixation of the Symphysis 476 Chapter three Open Reduction and Internal Fixation of the Sacroiliac Joint and Sacrum 487 Chapter 4 Open Reduction and Internal Fixation of the Posterior Wall of the Acetabulum 503 Chapter 5 Open Reduction and Internal Fixation of Femoral Head Fractures 514 Chapter 6 Open Reduction and Internal Fixation and Closed Reduction and Percutaneous Fixation of Femoral Neck Fractures 521 Chapter 7 Cephalomedullary Nailing of the Proximal Femur 533 Chapter eight Open Reduction and Internal Fixation of Peritrochanteric Hip Fractures 547 Chapter 9 Retrograde Intramedullary Nailing of the Femur 558 Chapter 10 Anterograde Intramedullary Nailing of the Femur 569 Chapter 11 Open Reduction and Internal Fixation of the Distal Femur 582 Chapter 12 Open Reduction and Internal Fixation of the Patella 604 Chapter thirteen Open Reduction and Internal Fixation of the Bicondylar Plateau 613 Chapter 14 Lateral Tibial Plateau Fractures 622 Chapter 15 External Fixation of the Tibia 629 Chapter sixteen Intramedullary Nailing of the Tibia 642 Chapter 17 Peroneus longus Fibula Interosseous membrane Tibia Fasciotomy of the Leg for Acute Compartment Syndrome 660 Chapter 18 Flexor hallucis longus Open Reduction and Internal Fixation of the Pilon 671 Chapter 19 the Knee Open Reduction and Internal Fixation of the Ankle 687 Chapter 20 Open Reduction and Internal Fixation of the Talus 697 Chapter 21 Surgical Treatment of Calcaneal Fractures 712 Chapter 22 Open Reduction and Internal Fixation of Lisfranc Injury 724 Chapter 23 Open Reduction and Internal Fixation of Jones Fracture 734 Chapter 1 External Fixation of the Pelvis Stephen Kottmeier, John C. Pelvic external fixation can serve a number of different purposes depending on hemodynamic and pelvic structural instability. Early external fixator software throughout resuscitative acute part management can serve to control intrapelvic hemorrhage. It might, nevertheless, show insufficient in reaching long-term goals in the absence of additional surgical stabilizing efforts. With certain rotationally unstable but vertically stable patterns, exterior fixation of the pelvis might serve as definitive administration. The pelvis affords safety and passage for genitourinary, gastrointestinal, and neurovascular structures. Life-threatening massive hemorrhage, a complication of pelvic damage, may be of arterial (branches of the iliac system), venous plexus, or fracture surface origins. Additional considerations when treating pelvic ring trauma include harm to the lumbosacral and coccygeal nerves and male urethra. The anterior portion of the pelvic ring assumes minimal weight-bearing operate and affords little pelvic ring stability. Ligamentous, somewhat than osseous, assist is the sole source of stability to the pelvis. Stability of the pelvis is especially depending on the tension band of the posterior weight-bearing sacroiliac complicated (comprising the anterior sacroiliac ligaments, the interosseous ligaments, and the posterior sacroiliac ligaments) in addition to the iliosacral ligaments throughout the pelvic floor (sacrospinous and sacrotuberous). The iliolumbar ligaments confer extra stability between the axial skeleton (L5 transverse process) and the hemipelvis (ilium). Anteroposterior compression and hemipelvic rotational forces tend to result in harm to the "anterior ligamentous" complicated (severity order: symphysis pubis, ischiosacral ligaments, anterior sacroiliac ligament). Depending on the severity of harm to the anterior ligamentous complicated, rotational instability could ensue. Lateral compression injuries, depending on severity, may end in inside collapse of the pelvis. Osseous injuries both anteriorly and posteriorly are usually secure impaction variants. Occasionally inner rotatory instability is sufficient to warrant surgical stabilization (external or inner fixation). Vertical instability implies disruption of the posterior tension band of the pelvic ring. Division of the sacrospinous and sacrotuberous ligaments within the presence of intact posterior ligaments will render a pelvis rotationally unstable. Further division of the posterior ligaments of the sacroiliac complicated will result in both rotational and vertical instability. Any injury mechanism (anteroposterior compression, lateral compression, vertical shear) could lead to full (vertical and rotational) instability if the magnitude of drive is adequate. Early sheeting (circumferential external compression) might supply an preliminary beneficial hemodynamic response. Suspected sustained hemorrhage of indeterminate source may be intrapelvic arterial in origin. Exploratory laparotomy, from the standpoints of function and timing, remains controversial. Imaging findings, results of diagnostic peritoneal lavage (if indicated), and response to fluid resuscitation should be thought of before exposing the unstable trauma sufferer to the potential negative results of belly exploration (decompression of intrapelvic tamponade, amongst others). Pelvic fractures related to violation of the perineal, rectal, or vaginal regions have to be recognized immediately, and early measures directed toward stopping regional and systemic sepsis must be implemented. Appropriate soft tissue administration requires early aggressive d�bridement and restoration of pelvic stability to facilitate wound care. External fixation is of paramount significance in plenty of such instances, as is diverting colostomy. Applied forces may be simplified into anteroposterior compression, lateral compression, and vertical shear. Resultant instability patterns are categorized as (1) vertically and rotationally secure, (2) rotationally unstable and vertically steady; and (3) rotationally and vertically unstable. In addition to compromise to the "anterior ligamentous complicated," the integrity of the posterior pressure band is disrupted. Emergency discount for pelvic ring disruptions and control of related hemorrhage using the pelvic stabilizer. Pelvic discount with restoration of stability and occasionally neurologic decompression might afford a extra favorable prognosis if correctly indicated and executed. Lower extremity limb-length inequality and rotational deformity might end in functional deficits. Anterior ring accidents with significant displacement (tilt fragments) may end up in sexual dysfunction, significantly in females. This dictates, respectively, the hemodynamic response and the energy of injury required to generate sure pelvic ring accidents. Preexisting medical comorbidities should be ascertained, as they might have appreciable impression on survivability and problems associated with both operative and nonoperative management of pelvic injuries. Pelvic ring disruption is commonly accompanied by potentially life-threatening accidents to organs, vessels, and nerves inside the pelvis, as properly as other extrapelvic and closed cavity lesions of the stomach, thorax, and head. Adequate adherence and response to rules of resuscitation must be assessed and first and secondary surveys completed. Clinical evaluation consists of inspection for abrasions, contusions, limb-length discrepancy, or irregular rotation of the decrease extremities. Palpation and guide testing for instability patterns could additionally be pursued with caution. Identification of any open fracture variants and those with rectal or vaginal continuity is necessary, as mortality charges within the presence of such lesions are appreciable. Further scientific examination or imaging of the limb is warranted if asymmetry is of other than pelvic origin. Assessment of pelvic instability Lateral compression injury is implied by inner rotation and shortening. Neurologic assessment to identify deficits in voluntary sphincter management or perianal sensation. In the hemodynamically unstable patient, this picture alone is adequate to permit implementation of therapy. This view alone (particularly in the presence of hemodynamic instability) could additionally be used to confirm the presence of pelvic instability and provide indication for pelvic exterior fixation. The x-ray beam is directed caudad at forty five levels to the vertical axis centered on the midpelvis. The x-ray beam is directed cephalad at forty five degrees to the vertical axis centered on the midpelvis (perpendicular to the sacrum). Posterior pelvic displacement of more than 1 cm suggests posterior pelvic disruption. Longitudinal load and traction are sequentially imparted to the decrease extremity of the concerned hemipelvis with handbook stabilization of the contralateral extremity. Such maneuvers are contraindicated in the presence of lumbosacral plexopathy, hemodynamic instability, or ipsilateral lower extremity fractures. Sacral foraminal and central spinal canal involve- ment is confirmed, as is integrity of the posterior pressure band.






