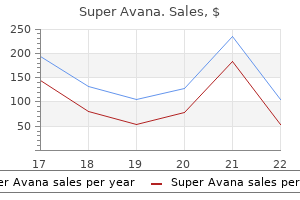
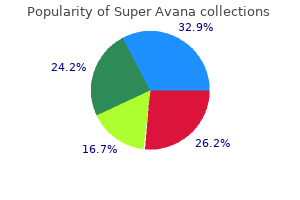
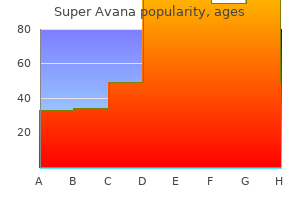
Super Avana
Super Avana
Super Avana dosages: 160 mg
Super Avana packs: 4 pills, 8 pills, 12 pills, 24 pills, 36 pills, 60 pills, 88 pills, 120 pills

The form and thickness of the plaque erectile dysfunction causes prescription drugs super avana 160 mg fast delivery, partially erectile dysfunction treatment brisbane super avana 160 mg generic otc, contribute to the chance of embolization erectile dysfunction world statistics 160 mg super avana discount. Thicker plaque embolizes more readily than thinner plaque, particularly plaque greater than four mm in thickness. These findings have been later supported in subsequent studies including the French Study of Aortic Plaques in Stroke Group. A potential clarification for this finding is that thicker plaque tends to be extra lipid-laden with overlying thrombi, each of which increase the possibility of embolization. Clinical manifestations rely upon the arterial phase affected by embolic disease. Emboli originating from the ascending aorta or arch are more likely to result in cerebral or higher extremity emboli. Therefore, such sufferers will current with transient ischemic assaults or stroke symptoms and upper extremity ischemia, respectively. Descending thoracic aortic emboli may lead to visceral, renal, or distal extremity emboli. Many sufferers show diffuse aortic thombus without embolic episodes; shaggy aorta syndrome analysis due to this fact requires the mix of both clinically evident embolic episodes as properly as ulcerated lesions on imaging studies. Thromboembolic disease from a shaggy aorta may cause peripheral ischemia, renal failure, bowel infarction, and pancreatitis, among many additional scientific manifestations. In their experience, management options with the bottom morbidities and mortalities concerned surgical restore including extra-anatomic bypass with ligation of the distal exterior iliac arteries. The formation of thrombus and atheroma inside aortic aneurysms are a potential source of both visceral/mesenteric in addition to peripheral emboli. Thromboembolism is the extra common type, and it arises from thrombus that overlies an atheromatous plaque within the aorta or a big artery. Focal aortic thrombus is eccentrically located inside the descending thoracic aorta. The superior mesenteric artery seems extensively patent on imaging prior to the acute event. Noninvasive imaging with pulse quantity recordings show dampening of the left above- and below-knee waveforms consistent with femoral-popliteal disease. Angiogram demonstrates an abrupt cutoff of the profunda in addition to a distal superficial femoral artery occlusion. However, case reviews suggest that speedy enlargement, which may occur with inflammatory and mycotic aneurysms, can dislodge thrombus. In sufferers with severe atherosclerosis of the ascending aorta, atheroemboli were found in 22% of postcardiac surgical procedure post-mortem instances. Atheroemboli, mostly from the belly aorta, include atheromatous plaque fragments containing ldl cholesterol crystals in addition to platelet and fibrin thrombi, which lead to a bathe of microemboli. The microembolic fragments cause an inflammatory reaction in addition to mechanical occlusion, which in combination can result in ischemia, necrosis, and/or infarction. Cholesterol emboli can also be liberated in aortic inflammatory situations, together with cases of Behcet syndrome, retroperitoneal fibrosis, aortitis syndrome, and bacterial infections. It has been reported after placement of an intra-aortic balloon pump, percutaneous coronary intervention, percutaneous transluminal angioplasty, and thoracic/abdominal aortic stent placement. There is eccentric aortic thrombus proximal to thrombus throughout the superior mesenteric artery (see arrowhead) Focal thrombus is also present on the level of the renal arteries with multiple right-sided renal infarctions. A shaggy aorta consists of multiple ulcerated atherosclerotic plaques, which may act as a source of spontaneous atheromatous embolization. Jones and Iannaccone14 even described a 1% incidence of atheromatous emboli within the setting of a renal biopsy. The analysis is predominantly medical, but a definitive prognosis may be made by muscle, pores and skin, or renal biopsy. The association between anticoagulation and atheroembolic disease was first described by Feder and Auerbach in 1961. The cessation of low-molecular-weight heparin has been related to the advance in clinical manifestations of atheroembolism. Of the 25 patients, 48% introduced with cutaneous indicators, whereas 64% had renal insufficiency. This further complicates the decision point of stopping or persevering with anticoagulation in the setting of scientific manifestations of atheroembolism with proof available to support each programs of motion. Liew and Bartholomew20 concluded that based mostly on the restricted data, clinicians should continue anticoagulation in the setting of "compelling indications. Cholesterol emboli originating in each the thoracic and stomach aorta may lead to renal failure, bowel ischemia, myocardial infarction, stroke, limb ischemia and emboli to the skeletal muscle tissue and pores and skin. The most commonly affected organs are the pores and skin and the kidneys, and the association of renal and cutaneous disease should immediate additional investigation for atheroembolic disease. Although gastrointestinal manifestations are thought to be widespread, they rarely current clinically. Overall the prognosis is poor both for the restoration of renal perform in addition to overall affected person mortality. The clinical presentation contains acute renal failure usually in combination with eosinophilia. Lastly, this prospective examine also demonstrated an in-hospital mortality of 16% and located that renal dysfunction was present in all the deadly outcomes. It has been instructed that hypocomplementaemia might provide some assistance in distinguishing between these entities as a outcome of this condition could be seen within the setting of ldl cholesterol embolism however is rare in systemic vasculitis. The ldl cholesterol crystal is assumed to obstruct the arteriole lumen and incite a neighborhood granulomatous response with subsequent inflammation, endothelial harm, and intimal proliferation. Cholesterol crystal embolization may be secondary to aortic manipulation, anticoagulation, or spontaneous embolization from an atherosclerotic plaque. Even more alarming, of the cases thought to be "probable" for atheroembolism, the mortality fee was over 50%. The pathophysiology is a delay in superficial venous drainage caused by the obstruction of capillaries and venules by ldl cholesterol emboli. Patients current with cyanotic, cool, and painful toes with palpable distal pulses. The cyanosis is more outstanding in dependent leg areas, typically with asymmetrical presentation if both extremities are involved. The degree of severity is decided by the diploma of microvascular obstruction with tissue necrosis, ulceration, and gangrenous modifications present in essentially the most severe instances. These photos show microvascular ischemia, blue toe syndrome, in a patient with palpable distal pulses. Microembolic Sources: Additional Sequelae of Atheroembolism Atheroembolism can also present with gastrointestinal, central nervous system, and pulmonary manifestations, although these are much less widespread than the cutaneous and renal shows. Gastrointestinal atheroembolic illness can present with bleeding, ache, or diarrhea, mostly involving the colon. Although rare, Moolenaar and Lamers36 also described acute inflammatory disease of each the pancreas and gallbladder from ldl cholesterol embolization. Atheroemboli to the central nervous system can current with cerebral infarction, retinal artery occlusion, or transient ischemic attack. Spinal wire infarction has been described and is usually related to iatrogenic causes. Dipyridamole and aspirin have been used in the setting of decrease extremity ischemia however no sturdy evidence supports their use with atheroembolic disease. Primary therapy options include reducing the risk elements for atheromatous embolization including blood stress control, the avoidance of hypercholesterolemia, and smoking cessation. Protection gadgets during endovascular intervention, stent placement within the setting of ulcerative atherosclerotic plaques, and open surgical restore are all potential treatment choices for sufferers with important atherosclerotic illness at risk for atheroembolism. Endovascular procedures could be a source of both thromboembolism and atheroembolism. Aortoembolic phenomena caused by dislodging of particles from the aortic wall might occur when a catheter or wire traverse an aorta containing atherosclerotic plaque. A prospective analysis by Keeley and Grines42 designed to quantify the aortic debris that exited the information catheter throughout its advancement around the aortic arch concluded that more than 50% of percutaneous revascularization procedures are related to scraping particles during guide catheter placement.
Syndromes
Normally less than 10 mm nodules are followed and biopsy undertaken only when progress traits are suspicious for malignancy erectile dysfunction caused by vasectomy 160 mg super avana cheap overnight delivery. Bronchial carcinoids constitute much less 25% of all carcinoids and 2% of all lung cancers erectile dysfunction 34 super avana 160 mg cheap on line. Typical carcinoid is slow rising regionally invasive tumor while atypical carcinoid is more aggressive and metastasizing tumor erectile dysfunction liver cirrhosis super avana 160 mg generic line. If the distal lung is aerated by collateral air drift, mucoid impaction (bronchocele) is seen which appear as elongated branching low density opacity. Some tumors, particularly atypical carcinoids, are seen as peripheral welldefined lobulated solitary pulmonary nodules. Bronchial carcinoids Small-cell lung cancer is a extremely malignant tobacco associated most cancers characterized by speedy growth and early metastases. It represents about 25% of all lung cancers and essentially the most aggressive hisotopathological subtype of lung cancer with poorest prognosis. These tumors secrete hormones, notably adrenocorticotrophic hormone, antidiuretic hormone and melanin stimulating hormone. Brain metastases are often symptomatic however; other websites are sometimes asymptomatic. Most primary tumors develop as small central tumor which rapidly unfold submucosally to contain vessels and lymphatics. The primary tumors are sometimes not separately visualized from disproportionate massive lymphadenopathy. Some of the tumors may not invade the bronchus and hence will not be visible on bronchoscopy. These are limited stage (disease in ipsilateral lung with unilateral or bilateral mediastinal nodes) and in depth stage (involvement of contralateral lung and/or distant metastases). Cyclophospha mide, etoposide or platinum-based chemotherapy regimens are generally used. Brain metastases are the identical old site of remedy failure and therefore, prophylactic mind irradiation is used to decrease the probabilities of mind metastases and enhance the survival. Non-small-cell lung carcinoma with sarcomatous components are classified as carcinosarcoma. On imaging, it reveals multiple nodular, flame-shaped or linear peribronchial opacities. Surrounding ground-glass opacities due to hemorrhages, lymphadenopathy and pleural effusions are also widespread. These come up from primitive blastomatous tissues and develop in pre-existing congenital lung lesions like cystic adenomatoid malformation, sequestration or bronchogenic cysts. Any cancer could cause lung metastases nevertheless, most common sources embrace breast, colon, kidney, uterus, prostate, head and neck in addition to most sarcomas. Various morphological patterns of lung metastases and the usual primaries associated with these are listed in Table. Osteosarcoma is the most typical explanation for calcified metastases; it may also be associated with calcified mediastinal lymph nodes and calcified pleural deposits. These may be associated with distal ground-glass opacities, infarction or lymphangitic involvement. Lung metastases are comparatively unusual in early cancers of head and neck and genitourinary tract. Similarly, in cancers of the breast, gastrointestinal tract and prostate, lung metastases are uncommon in absence of liver or bone metastases. Solitary pulmonary nodule detected in patients with head and neck cancers is extra more likely to characterize a model new major most cancers quite than the metastasis. On chest radiographs, lymphangitis carcinomatosis is seen as reticulonodular opacities with thickened septal lines. It is usually bilateral and symmetrical but could also be unilateral, especially in lung cancer. Subpleural bands and thickening of fissures because of subpleural edema is a useful sign within the analysis of lymphangitis carcinomatosis. Treatment of Lung Metastases Cancers during which resection of pulmonary metastases is useful embrace sarcomas (especially osterosarcoma), colorectal, urinary tract, testicular and head and neck cancers. Hence, this maneuver is essential to guarantee removing of all metastases through the surgical procedure. These could remain stable, turn into smaller or disappear fully and are no longer visible. Metastases from nonseminomatous germ cell tumors could enlarge regardless of responding efficiently to treatment. Variable response is common in a quantity of metastases and therefore, the sum of the diameters of enormous nodules (of diameter more than at least twice the slice thickness) is most accurate to quantify the response. With complete histopathological response, some metastases may persist in the form of fibrotic lesion with out viable tumor. Lymphomatous involvement of lung occurs in three distinct radiographic patterns; nodular, pneumonic and bronchovascular (lymphangitic). Lymphangitic kind outcomes from contiguous peribronchovascular unfold from hilar lymph nodes. Imaging features of these lymphomas are much like secondary lymphomatous involvement. Detectability of peripheral lung most cancers on chest radiographs: effect of the scale, location and extent of ground glass density. Real time ultrasound guided transbronchial needle aspiration for staging mediastinal lymph nodes. Endobronchial ultrasound reliably differentiates between airway infiltration and compression by tumor. Chest wall invasion by lung cancer: computed tomographic detection and results of operation. Prospective comparison of radiologic, thoracoscopic, and pathologic staging in patients with early non small cell lung most cancers. Survival in primary lung most cancers doubtlessly cured by operation: Influence of tumor stage and clinical traits. Interobserver variation within the computed tomographic evaluation of mediastinal lymph node dimension in sufferers with potentially resectable lung most cancers. The significance of cytologically negative pleural effusion in bronchogenic carcinoma. Non invasive staging of non small cell lung most cancers: A review of the present literature. Initial staging of non small cell lung most cancers: Value of routine radioisotope bone scanning. Impact of computed tomography-positron emission tomography fusion in staging patients with thoracic malignancies. Test performance of positron emission tomography and computed tomography for mediastinal staging in patients with non small cell lung most cancers: A meta-analysis. Staging of non small cell lung cancer with integrated positrom emission tomography and computed tomography. Clinical role of F-18 fluorodeoxyglucose positron emission tomography in patients with lung most cancers and suspected malignant pleural effusion. Positron emission tomography in non small cell lung most cancers: Prediction of response to chemotherapy by quantitative use of glucose uptake. Differentiation of pneumonia type bronchoalveolar carcinoma and infectious pneumonia. Determination of patient specific internal gross tumor volumes for lung most cancers utilizing 4 dimensional computed tomography. Feasibility of percutaneous radiofrequency ablation for intrathoracic malignancies: A massive single centre expertise. Radiofrequency ablation for remedy of medically inoperable stage 1 non small cell lung most cancers. Filling in of radiation therapy induced bronchiectatic change: A reliable sign of domestically recurrent lung most cancers. Early Lung Cancer Action Project: Overall design and findings from baseline screening. Bronchoplastic procedures in malignant and non malignant disease: Multivariate analysis of one hundred forty four circumstances. Clinical components related to suspected second main lung most cancers developments in sufferers with head and neck cancers. Long term outcomes of lung metastasectomy: Prognostic analysis based mostly on 5206 cases.
This anatomic bias displays the disparity in blood move in the base and apex of the lung in erect people erectile dysfunction cure video super avana 160 mg buy generic online. For the identical reason erectile dysfunction treatment new jersey purchase 160 mg super avana with visa, metastatic lesions occur more incessantly in lower lobes; a solitary mass in an upper lobe is unlikely to be metastatic erectile dysfunction doctors near me purchase super avana 160 mg otc. The predilection of tuberculosis for the lung apices has been attributed to this distinction in oxygen pressures. Pulmonary sequestration happens almost completely in the decrease lobes, most commonly within the posterior basilar phase and on the left aspect than the proper. Chronic idiopathic interstitial fibrosis and interstitial fibrosis of progressive systemic sclerosis are predominantly basal in distribution. Relative density can be a factor, since juxtaposed borders of comparable density will produce the signal and the borders of opacities that are markedly dissimilar is in all probability not obscured. Furthermore, there must be enough exposure to penetrate the margins of the buildings in question. The "hilus overlay" sign permits differentiation of true cardiomegaly from giant anterior mediastinal plenty. In the presence of an anterior mediastinal mass, the hilum is projected medial to the lateral border of the mass and in cardiomegaly the hilum is displaced laterally. The "hilus bifurcation signal" differentiates hilar lots from vascular structures in circumstances of hilar enlargement. If vessels are seen to arise instantly from the hilar shadow, the enlargement is vascular, if they appear to arise medial to the lateral facet of the hilar shadow, the enlargement is brought on by an extravascular mass. A well-defined mass seen above the clavicles is all the time posterior whereas an anterior mass being in contact with gentle tissues somewhat than aerated lung, is ill-defined. Line Shadows Linear opacities on a chest X-ray could be grouped on the idea of pathogenesis. Chapter 153 Basic Patterns of Lung Diseases 2521 Tubular Shadows (Bronchial Wall Shadows) the air column of the trachea, main bronchi, proper intermediate bronchus and left decrease lobe bronchus normally is seen on well-exposed radiographs. Where these structures are involved with air-containing parenchyma their partitions are also visible, their thickness being enough to forged a radiographic shadow. When tubular shadows are recognized exterior the hilar limits they constitute a definite signal of disease. Tubular shadows are double-line shadows that might be parallel or barely tapered as they proceed distally and always observe the bronchovascular distribution. Identification of a single line paralleling a vessel has the same significance as a tubular shadow. The most typical explanation for tubular shadows is bronchiectasis, by which the line shadows are roughly parallel and measure 1 mm or barely extra in width. The width of the air column separating them depends upon the severity of the bronchial dilatation. Since persistent bronchiectasis is commonly related to atelectasis, multiple tubular shadows may be crowded together. They could also be of unknown nature and pathogenesis at occasions and seen as isolated shadows in the best decrease lobe of adult patients of any age. The tubular shadows seen in chronic bronchitis have been attributed to an accompanying bronchiectasis. The double pleural line seen along both facet of the mediastinum in circumstances of mediastinal emphysema is created by the mixed thickness of parietal and visceral pleura displaced laterally by mediastinal gas. These linear opacities are associated with ailments that diminish diaphragmatic tour. After stomach surgical procedure varied factors mix to produce basal linear opacities (a) restriction of diaphragmatic excursion diminishes air flow of lungs, particularly within the bases (b) accumulation of bronchial secretions within the dependent portions of the lungs and obstruction of small airways (c) stagnation of secretions encourages the development of pneumonia with resulting inflammatory exudate obstructing the channels of interalveolar communication. Parenchymal Scarring A section of lung that was the site of infectious illness and has healed via fibrosis might present as a linear shadow. Healed upper lobe postprimary tuberculosis is a typical instance of this kind of linear shadow. The line shadow created by healed pulmonary infarction represents fibrous scarring secondary to lung necrosis. These linear shadows all the time prolong to a pleural floor and this can be brought on in part by an indrawing of the pleura by the scar. Radiological visibility of fissures not usually seen in a specific projection could level to otherwise invisible disease. For instance, when a decrease lobe loses volume, the upper portion of the main fissure sweeps downward and medially and becomes visible on frontal radiograph as an obliquely oriented shadow extending inferiorly and laterally from the lateral side of mediastinum above the hilum. Thickening of an interlobar fissure is caused extra typically by pleural edema than by pleural effusion. Since the pleural connective tissue layer is steady with the interlobular septa, edema fluid also collects in the subpleural space. Nodules A pulmonary nodule may be broadly outlined as any comparatively sharply defined, discrete, almost circular opacity within the lung, ranging in size from 2 to 30 mm. Nodules are normally additional characterised with respect to size, border definition, density, number and placement. Centrilobular nodules: these are distributed primarily throughout the center of the secondary pulmonary lobule. Centrilobular nodules range in size from a couple of millimeter to slightly greater than 1 cm and may be well-defined or ill-defined, relying on the underlying disease process. There are quite a few noninfectious disorders associated with the tree-in-bud sample. In allergic bronchopulmonary Aspergillosis, immunologic responses to the endobronchial development of aspergillus species leads to injury to the bronchial wall, central bronchiectasis and the formation of mucous plugs that comprise fungus and inflammatory cells. Bronchial wall irritation progresses to bronchiectasis and bronchiolar secretions result in a treein-bud pattern. This pattern can additionally be seen with aspiration of contaminated oral secretions or other irritant material, diffuse panbronchiolitis, obliterative bronchiolitis and asthma. Additionally, different findings are often present to assist in producing a sensible differential analysis. Pulmonary lymphatics are usually discovered inside the visceral pleura, inside the interlobular septa and alongside the veins and bronchovascular bundles, so illnesses involving the lymphatics could produce nodules in relation to these constructions. Because pulmonary lymphatics are current alongside brochovascular bundles, centrilobular nodules are generally additionally seen in ailments producing perilymphatic nodules; however, the nodules are predominantly found along interlobular septa and the visceral pleura and never inside the heart of the lobule. Nodules involve the subpleural interstitium in the lung periphery and adjacent to the fissure. Visualization of some interlobular septa, often anteriorly or along the mediastinal pleural surfaces, is normal, however visualization of numerous septa indicates an irregular situation. Thickening of interlobular septa may be seen in conditions related to dilatation of the pulmonary veins; infiltration of the pulmonary lymphatics; or with infiltration of the pulmonary interstitium by cells, fluid, or fibrosis. Smooth interlobular septal thickening is commonly seen with pulmonary edema and pulmonary alveolar proteinosis and in addition in lymphangitic carcinomatosis, lymphoproliferative illness, Pneumocystis jiroveci pneumonia and amylodosis. Occasionally, a parenchymal band represents a quantity of contiguous interlobular septa. Parenchymal bands have been reported to happen frequently in sufferers with asbestos publicity. Patchy subpleural reticular opacities are additionally seen Subpleural Lines A subpleural line is a curvilinear opacity, measuring less than 10 mm in thickness, that parallels the pleura. Subpleural traces are nonspecific and often symbolize atelestasis, fibrosis, or irritation. Subpleural lines were first described in patients with asbestosis and are seen extra generally in this disease. In certain medical circumstances, it can suggest a selected prognosis and it might possibly guide a bronchoscopist or surgeon to an applicable area for biopsy. In patients with lung transplants, Reticular Abnormalities Reticular opacities characterize linear opacities that intersect each other at numerous angles, producing a netlike pattern. It could also be attributable to pulmonary fibrosis or irritation within the absence of fibrosis. When underlying fibrosis is present, the reticulation typically appears coarse and traction bronchiectasis and architectural distortion may be seen. It can also be a standard finding in patients with nonspecific interstitial pneumonitis and pulmonary disease related to collagen vascular diseases. They are sublobular and should characterize opacification of single acini; hence the time period acinar nodules. With increasing consolidation, the nodules coalesce to kind bigger areas of opacity. Frequently, this extent of lung consolidation conforms to lobular boundaries, inflicting a "patchwork quilt" look.
An evaluation of 412 operations in nine collection demonstrated a crude patency rate of 70% to 85% erectile dysfunction cvs super avana 160 mg proven, although duration of follow-up and use of goal measures of graft patency various between the studies erectile dysfunction and testosterone injections purchase 160 mg super avana overnight delivery. One group discovered the 2-year major and secondary patency rates of thirteen bypass grafts (5 iliocaval and 8 femorocaval) to be 38% and 54% erectile dysfunction vitamin b12 order super avana 160 mg mastercard, respectively. Importance, etiology, and diagnosis of persistent proximal venous outflow obstruction. Endovascular management of continual disabling ilio-caval obstructive lesions: long-term results. Venous operate assessed during a 5 year period after acute ilio-femoral venous thrombosis handled with anticoagulation. Relationship between modifications in the deep venous system and the development of the postthrombotic syndrome after an acute episode of decrease limb deep vein thrombosis: a one- to six-year follow-up. High prevalence of nonthrombotic iliac vein lesions in chronic venous illness: a permissive role in pathogenicity. Use of compression stockings in continual venous disease: affected person compliance and efficacy. Venous leg ulcer: a meta-analysis of adjunctive therapy with micronized purified flavonoid fraction. Venous recanalization by metallic stents after failure of balloon angioplasty or surgery: four-year expertise. Revision of the venous clinical severity rating: venous outcomes consensus assertion: particular communication of the American Venous Forum Ad Hoc Outcomes Working Group. Whereas endovascular administration of iliocaval occlusion is efficient in many of those sufferers, the outcomes are less favorable than those for patients with major vein obstruction. Relationship between medical classification of continual venous illness and patient-reported high quality of life: results from an international cohort examine. Stenting of the venous outflow in persistent venous illness: long-term stent-related outcome, scientific, and hemodynamic end result. Surgical reconstruction of iliofemoral veins and the inferior vena cava for nonmalignant occlusive disease. Initially described as a cause of intestinal infarction by Elliot in 1895,1 mesenteric venous thrombosis is liable for 5% to 15% of all mesenteric ischemic events. Nonspecific symptomatology delays diagnosis and contributes to the poor outcomes associated with the condition, though improved imaging strategies have enabled extra rapid recognition and detection. Additionally, improved understanding of underlying disease mechanisms has improved both treatment and outcomes. Despite a imprecise medical presentation, the immediate recognition and aggressive treatment of this situation is necessitated by high morbidity and mortality charges related to intestinal infarction, bowel perforation, and high recurrence rates. Oral contraceptive use is liable for 4% to 5% of total mesenteric venous thrombotic occasions, a better percentage of circumstances occurring in young women. Direct Injury Direct damage is acknowledged as a predisposing condition for mesenteric venous thrombosis. These injuries embrace pancreatitis, inflammatory bowel disease, abdominal trauma, and postsurgical trauma. Primary mesenteric venous thrombosis is defined as spontaneous, idiopathic thrombosis of the mesenteric veins and accounts for approximately 25% of cases. Local Venous Stasis Conditions causing venous stasis within the mesenteric system embody cirrhosis, portal hypertension, severe congestive coronary heart failure, and morbid weight problems. These patients should be managed with lifelong anticoagulation to forestall recurrence. Additional hematologic hypercoagulable states related to mesenteric venous thrombosis embrace polycythemia vera, thrombocytosis, hyperfibrinogenemia, paroxysmal nocturnal hemoglobinuria, and myeloproliferative states. The location of acute thrombus formation could be an important predictor of the underlying explanation for mesenteric venous thrombosis. Intra-abdominal causes, similar to splenectomy and pancreatitis, provoke thrombus formation within the massive veins and spread peripherally. Hypercoagulable states usually result in thrombus formation within the vasa recta, arcuate veins, and venous arcades and progress to contain the larger veins. Even after the venous obstruction has been relieved, arterial vasoconstriction can persist, adequate to cause intestinal infarction and arterial thrombosis. Mesenteric ischemia usually presents with generalized midabdominal pain not defined by physical findings and is usually accompanied by vomiting, belly distention, and constipation. In these cases, onset of signs is sudden with colicky and severe pain, out of proportion to stomach findings on physical exam. More than half of sufferers report other nonspecific symptoms, such as nausea/vomiting, anorexia, and constipation with or without bloody diarrhea. In these sufferers with subacute mesenteric venous thrombosis, abdominal pain is the major finding without bowel infarction or variceal hemorrhage. Patients with continual mesenteric venous thrombosis have intensive venous collateral circulation and therefore much less abdominal ache. The prognosis is normally one of exclusion, after more widespread causes of belly pain, such as cholecystitis, pancreatitis, gastroesophageal reflux, and gastric issues, have been explored. These circumstances could demonstrate weight reduction, meals avoidance, and imprecise postprandial stomach ache. The differential diagnosis for acute mesenteric venous thrombosis is prolonged and consists of each intravascular and extravascular causes. Arterial causes embody embolic disease, occlusive/nononcclusive atherosclerotic disease, dissecting aortic aneurysm, hypoperfusion, and disseminated intravascular coagulation. Extravasular causes embrace incarcerated hernias, small bowel obstruction, volvulus, intussusception, and adhesive bands/scars. Patients with subacute or chronic mesenteric venous occlusion regularly have thrombosis of the portal and/or splenic veins, sparing the vasa recta and venous arcades. These patients current less acutely as a end result of venous collaterals provide enough venous drainage. Whatever the mechanism, occlusion of the mesenteric veins causes inadequate venous drainage of the bowel. Ischemic bowel becomes edematous and thickened with intramural hemorrhage, resulting in fast loss of fluid into the bowel lumen, mesentery, and peritoneal cavity. The elevated venous pressure leads to hemorrhage, perforation, and peritonitis. Metabolic acidosis or elevated lactate levels are late findings associated with bowel infarction. Findings on abdominal X-rays include dilated loops of small bowel with air-fluid levels indicative of small bowel obstruction or ileus, thickened loops of bowel or "thumbprinting" indicative of bowel wall edema, and pneumatosis intestinalis. B conditions together with portal hypertension and gallbladder disease, portomesenteric thrombosis could additionally be an incidental discovering. This modality has several limitations: its operator-dependent nature, restricted visualization due to overlying bowel gas or giant patient body habitus, and sensitivity to detect gradual circulate. The mesenteric veins could have thick, enhancing partitions and multivein occlusion is frequent. Bowel wall dilatation is a standard manifestation reflecting absence of peristalsis secondary to both arterial and venous perfusion abnormalities. Associated findings embrace stranding within the mesentery, collateral circulation, and ascites. Pneumatosis intestinalis, portomesenteric gasoline, and free intraperitoneal air are late findings of transmural infarction and perforation. In patients with chronic mesenteric venous occlusion, cavernous transformation of the portal vein, plentiful venous collaterals, gastroesophageal varices, and ascites could be recognized within the absence of intestinal ischemia. Additionally, "ectopic" varices within the small intestine, colon, and rectum can be identified. The primary aim of therapy is to avoid bowel infarction, peritonitis, and ischemia. In the absence of ongoing ischemia, oral anticoagulation with warfarin ought to be began and continued for 3 to 6 months or lifetime, depending on the underlying trigger. The use of anticoagulants in patients with continual mesenteric venous ischemia is controversial; although useful in stopping new thromboses, it carries the chance of exacerbating variceal hemorrhage. Surgical Management Acute mesenteric ischemia with evidence of bowel infarction or peritonitis is an indication for emergent surgical procedure. Intraoperatively, mesenteric edema and cyanotic discoloration of the bowel indicate mesenteric venous thrombosis.
Although the diagnosis is usually made on echo erectile dysfunction treatment vacuum constriction devices buy generic super avana 160 mg online, stagnant blood within aneurysm concavity might simulate a cystic tumor erectile dysfunction protocol guide buy super avana 160 mg low price. Both modalities are notably useful for demonstrating Pleuropericardial Cyst Though the most common pericardial mass lesion erectile dysfunction treatment edmonton super avana 160 mg discount without prescription, these are very rare, the reported incidence being 1:100,000 of the overall inhabitants. The commonest location is in the right cardiophrenic angle, although they could also be seen in left cardiophrenic angle and posterior mediastinum. Patients are usually asymptomatic, the lesion usually being detected by the way on imaging. In (B), the lesion reveals a quantity of massive sign voids, consistent with its vascular nature Intracystic septae could also be noticed following paramagnetic contrast agent administration. Right sided lesions are seen to increase into the chamber cavity and subendocardially, whereas the left sided lesions more usually grow subepicardially. The heart also could be secondarily affected by direct contact with hydatid cysts originating from the liver or the lung. These lesions are often asymptomatic, and incidental detection is reported in 47% sufferers in one examine. These modalities are primarily indicated for detection of extent of perivalvular invasion, together with abscess and/or fistula formation. In B, the typical hypointense rim to the lesion is seen could compress the cardiac cavity or may rupture leading to anaphylaxis, tamponade or pericardial constriction. The cysts could also be single or a number of, uniloculated or multiloculated, and thin or thick walled. More specific indicators embrace calcification of the cyst wall, presence of daughter cysts and membrane detachment. However, intensive infiltration of the myocardium, inseparable from pericardium and with the center showing literally "boxed in" has additionally been described. The lesion is often well-defined with a sharp define and without any move voids. A typical example is a excessive extending superior pericardial recess that will simulate an enlarged lymph node, vascular tumor or an aortic dissection. There is a homogeneous, well-marginated right atrial mass that has significantly reduced in size following therapy. It is crucial to differentiate between neoplastic, non-neoplastic and nonpathologic entities mimicking a mass, in order to avoid an inadvertent surgery. Although echo is universally accepted as the preliminary modality for evaluation of a suspected intracardiac mass, it has vital limitations. It is capable of simultaneously assessing their nature, extent and hemodynamic consequences. However, scanning time needs to be reduced by software program modifications in order to enhance picture high quality, get hold of diagnostic images in babies and fast coronary heart charges, and enhance affected person throughput. Adequate sedation stays a significant requirement for a profitable examination in a small youngster. The surgical therapy of 30 sufferers with cardiac myxomas: A comparability of scientific features according to morphological classification. Late enhancement of a left ventricular cardiac fibroma assessed with gadoliniumenhanced cardiovascular magnetic resonance. Sunray appearance on enhanced magnetic resonance image of cardiac angiosarcoma with pericardial obliteration. Malignant fibrous histiocytoma of the center: Case report and review of forty six cases within the literature. Visualization of Ventricular Thrombi With Contrast-Enhanced Magnetic Resonance Imaging in Patients With Ischemic Heart Disease. Ruptured sinus of Valsalva aneurysm difficult by myocardial ischemia: Pathogenetic mechanisms. Unruptured aneurysm of the left sinus of Valsalva extending into the left ventricular outflow tract: presentation and imaging. This illness most commonly entails the mitral valve, adopted by the aortic, tricuspid and pulmonary valves in this order. The resultant lesions may find yourself in stenosis, incompetence or both within the concerned valve. The goals of imaging in valvular illness irrespective of its etiology embrace the next: zz Diagnosis of the valvular disease: qualitative as properly as quantitative evaluation of all valves zz Assessment of the hemodynamic results of valvular illness on the pulmonary vasculature and ventricular operate zz Detection of related pulmonary pathologies as a complication or coincidental to heart disease, and zz Follow-up after remedy. The recent advances in imaging methods for noninvasive analysis of the cardiac illnesses have helped better delineate the anatomic location of the disease, and study the impact of the resultant structural abnormalities on the hemodynamic and practical penalties on the cardiovascular system. These have also gone a great distance in an improved understanding of the pure history of the illness processes. It provides useful details about the cardiac dimension, pulmonary vasculature, arterial and venous hypertension, and the secondary adjustments within the lungs. Echocardiography is a useful screening technique that permits realtime analysis of every cardiac chamber in multiple orthogonal planes. It is noninvasive, simply obtainable, provides a direct visualization of cardiac valves and likewise helps evaluate the attendant functional disturbances on the cardiac chambers. The stenosis and regurgitation, as properly as the resultant derangement of ventricular perform, including the scale of the chamber, wall thickness, dimension of valvular orifice, trans-stenotic strain gradient or the regurgitant volume, may be reliably estimated by quantitative methods. The published reviews counsel that the results compare favorably with the data obtained at cardiac catheterization and angiocardiography. It helps assist the analysis and outline the impression of the illness on the pulmonary vasculature. It is also helpful in the evaluation of the effect of therapy in a given affected person. This method is easily and broadly available, and offers a reproducible and a permanent report of the patient. The chest radiographic abnormalities in numerous disease states are described beneath. Heart dimension is normal or minimally enlarged in stenotic lesions whereas it shows a reasonable or extreme enlargement in regurgitant lesions. Subtle cardiac enlargement in aortic stenosis is better detected on the lateral movie and with volumetric measurements. If one also takes into account different parameters of cardiac configuration, the false-negative rates are reduced to only 5%. The presence of calcification in the aortic valve is localized primarily based 2848 Section 6 Chest and Cardiovascular Imaging on its characteristic location and motion. These changes have been discussed earlier and have been shown to bear a rough correlation with the stress values obtained at cardiac catheterization. Valvular calcification, usually seen on fluoroscopy, strongly suggests a rheumatic etiology. In distinction, mitral annular calcification is often seen in age-related degenerative disease and in the postoperative affected person after closed mitral valvotomy. Associated Pulmonary Pathologies A plain chest radiograph is useful in assessing most abnormalities of the lungs in a patient with valvular coronary heart disease. Various lung pathologies, if present, can simulate or worsen the symptoms in these sufferers. These embody pulmonary tuberculosis, persistent airway obstructive illness, interstitial lung disease, and pneumonia among others. This chamber is most difficult to assess by plain chest radiography, especially when the other chambers are also enlarged. Since valvular coronary heart illnesses typically run a protracted course and most patients lead a close to normal life after surgical or different intervention, their follow-up requires close monitoring. Echocardiogram is finest fitted to this purpose as a result of it can exactly quantify the hemodynamic results of the valvular lesions. Chest radiographs are additionally useful for a prepared comparison of the heart measurement and the status of the pulmonary vasculature. Once the diagnosis has been established, the affected person could be followed-up by monitoring the guts dimension. Similarly, a postoperative reduction in heart dimension serves as an excellent indicator of profitable outcome.
Harongarinde bark (Haronga). Super Avana.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96593
Steno-occlusive hepatic artery complications symbolize over 95% of arterial complications of the hepatic artery after liver transplantation erectile dysfunction clinic 160 mg super avana cheap amex. Hepatic artery stenoses are classified based on erectile dysfunction young cure discount super avana 160 mg online their location and multiplicity erectile dysfunction natural cures 160 mg super avana purchase visa. In truth, hepatic graft dysfunction can characterize a myriad of posttransplant hepatic graft complications, such as all vascular issues, biliary abnormalities, graft rejections, graft ischemia not related to anatomic vascular defects, and important infections/sepsis. Hepatic Venous Outflow Surgical Anatomy the hepatic graft venous outflow includes the hepatic veins proper and the donor and/or recipient vena cava. Demonstrates straightforward end-to-end recipient hepatic artery to graft hepatic artery anastomosis. Demonstrates an end-to-end recipient gastroduodenal artery to graft hepatic artery anastomosis. Demonstrates an end-to-side recipient splenic artery to graft hepatic artery anastomosis. Demonstrates an end-to-end recipient replaced hepatic artery, which is off the recipient superior mesenteric artery to graft hepatic artery anastomosis. Such a examine would be troublesome to design, hard to implement, and require massive topic numbers involving a number of facilities enrolling examine subjects over years. This is due to the relative rarity of the complication and the quite a few surgical, anatomic, medical, and transplant-related variables that need to be thought-about for a complete end result evaluation. In addition, detailed surgical anatomic terminology for the hepatic artery is provided (C). Proximal to the surgical anastomosis (anastomosis) is the native (N) or recipient vasculature. Distal to the surgical anastomosis (anastomosis) is the donor or graft (G) vasculature. The graft (G) hepatic artery is subdivided into the extrahepatic hepatic artery (a) and the intrahepatic/branch hepatic arteries (b). This is opposite to the findings of an anecdotal case report prior to the work of Orons et al. Piggyback caval anastomoses for entire grafts: B is with an endto-end anastomosis with the recipient hepatic vein after recipient hepatic vein venotomy, and C is an end-to-side with a graft patch to the facet of the recipient cava. An end-to-side anastomosis with potential venotomy/triangulation of the graft hepatic venous outflow for split grafts. Also for cut up grafts is an end-to-end anastomosis between the graft hepatic venous outflow and the recipient hepatic veins. The graft (G) hepatic artery is subdivided into the extrahepatic hepatic artery (a) and the intra-hepatic/branch hepatic arteries (b). The hollow arrow points to the positioning of arterial narrowing (hepatic artery stenosis). Fluoroscopic image throughout balloon angioplasty of the anastomotic hepatic artery stenosis (hollow arrow). Postangioplasty digital subtraction angiogram of the celiac axis (trunk) through the reinforced sheath demonstrating a corrugated look to the recipient common hepatic artery due to spasm (between strong arrows). The operator gave the affected person 300 mg of intra-arterial nitroglycerin by way of the sheath, followed by 20 cc of warm zero. Completion digital subtraction angiogram of the celiac axis (trunk) via the reinforced sheath after elimination of the wire and intra-arterial nitroglycerin injection demonstrating much less spasm and the lower than 30% residual stenosis on the anastomosis (hollow arrow). Management of hepatic artery steno occlusive problems after liver transplantation. Management of hepatic artery steno-occlusive issues after liver transplantation. Hepatic artery stenosis after liver transplantation: incidence, presentation, remedy and long-term end result. The dangers include recoil to simple angioplasty (high technical failure), arterial dissection, spasm and/or thrombosis. It represents 58% of arterial complications and is twice as prone to occur in pediatric recipients compared to grownup entire graft recipients: 4% to 11% versus 11% to 26%, respectively. They embrace: (1) intermittant relapsing bacteremia, (2) biliary ischemia (biliary strictures, biliary solid syndrome, biliary necrosis), and (3) fulminant hepatic failure (rapidly deteriorating graft function). For years this principle hinged on the age-related capacity of the pediatric recipient inhabitants to create arterial collaterals. This brings further hypothesis as to the purpose for increased arterial collaterals beyond the mere age of the recipients. As a result, the speculative theories of increased collateral formation may hinge on break up grafts and never solely pediatric recipients. Short-Segment Hepatic Artery Occlusion that is uncommon and is the most underdescribed arterial complication after liver transplantation. Extrahepatic lesions (less common) would probably be short-segment thrombus or a focal ischemic damage. This is as a outcome of these lesions are recalcitrant to balloon angioplasty and recoil instantly, requiring stent bailout. The function of endovascular remedy is additional unclear in the literature because the expertise is scant, inconsistent, and thus largely anecdotal. Techniques, vascular anatomy, the standing of the graft at time of remedy, and the time lapse between transplant and endovascular remedy (age of the thrombus) are a few of the variables that are inconsistently reported. Thrombolysis of aortohepatic conduits, all variables being the same, might (in theory) be easier to thrombolyse because the conduit according to the hepatic artery vascular mattress is an end artery and pharmacolytics have nowhere to go however into the liver. Moreover, as soon as an anatomic defect is unmasked after pharmacolysis, it must be resolved (either by endovascular means or surgical revascularization) to obtain definitive therapy. The author speculates that the situation is probably under-recognized in sure establishments and might be overcalled in others. These patients did nicely with a patency rate in all 4 patients exceeding 1 yr following revascularization. This discovering represents very sluggish hepatic arterial flow and, on this case, the edge may be set excessive, to the extent that the sensitivity of this angiographic discovering is low. Certain studies have evaluated the incidence of splenomegaly (>830 mL has a 75% accuracy), nominal splenic artery diameters (>4 mm is taken into account significant), and/or the ratio of the splenic artery to the hepatic artery (>1. When reported, portal vein velocities have been valued at larger than 50 (up to 150) cm/second66,seventy four,seventy six (see significance of this below). However, portal vein velocities have also been reported between thirteen and 37 cm/second. Unfortunately, the splanchnic hemodynamics are partly understood, and this adds to the issue in making this diagnosis. There is an issue concerning the precise cause of the hepatic artery hypoperfusion in splenic steal syndrome. Initially when it was first described (1990�1993), it was thought-about a real arterial flow phenomenon with circulate preferentially going to the splenic artery and being diverted from the hepatic artery (a true steal phenomenon); hence the unique name of the syndrome. A lowresistant splenic mattress relative to a higher-resistant hepatic mattress would favor circulate towards the spleen (splenic steal). This has been partly mentioned by prior authors, where they proposed that causes of elevated hepatic arterial resistance could worsen the splenic steal situation. There is a partly reciprocal relationship between the arterial half (A, high half of illustration) and the porto-venous half (B, decrease half of illustration) of the illustration. The arterial half of the system (A, high half of illustration) is a stability between the peripheral arterial resistance of the splenic vascular mattress (resistance of splenic vasc. The portovenous half of the system (B, decrease half of illustration) is a balance between the dimensions and high quality of the hepatic graft and the degree of portal venous circulate. The drawback can be an undersized graft or portal venous hyperperfusion, or each (it is relative). We can solely speculate that "splenic steal syndrome" might have a number of causes and, if certain causes predominate, there could additionally be a number of varieties. Furthermore, there may be levels of severity of this or these hypoperfusion phenomena. This specific embolization would utilize standard microcatheter methods and available bland particulate embolic products. Usually two to three classes are required to assist scale back the splenic quantity with decreased threat of splenic infarction with superadded abscess formation. Intrahepatic PsA have related etiology, prognoses, and management as other intrahepatic arterial injuries. Furthermore, some native livers may be poorly compliant because of cirrhosis, chemoembolization, and liver fibrosis.
Since the analysis of constriction is finally that of altered physiology impotence from blood pressure medication buy 160 mg super avana with mastercard, cine imaging is a more direct technique of confirming the analysis erectile dysfunction treatment shots super avana 160 mg order. The most sensitive and specific finding is the septal bounce erectile dysfunction recovery stories super avana 160 mg generic on line, greatest appreciated in inspiration. During inspiration, the negative intrathoracic strain results in extra fast right coronary heart filling than the left. In a patient with distant history of tuberculosis, posteroanterior (A) and lateral (B) chest radiographs demonstrate irregular curvilinear calcification (arrows) about the lower left heart border extending to the diaphragmatic floor of the heart. Underlying myocardium also must be evaluated in these circumstances because the presence of the myocardial issue (myocardial atrophy or fibrosis) is a contraindication to pericardiectomy, because of the risk of acute dilatation or rupture of 1 or each cardiac chambers following surgical procedure. The typical scientific setting is that pericardial effusion is identified in a patient with signs of heart failure and despite drainage of the effusion, the affected person continues to have irregular pericardial dynamics. Other rarer causes could additionally be infectious pericarditis or from a gastrointestinal fistula. Pneumopericardium following pneumothorax or pneumomediastinum normally signifies a disruption of the pericardium. Metastases to the guts and pericardium are found at autopsy in 10�12% of all sufferers with malignancies. Leukemias, lymphomas and melanomas are the other malignancies that can spread to the pericardium. Metastatic melanoma is an exception; it may have high-signal intensity on T1-weighted photographs which is virtually pathognomonic of this analysis. These include benign tumors (lipoma, benign teratoma, fibroma, and hemangioma) and malignant tumors (mesothelioma, lymphoma, sarcoma and liposarcoma, malignant teratoma). Although pericardial mesotheliomas characterize less than 1% of all malignant mesotheliomas, they account for 50% of all main pericardial tumor. Histopathology is often essential to achieve a definitive diagnosis of most pericardial tumors. Fibroma characteristically has low sign depth on T2-weighted pictures with poor enhancement traits. A coronary artery aneurysm should be suspected when a clean enhancing mass is seen along the expected course of a coronary artery. With the advantages of a big field of view and excessive gentle tissue contrast, these imaging modalities might help differentiate pericardial diseases, particularly when echocardiography findings are equivocal. Comparison of radiation doses from multislice computed tomography coronary angiography and conventional diagnostic angiography. Maximal thickness of the traditional human pericardium assessed by electron-beam computed tomography. Computed tomography and Magnetic resonance imaging of the pericardium: Anatomy and pathology. Congenital deficiencies in partial pericardium: Review with two new cases together with successful diagnosis by plain roentgenography. The usefulness of threedimensional multidetector computed tomography to delineate pericardial calcification in constrictive pericarditis. Cardiac and paracardiac plenty: Current opinion on diagnostic evaluation by magnetic resonance imaging. It also performs an necessary position in assessment of myocardial viability, preoperative threat assessment for patients present process noncardiac surgical procedure and evaluation of efficacy of revascularization therapy. Tl-201 being a potassium analog is transported across the myocardial cell membrane in an analogous method. After the preliminary uptake, Tl-201 undergoes redistribution which is continuous trade of Tl-201 between the myocardial cell and the vascular blood pool. However, it has a comparatively long half-life (73 hr) which increases radiation burden to the patient and a low photon vitality (69�80 keV) which outcomes in low decision images with vital attenuation by soft tissues. Tc99m-Tetrofosmin (6, 9-bis (2-ethoxy)-3, 12-dioxa-6, 9 diphosphatetradecane) is a lipophilic cationic compound which enters myocardial cells through passive transport pushed by the unfavorable membrane potential of the cell membrane. Both sestamibi and tetrofosmin are available within the package type which requires reconstitution with Tc99m radiotracer. It has a brief half-life (6 hours) and so a higher dose can be administered with much less radiation burden. This could be achieved by stressing the patient physically or by pharmacological stress to improve the coronary artery flow. During stress, blood move increases in regular coronaries however not in stenosed coronary artery. When injected at peak stress, perfusion radiotracers reflect myocardial perfusion at peak stress with lowered radiotracer uptake reflecting hypoperfused myocardium. Images acquired 2�3 hours after the stress will show the myocardial perfusion at relaxation. In patients with regular coronaries, the tracer is homogenously distributed within the left ventricular myocardium on each stress and relaxation pictures. Regions of decreased perfusion on stress photographs may be as a outcome of decreased flow secondary to the obstructed coronary artery or because of lack of viable myocytes. If perfusion defects on stress pictures persist on the remaining pictures, it suggests scarred myocardium. Therefore, two separate injections, one at peak stress and the other at relaxation are administered. Beta blockers are stopped forty eight hours and calcium channel blockers 24 hours earlier than research. At peak train, when target coronary heart rate (85% of age predicted most heart price or when other normal exercise end level criteria) is achieved, three. Thallium-201 rest/redistribution images are acquired 3�4 hours after the stress pictures. For Tc99m-labeled tracers, 8�10 mCi tracer is injected intravenously at peak exercise. The pictures are acquired 30�45 minutes later to allow the clearance of tracer from the liver. In some facilities, a two day protocol is adopted by which the stress and rest research is performed on separate days. In patients unable to train or reach goal coronary heart fee with physical exercise, pharmacological stress can be performed. Commonly used brokers for pharmacological stress are dobutamine, adenosine and dipyridamole. Patient preparation for pharmacological stress is much like the train protocol. In addition, for adenosine and dipyridamole, medicine and meals containing theophylline and caffeine are discontinued as they counteract the action of these vasodilators. Both these vasodilators may cause bronchospasm and therefore, should be averted in sufferers with bronchial asthma or severe obstructive lung illness. The improve in heart fee and myocardial contractility leads to an increase in myocardial oxygen demand leading to secondary dilation of coronary arteries and thus an increase in blood move. Adenosine is produced endogenously in the coronary endothelium which prompts the coronary receptors that produce vasodilation. Dipyridamole acts as an indirect vasodilator; it will increase the extracellular concentration of adenosine by blocking its intracellular reuptake and in addition inhibits the intracellular breakdown of adenosine. The radiotracer is injected at 2�3 min and the adenosine infusion continued for another 2�3 minutes. Assessment of prognosis and danger stratification 2872 Section 6 Chest and Cardiovascular Imaging three. This variable eliminates the referral bias of predominantly patients with abnormal scans being referred for angiography. Both breast tissue and diaphragmatic attenuation lead to high false positive results, more so with Tl-201 imaging. Visualization of normal systolic thickening in an area of hypoperfusion would assist distinguish attenuation artifact from a myocardial scar, the latter more than likely shall be associated with reduced systolic thickening. This helps to identify sufferers with high danger for future cardiac occasions who may be promptly referred for additional invasive strategies from patients at low danger who can be managed conservatively. This ends in effective price administration not solely at particular person patient stage but also for the entire neighborhood. Clinical statement and experimental studies have shown that this dysfunction can improve if enough viable myocardium is current within the dysfunctional segments. This led to understanding the 2874 Section 6 Chest and Cardiovascular Imaging idea of gorgeous and hibernating myocardium. There is reduction in mortality price in sufferers with viable myocardium treated with revascularization compared to medical remedy.
Diffusion- weighted pictures at b zero s/mm2 (B) and b 400 s/mm2 (C) show retention of sign at greater b value erectile dysfunction and diabetes a study in primary care super avana 160 mg order overnight delivery, suggesting restricted diffusion erectile dysfunction treatment seattle cheap 160 mg super avana. Sagittal T1W in-phase (D) and opposed-phase (E) pictures show suppression of marrow signal within the regular vertebrae www.erectile dysfunction treatment super avana 160 mg buy line. Diffusion restriction and absence of sign suppression on opposed section pictures are markers of malignant vertebral involvement. Collapse as a end result of osteoporosis will retain some normal fatty marrow which is able to show lack of sign on the opposed section picture. The elucidation of the full extent facilitates preoperative planning of the maximal diploma of debridement or the level of the amputation. Fat suppression techniques mixed with gadolinium administration further improve the sensitivity for detection of concerned areas. It can detect pre-erosive synovitis and can also establish early bone damage before it turns into obvious on radiography. In addition, brief bore highfield techniques presently allow passable affected person entry combined with excessive efficiency imaging capabilities. Three forms of magnets are clinically used for percutaneous biopsies: open low-field magnets (0. Improved affected person access with open magnet allows interventions in any desired airplane and affected person place. Vertically open items permit unrestricted vertical and facet entry to the affected person at the most homogeneous portion of the magnetic field. However, because of larger area strength, image high quality as nicely as the imaging pace is best. The size of the artifact is inversely proportional to the dimensions of the instrument and instantly proportional to the field power and to the angle the instrument makes with the main magnetic field. Typically, biopsy needles are displayed as dark areas surrounded by a brighter rim. Fine needles of 20�24G with different tip configurations and slicing needles of 14�18G are commercially out there. After defining the goal region, a T1W or T2W suitable grid is mounted to the pores and skin of the affected person to assist in selecting needle entry site. The angle and distance from skin to the lesion may be obtained by using commonplace scanner software. In the open magnet, a palpating finger could also be used as a substitute of a grid for entry site. The instrument could be tracked by continuous repetition of a quick imaging sequence. For the optimal use of this know-how the radiologist must couple these photographs with an in depth data of pathophysiology and scientific perspective in order that he can information the referring clinician appropriately. Advanced magnetic resonance imaging techniques in the analysis of musculoskeletal tumors. The main advantage of nuclear drugs imaging stems from the fact that practical changes appear much earlier than anatomical modifications. Hence, nuclear medicine imaging permits early detection of illnesses affecting musculoskeletal system. The present chapter summarizes the nuclear medication methods used for musculoskeletal imaging and their utility in various benign and malignant pathologies involving the musculoskeletal system. This osteoblastic activation could be seen due to wide array of pathologies, thereby decreasing the specificity. The routine bone scintigraphy employs whole physique anterior and posterior sweep photographs. It provides three-dimensional pictures and is useful in patients with regular planar pictures despite symptoms and in those with equivocal findings. The presences of p-c-p bonds make these compounds proof against hydrolysis by bone phosphatases, thereby rising the organic half life. Three to 4 hours after intravenous injection about 25�35% of radiotracer is retained in the regular grownup skeleton, the remaining is excreted within the urine by way of the kidney. These phosphorus containing complexes avidly attach themselves to the hydroxyapatite crystal surface by the method of chemisorptions. The inherent physics of positron decay allows tomographic imaging with out the need for collimators thereby improving the sensitivity and resolution. It impacts approximately two-thirds of most cancers sufferers, with breast most cancers being the leading trigger in girls, prostate most cancers in males, followed by lung most cancers in each sexes. Accurate assessment of skeletal involvement is essential for optimum management of these patients. For the previous few many years, planar bone scintigraphy has been essentially the most incessantly performed imaging examine in the analysis of metastatic bone disease. Although scintigraphic findings alone are sometimes nonspecific for skeletal pathologies, this method reportedly has an beautiful sensitivity. Radiographs are found to be adverse in 30�50% of patients with optimistic bone scan. Most widespread sample of bone metastasis is a quantity of "scorching" lesions distributed randomly throughout the skeleton. False-negative leads to bone scintigraphy are seen in avascular lesions, in the presence of quickly growing pure osteolytic metastases with no reactive elevated osteoblastic exercise, or in lesions with low bone turnover (multiple myeloma, thyroid cancer). Planar bone scintigraphy (A and B) confirmed a suspicious focal uptake in left superior pubic rami (arrow). This may assist characterize indeterminate lesions and information targeted biopsy of essentially the most metabolically lively space inside bigger tumors. This facet is particularly important in many gentle tissue and bone tumors which are of blended grade and/or cell type. It addition bone scintigraphy has been used for detecting recurrence after radiofrequency ablation of osteoid osteoma. Other benign lesions, which may show increased uptake, are eosinophilic granuloma, aneurysmal bone cyst, chondroblastoma, enchondroma, and so on. The basic findings are increased regional blood move and blood pool with a corresponding increased uptake on delayed pictures. This is totally different from cellulitis the place solely enhance in blood circulate and blood pool in the delicate tissue with no elevated radiotracer uptake on delayed picture is seen. Compared with anatomic modalities, the radionuclide bone scan has the additional benefit of detecting multiple foci of disease which could be seen especially in children. Planar bone scintigraphy (A and B) exhibits mass in left femoral shaft with heterogeneous tracer uptake (arrows), in keeping with main tumor. Planar bone scintigraphy (A and B) confirmed elevated irregular tracer uptake in D6 vertebra (arrow). The findings were highly suspicious for tuberculosis and confirmed at histopathology thrombosis. Bone scan stays optimistic for months even after successful therapy of acute osteomyelitis. However, 67 Ga-Citrate scintigraphy suffers from poor picture high quality, lengthy scanning time and significantly higher affected person radiation dose resulting in decline in its use with introduction of better tracers. Its uptake is dependent on the chemotaxis of labeled leukocytes on the website of infection. As the overwhelming majority of leukocytes labeled are neutrophils, the process is most helpful for identifying neutrophil mediated inflammatory processes, similar to bacterial infections. It is much less helpful for these sicknesses in which the predominant cellular response is aside from neutrophilic, such as tuberculosis. It supplies better resolution and shorter test period in comparability with standard radionuclide procedures, albeit with larger price and radiation publicity. It has been proven to be superior to labeled leukocyte imaging for chronic musculoskeletal infections. It must be remembered that image interpretation in patients with prosthetic devices can be affected by attenuationcorrection-induced artifacts. Foot osteomyelitis incessantly presents with out systemic illness and with no apparent scientific signs or indicators, besides the ulcer and imaging research are often wanted to affirm the prognosis. Labeled leukocyte imaging may be extra delicate for detecting clinically unsuspected pedal osteomyelitis and is beneficial for monitoring response to medical therapy. Although the scientific outcomes of joint replacement surgery are often excellent, these implants do fail. Aspetic loosening due to mechanical elements and inflammatory reaction to prosthetic parts is the most typical trigger for implant failure followed by infection.
Depending on the nature of the malignancy and the remedy regimen impotence while trying to conceive order 160 mg super avana amex, the onset cialis erectile dysfunction wiki super avana 160 mg generic with visa, severity erectile dysfunction drugs medications 160 mg super avana generic with amex, and length of these adjustments are variable, as are its results and functional and psychosocial outcomes. Patients receiving several types of cytotoxic therapy together are at a higher danger of developing cognitive impairment after therapy (Cheung 2012). Prevalence Cognitive modifications can include poor word or name recall, problem staying centered, diminished capability to study new issues, 114 Depending on the type of most cancers investigated, estimates of the prevalence of cancer-related alterations in cognitive operate are 16%�75% throughout therapy, though these adjustments can stay after completion or withdrawal of treatment (Cheung 2012). Neuroimaging research have revealed a correlation between deficits in cognitive operate and white matter modifications within the mind. Supported by findings from neuropsychological checks, stories point out that individuals can still have cognitive changes for as lengthy as 20 years after chemotherapy for breast most cancers (Koppelmans 2012). On evaluate of systems, he has complaints of numbness and tingling in his fingers, and the signs affect him significantly throughout his every day exercise. Before his cancer analysis, the affected person had a medical history of diabetes and peripheral neuropathy, and he had used oxycodone intermittently to management his ache. The oncologist believes that the affected person has persistent peripheral neuropathy exacerbated by his current use of oxaliplatin. Randomized managed trials have shown the efficacy of controlled-release oxycodone within the therapy of diabetic neuropathy. Chemotherapy-induced peripheral neuropathy is a cause of significant distress in patients with cancer and is associated with decreased high quality of life and functional disability. On objective nerve conduction research, a number of abnormalities are detected, which embody axonal loss (refers to lower nerve amplitudes) and demyelination (refers to prolonged latency and gradual conduction velocity). For treatment of his neuropathy, duloxetine is useful and can be indicated for the therapy of diabetic neuropathy. Effect of duloxetine on ache, operate, and high quality of life among patients with chemotherapyinduced painful peripheral neuropathy: a randomized scientific trial. Current Management Screening and Assessment Questionnaire) can be used to assess how cognitive impairment affects health-related high quality of life. Nonpharmacologic Interventions Survivors reporting cognitive changes should be screened for probably reversible components that will contribute to cognitive changes, which embody psychological misery, fatigue, sleep disturbances, and ache. Assessment of cognitive complaints should determine the onset, severity, duration, and domains of cognitive modifications. Brief screening instruments such as the Mini-Mental State Examination lack sufficient sensitivity to detect a refined decline in cognitive efficiency. A complete neuropsychological analysis is helpful to establish the precise cognitive domains of deficit. Cognitive training is a type of brain training, aiming to improve neurocognitive perform. Studies have instructed that the advantages of cognitive coaching outcome from an total enhancement in self-reported high quality of life. This could be because of the poor understanding of organic mechanisms behind this phenomenon. Data are conflicting on the evaluation of short- and medium-term cognitive measures between psychostimulants corresponding to methylphenidate and modafinil and controls. One randomized, double-blind, crossover trial that enrolled childhood most cancers survivors of acute lymphoblastic leukemia or brain tumors found that methylphenidate was more effective than placebo in enhancing consideration, cognitive flexibility, and processing speed (Conklin 2007). However, these results have been inconsistent with those of one other trial of sufferers with breast most cancers (Mar Fan 2008). In the first section, all sufferers received modafinil a hundred mg as soon as daily for three days, adopted by 200 mg as quickly as day by day throughout a 4-week openlabel period. In the following phase, patients reaching a positive response in attention and memory within the first phase had been randomized to an extra four weeks of modafinil 200 mg/day or placebo. In the evaluation of short- and mediumterm cognitive measures between modafinil and controls, no statistically vital distinction in cognitive measures was observed. Gingko biloba was studied for preventing cognitive impairment in sufferers with breast cancer receiving adjuvant chemotherapy. The intervention commenced at the second cycle of chemotherapy and continued until 1 month after the top of chemotherapy. There have been no significant variations in both subjective or goal cognitive measures between the two teams (Barton 2013). Breast most cancers survivors, compared with healthy controls, reported longer-lasting fatigue within the week earlier than all 4 examine assessments (p<0. A higher share of sufferers than wholesome controls scored in the irregular vary on this measure throughout every assessment (p<0. Patients receiving radiotherapy alone had their most extreme fatigue at the finish of therapy, and patients who received multimodality remedy (chemotherapy and radiation) had their most extreme fatigue as a lot as 2 months after chemotherapy (Jacobsen 2007). Cancer-related fatigue can also happen because of cancer-related signs corresponding to pain, nausea, and dyspnea. Alterations in the hypothalamic-pituitary-adrenal axis, alterations within the cellular immune system, and reactivation of latent herpes virus may also contribute to fatigue. Recent studies have additionally advised that chemotherapy results in dysregulation of proinflammatory cytokine concentrations (Eyob 2016). Patients fee fatigue as extra distressing than different cancer- or treatment-induced symptoms, including nausea and pain. Cancerrelated fatigue can also negatively have an result on the standard of lifetime of patients with cancer; people who report vital levels of fatigue decrease their participation in actions that make their lives significant. Pharmacologic therapies have restricted roles as a outcome of experimental research are lacking, and a major placebo response has occurred in randomized trials. Screening must be carried out and documented using a quantitative or semiquantitative evaluation. For instance, on a 0�10 numeric score scale (0 = no fatigue; 10 = worst fatigue imaginable), mild fatigue is indicated by a rating of 1�3, average fatigue by 4�6, and severe fatigue by 7�10. Recommendations for bodily exercise are described underneath Lifestyle-Related Prevention. Survivors ought to be referred to psychosocial service providers who specialize in most cancers and are educated to deliver empirically based mostly interventions. However, more studies are required before standardized suggestions may be made for these therapies. It can be advised that insomnia may be exacerbated among survivors by continual antagonistic results of anticancer therapy, emotional misery, drugs, and maladaptive behaviors, including adjustments in sleep patterns and poor sleep hygiene. For administration of insomnia, it is very important assess whether or not sufferers have any treatable contributing components, including comorbidities such as hypothyroidism, caffeine consumption late in the day, emotional distress, shift work, and different symptoms similar to fatigue and pain which will contribute to insomnia. Sleep issues are usually classified as insomnia, sleep disturbances, and/or extreme sleepiness. Insomnia has been recognized as one of the prevalent sleep problems amongst most cancers survivors. Sleep issues might result in many unfavorable health outcomes, together with poor health-related high quality of life, fatigue, poor healing, cognitive dysfunction, lost work productiveness, accidents, poor relationships, and increased well being care costs. Insomnia could be problematic as a outcome of it may decrease daytime functioning and result in poor high quality Physical activity is well established inside the literature to improve sleep among most cancers survivors. One randomized managed trial in contrast a standardized yoga intervention mixed with commonplace of care with standard of care alone to enhance average to severe sleep disruption amongst most cancers survivors. Participants within the yoga group had higher improvements in international and subjective sleep high quality, daytime functioning, and sleep efficiency and reductions in hypnotic use. A Cochrane review also instructed that exercise can improve sleep at a 12-week follow-up (Mishra 2012). However, the best standardized exercise/activity routine to enhance insomnia in most cancers survivors is unknown. Cognitive behavioral remedy may benefit most cancers survivors for the management of insomnia. Other nonpharmacologic strategies corresponding to sleep hygiene schooling are additionally deemed important. For example, it is suggested that survivors scale back shiny light (computer or phone screens or mild sources close to the eyes) within a few hours before bedtime and in the course of the night. In addition, they should avoid alcohol, caffeine, nicotine, and heavy meals close to bedtime.
Mature chondrocytes seldom divide but stay metabolically active erectile dysfunction vitamin e super avana 160 mg buy with visa, synthesizing and turning over matrix proteoglycans erectile dysfunction walgreens discount 160 mg super avana. A complex network of cytokines and growth factors secreted by synovial lining cells and by Imaging Modalities 1 erectile dysfunction caused by low testosterone 160 mg super avana discount. Conventional radiography: It is the preliminary examination performed in routine evaluation of degenerative arthritis. It is a sensitive and cost-effective modality, therefore, appropriate for giant scale studies and follow-up of patients. The electrostatic repulsion of aggrecan gives cartilage its compressive stiffness. In early osteoarthritis, regardless of an increased manufacturing of aggrecan and matrix in general, the net concentration of aggrecan in cartilage falls as degradation outweighs synthesis. Eventually, superficial fibrillation and cracking of the matrix occur, which are adopted by focal disintegration and ulcerations of cartilage. At the joint margins, chondral constructions form at sites of pressure, and endochondral ossification happens in these structures, producing chondro-osteophytes, so referred to as "osteophytes". Osteophytes type in areas of low stress, rising the surface space of the articular cartilage, thereby, lowering the stresses that are experienced by the joint and enhance joint stability. Synovial involvement in osteoarthritis may contribute to disease by serving as the supply of cytokines similar to interleukin-1 that will flip off chondrocyte-mediated cartilage matrix synthesis and set off synthesis of degradative enzymes, by secreting excess synovial fluid that makes the joint-lax and susceptible to damage. Attrition and perhaps even low-bone density are related to the progression of osteoarthritis, and it seems probably that high-bone density contributes only to the preliminary occurrence of illness and not necessarily to its development. Women have a highrisk for osteoarthritis after about age of fifty years, a lot higher than the risk for men. Studies have been inconsistent concerning whether or not estrogen substitute therapy eliminates that danger. Preliminary knowledge suggest that dietary deficiencies could improve the incidence or progression of osteoarthritis, together with low-level intakes of vitamin C, vitamin E, and vitamin D. Developmental abnormalities occurring during infancy or childhood that leave a hip-joint misshapen and that increase local stresses to cartilage in that hip-joint predispose to hip osteoarthritis in early maturity. The three types of congenital and developmental abnormalities which would possibly be most commonly implicated are congenital dysplasia, Legg�Perthes disease, and a slipped capital femoral epiphysis. Although these abnormalities are uncommon in childhood, milder varieties could also be more common and should account for a large proportion of osteoarthritis of the hips in adults. Injury to the knee in an adolescent is unlikely to trigger osteoarthritis shortly, if in any respect. In distinction, older joint is extra vulnerable to main damage than the younger joint. There is a better percentage of hand and hip osteoarthritis as a result of inheritance than knee osteoarthritis. It is more and more likely that the genetic predisposition to osteoarthritis will be based on a selection of physiologic vulnerabilities, together with alterations in minor collagens within cartilage, changes in enzymes or their activators within cartilage, variations in cytokines, or growth factor profiles in cartilage and genes that dictate joint form and structure. Weight probably will increase the chance for knee osteoarthritis by increasing the amount of mechanical load across a joint. Indeed, each pound of weight is multiplied threefold to sixfold in phrases of its effect on knee loading. Although, obesity markedly increases the chance for knee osteoarthritis, its relationship to hip osteoarthritis is 3068 Section 7 Musculoskeletal and Breast Imaging not as robust. Muscle weak spot: As a consequence of disease, individuals with osteoarthritis have weak point in the muscular tissues that bridge, the diseased joint. Also, direct neurologic messages transmitted by a swollen joint by way of afferent impulses inhibit the maximal contraction of muscles bridging joints, resulting in apparent weak point. This weak point most likely accounts for much of the disability and should enhance the danger of development. Joint Overuse from Occupations and Athletics the traditional joint is built to face up to the appreciable dynamic loading that occurs with day by day activities. Examples include jobs that require regular knee bending and lifting or carrying heavy masses, which predispose to knee osteoarthritis. This will not be true for nationally aggressive skilled runners who are extra likely to have hip osteoarthritis. They commonly type at the margins of the joint the place increased vascularization of subchondral bone stimulates endochondral ossification. Marginal and central osteophytes develop through endochondral ossification after vascularization of subchondral bone marrow. Periosteal osteophytes form from a course of resembling appositional bone progress as a end result of stimulation of periosteal membrane; capsular osteophytes develop in reaction to capsular traction forces. Subchondral sclerosis: It is believed to be brought on by redistribution of stress that results from progressive cartilage loss. Subchondral sclerosis occurs at these sites on account of deposition of recent bone on preexisting trabeculae and trabecular microfractures with callus formation. Cysts typically are multiple, and, histologically, can include myxoid and adipose tissue, occasional cartilage with surrounding fibrous elements and are bordered by peripheral sclerotic bone. Osteophytes of the central sort result in new bone formation within the middle of the joint and therefore might produce an irregular contour of the joint surface. Besides the articular floor itself, different articular buildings, corresponding to ligamentous and capsular tissue could endure extreme degenerative adjustments, including thickening, disruption and distortion, which lead radiographically to deformation, malalignment and subluxation of the joint. Degenerative lesions additionally occur in intra-articular fibrocartilaginous tissue, similar to menisci within the knee or the labra in hip and shoulders. Fragmentation of the cartilaginous or osseous surface, especially in advanced disease can lead to the formation of Radiographic�Pathologic Correlation Altman et al. In the stressed section of the joint, cartilage damage is evidenced by thinning of the cartilage rim and growth of erosions and ulceration. Distinctive patterns of nonuniform loss of articular cartilage result in the traditional patterns of femoral head migration which may be categorized into three different patterns: (i) superior migration, (ii) medial migration, and (iii) axial migration. Depending on their measurement and placement, intra-articular bodies may cause joint irritation with scientific symptoms and acceleration of osteoarthritis. The superior aspect of the joint area is visualized however with a unique projection of the femoral head. Neither anteroposterior nor frog-leg views permit assessment of the anterior and posterior a half of the joint area. Therefore, anterior and posterior indirect views (between 30o�45o) are additionally really helpful. All of these views besides the frog-leg view may also be obtained underneath weight-bearing situations, which supplies more correct measurement of the joint house. The "false profile" view is an oblique lateral view of the hip obtained in the erect position. The superolateral kind is characterised by unilateral and uneven modifications, together with narrowing of the superior joint house, which causes the femoral head to move superiorly. In more superior illness, flattening of the superolateral side and lateral displacement of the femoral head result in widening of the inferomedial joint space. In the stress zone on the lateral and outer aspect of the femoral head and acetabulum, sclerosis, cyst formation and osteophytes also could be seen. Superomedial migration generally happens bilaterally and in distinction to the superolateral pattern, is extra frequent in men than women. After superior movement of the femoral head with narrowing of the superior joint area and progressive head deformity, broad primarily based osteophytes begin to fill within the apparently widened medial part of the joint house. Other findings on this explicit migration pattern are osteophytes and cystic lesions on the lateral and outer elements of the femoral head and acetabulum in affiliation with subchondral sclerosis. Medial Migration Pattern Medial migration of the femoral head can be observed in about 22% of all patients with osteoarthritis. Radiographically, joint area loss in the medial aspect with consequent widening of the lateral aspect of the joint area is the most common discovering. Osteophytes develop on the lateral and medial sides of femur and acetabulum, and cystic lesions are mostly small. The presence of osteophytes and sclerosis as well as the absence of erosions and osteoporosis adjoining to the joint may be helpful for differentiation. Inflammatory disease will normally cause erosive changes and aggressive destruction of cartilage.






