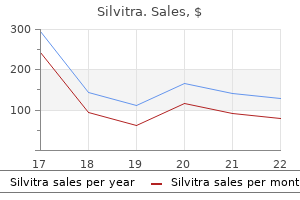
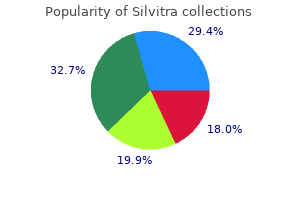
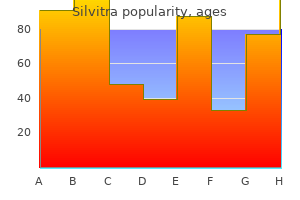
Silvitra
Silvitra
Silvitra dosages: 120 mg
Silvitra packs: 10 pills, 20 pills, 30 pills, 60 pills, 90 pills, 120 pills, 180 pills

They behave as cationic discount erectile dysfunction pills buy 120 mg silvitra mastercard, surface-active compounds that disrupt the permeability of both the outer and the cytoplasmic membranes of gram-negative bacteria zinc causes erectile dysfunction generic silvitra 120 mg with mastercard. The -lactamases of gramnegative micro organism are confined to the periplasm best pills for erectile dysfunction yahoo cheap silvitra 120 mg without prescription, between the inner and outer membranes, whereas gram-positive bacteria secrete their -lactamases into the encompassing medium. These enzymes have a higher affinity for the antibiotic than the antibiotic has for its goal. Genes encoding -lactamases have been present in both chromosomal and extrachromosomal places and in both grampositive and gram-negative micro organism; these genes are often on mobile genetic elements. Many "advanced-generation" -lactam antibiotics, such as ceftriaxone and cefepime, are steady within the presence of plasmid-mediated -lactamases and are lively towards bacteria proof against earlier-generation nedasalamatebook@gmail. One strategy that has been devised for circumventing resistance mediated by -lactamases is to mix the -lactam agent with an inhibitor that avidly binds the inactivating enzyme, preventing its assault on the antibiotic. No -lactam antibiotic or inhibitor has been produced that may resist all the many -lactamases that have been recognized. A last resistance mechanism is the coupling, in gramnegative micro organism, of a decrease in outer-membrane permeability with fast efflux of the antibiotic from the periplasm to the cell exterior. Mutations of genes encoding outer-membrane protein channels referred to as porins lower the entry of -lactam antibiotics into the cell, whereas extra proteins kind channels that actively pump -lactams out of the cell. Resistance of Enterobacteriaceae to some cephalosporins and resistance of Pseudomonas spp. These mutants have been apparently selected in sufferers who have been undergoing prolonged vancomycin remedy. Aminoglycoside-modifying enzymes, normally encoded on plasmids, transfer phosphate, adenyl, or acetyl residues from intracellular molecules to hydroxyl or amino aspect teams on the antibiotic. The modified antibiotic is less lively because of diminished binding to its ribosomal goal. Modifying enzymes that may inactivate any of the obtainable aminoglycosides have been found in each gram-positive and gram-negative micro organism. A second aminoglycoside resistance mechanism, which has been identified predominantly in scientific isolates of Pseudomonas aeruginosa, is decreased antibiotic uptake, presumably as a outcome of alterations within the bacterial outer membrane. Methylation mediates resistance to erythromycin, clarithromycin, azithromycin, clindamycin, and streptogramin B. Resistance to streptogramin B converts quinupristin/dalfopristin from a bactericidal to a bacteriostatic antibiotic. Streptococci can even actively trigger the efflux of macrolides, and staphylococci could cause the efflux of macrolides, clindamycin, and streptogramin A. Ketolides corresponding to telithromycin retain exercise towards most isolates of Streptococcus pneumoniae that are immune to macrolides. In addition, staphylococci can inactivate streptogramin A by acetylation and streptogramin B by both acetylation or hydrolysis. The genes encoding resistance are carried on plasmids that can switch themselves from cell to cell and on transposons that may leap from plasmids to chromosomes. This kind of acquired vancomycin resistance was confined for 14 years to enterococci-more specifically, to Enterococcus faecium quite than the extra common pathogen E. All of the isolates include vanA, the gene that mediates vancomycin resistance in enterococci. Resistance in gram-positive micro organism is due either to active efflux or to ribosomal alterations that diminish binding of the antibiotic to its goal. Some gram-negative micro organism develop mutations that both decrease outer-membrane porin permeability and trigger active drug efflux from the cytoplasm. Mutations that result in energetic quinolone efflux are additionally present in gram-positive micro organism. The fast number of resistant mutants is the major limitation to the use of this antibiotic towards otherwisesusceptible staphylococci and requires that the drug be used in combination with one other antistaphylococcal agent. The two major mechanisms are the acquisition of multiple unrelated resistance genes and the event of mutations in a single gene or gene complex that mediate resistance to a collection of unrelated compounds. The development of multiresistant strains by acquisition of multiple genes occurs by sequential steps of gene switch and environmental choice in areas of high-level antimicrobial use. In contrast, mutations in a single gene can conceivably be chosen in a single step. Bacteria which might be multiresistant by virtue of the acquisition of latest genes embody hospital-associated strains of gram-negative bacteria, enterococci, and staphylococci and communityacquired strains of salmonellae, gonococci, and pneumococci. Mutations that confer resistance to a number of unrelated antimicrobial brokers occur within the genes encoding outer-membrane porins and efflux proteins of gramnegative micro organism. These mutations decrease bacterial intracellular and periplasmic accumulation of -lactams, quinolones, tetracyclines, chloramphenicol, and aminoglycosides. Important traits include peak and trough serum concentrations and mathematically derived parameters corresponding to half-life, clearance, and distribution quantity. Pharmacokinetic data is beneficial for estimating the appropriate antibacterial dose and frequency of administration, for adjusting dosages in patients with impaired excretory capacity, and for comparing one drug with another. Oral Administration Most patients with infection are handled with oral antibacterial agents within the outpatient setting. However, therapeutic efficacy could also be compromised when absorption is lowered on account of physiologic or pathologic circumstances (such because the presence of food for some medication or the shunting of blood away from the gastrointestinal tract in sufferers with hypotension), drug interactions (such as that of quinolones and metallic cations), or noncompliance. Concentrations of most antibacterial brokers in interstitial fluid are just like free-drug concentrations in serum. In addition, although an antibacterial agent could penetrate to the site of infection, its exercise could additionally be antagonized by components in the native surroundings, similar to an unfavorable pH or inactivation by cellular degradation merchandise. For instance, for the rationale that exercise of aminoglycosides is decreased at acidic pH, the acidic environment in many infected tissues could also be partly liable for the relatively poor efficacy of aminoglycoside monotherapy. In addition, the abscess milieu reduces the penetration and native activity of many antibacterial compounds, in order that surgical drainage may be required for remedy. For many of the antibacterial medication, metabolism leads to lack of in vitro activity, although some agents, such as cefotaxime, rifampin, and clarithromycin, have bioactive metabolites that may contribute to their total efficacy. The most practical software of data on the mode of excretion of an antibacterial agent is in adjusting dosage when elimination capability is impaired (Table 33-3). Direct, nonidiosyncratic toxicity from antibacterial medicine may outcome from failure to scale back the dosage given to sufferers with impaired elimination. For brokers which are primarily cleared intact by glomerular filtration, drug clearance is correlated with creatinine clearance, and estimates of the latter can be utilized to information dosage. For medicine whose elimination is primarily hepatic, no simple marker is helpful for dosage adjustment in patients with liver disease. However, in patients with extreme hepatic illness, residual metabolic functionality is often enough to preclude accumulation and toxic effects. Susceptibility testing is designed to estimate the susceptibility of a bacterial isolate to an antibacterial drug underneath standardized situations. These circumstances favor quickly rising aerobic or facultative organisms and assess bacteriostasis only. Specialized testing is required for the assessment of bactericidal antimicrobial exercise; for the detection of resistance amongst such fastidious organisms as obligate anaerobes, Haemophilus spp. Antimicrobial susceptibility testing is essential when susceptibility is unpredictable, most often because of rising acquired resistance amongst micro organism infecting hospitalized sufferers. The breakpoint is the concentration of the antibiotic that separates vulnerable from resistant micro organism. When a majority of the isolates of a given bacterial species are inhibited at concentrations beneath the breakpoint, the species is considered to be within the spectrum of the antibiotic. The basic tenets of chemotherapy, to be elaborated under, embody the following: When appropriate, materials containing the infecting organism(s) should be obtained before the beginning of remedy so that presumptive identification may be made by microscopic examination of stained specimens and the organism can be grown for definitive identification and susceptibility testing. Awareness of native susceptibility patterns is useful when the affected person is treated empirically. Once the organism is identified and its susceptibility to antibacterial brokers is decided, the regimen with the narrowest efficient spectrum ought to be chosen. The alternative of antibacterial agent is guided by the pharmacokinetic and adverse-reaction profile of lively compounds, the site of infection, the immune status of the host, and evidence of efficacy from well-performed clinical trials. If all other elements are equal, the least costly antibacterial regimen must be chosen.
Such direct inoculation of mammal-adapted organisms expressing the F1 antigen is associated with primary septicemia and excessive mortality rates erectile dysfunction causes natural treatment 120 mg silvitra purchase amex. Pharyngeal plague may result from the ingestion of undercooked contaminated meat; outbreaks of pharyngeal plague have been reported among individuals consuming undercooked camel and goat meat erectile dysfunction viagra free trials silvitra 120 mg buy generic online. Plague can additionally be acquired by inhalation of infective respiratory droplets and perhaps by manual switch of infected fluids to the mouth in the course of the handling of contaminated animal tissues fluoride causes erectile dysfunction silvitra 120 mg purchase on-line. Although scientific plague commonly develops in contaminated cats, it rarely does so in infected canines. Both canine and cats could transport contaminated fleas from rodent-infested areas to the home environment. The mechanisms by which the organism causes disease are incompletely understood, however each chromosome- and plasmid-encoded gene products in addition to altered cell-mediated immune responses are involved. Three plasmids encode for a selection of identified or presumed virulence elements, including the F1 envelope antigen and numerous Yersinia outermembrane proteins, which confer bacterial resistance to phagocytosis; the V antigen, which is crucial for virulence and suppresses the synthesis of various proinflammatory cytokines. A chromosomally encoded lipopolysaccharide endotoxin is necessary in sepsis, playing a role in triggering the systemic inflammatory response syndrome and its complications. Plague can involve almost any organ, and untreated plague typically ends in widespread and massive tissue destruction. Primary septicemic plague consists of sepsis in the absence of a bubo; secondary septicemic plague is a complication of bubonic or pneumonic plague that occurs when local host defenses are breached. Primary plague pneumonia typically begins as a lobular course of after which extends by confluence, changing into lobar after which multilobar. Secondary plague pneumonia begins more diffusely, with organisms at first most numerous within the interstitium. Upright posteroanterior film taken at admission to hospital emergency division on third day of sickness, exhibiting segmental consolidation of proper higher lobe. Portable anteroposterior movie taken 8 h after admission, exhibiting extension of pneumonia to right center and proper lower lobes. Portable anteroposterior movie taken 13 h after admission (when patient had clinical adult respiratory distress syndrome), exhibiting diffuse infiltration all through proper lung and patchy infiltration of left decrease lung. In humans, the three principal forms of plague are bubonic, septicemic, and pneumonic. Bubonic plague, accounting in the United States for 75% of instances, is nearly at all times attributable to the chew of an infected flea however sometimes outcomes from direct contact with infectious materials. Septicemic and pneumonic plague could be both major or secondary to metastatic unfold. Unusual forms embody plague meningitis, endophthalmitis, and lymphadenitis at multiple sites. Primary plague pharyngitis has been documented by culture of organisms from throat swabs and may result from respiratory exposure or ingestion of undercooked flesh of infected animals. Patients expertise chills; fever, with temperatures that rise within hours to 38�C; myalgias; arthralgias; headache; and a sense of weak spot. Soon-usually inside 24 h-the affected person notices tenderness and ache in a quantity of regional lymph nodes proximal to the location of inoculation of the plague bacillus. Because fleas most often chunk the legs, femoral and inguinal nodes are most commonly involved; axillary and cervical nodes are subsequent most commonly affected. Within hours, the enlarging bubo turns into progressively painful and tender, typically exquisitely so. The patient often guards towards palpation and limits movement, stress, and stretch around the bubo. The surrounding tissue often turns into edematous, typically markedly so, and the overlying skin could also be erythematous, heat, and tense. Inspection of the pores and skin surrounding or distal to the bubo generally reveals the site of a flea bite marked by a papule, pustule, or ulcer. A record of lymphadenitic circumstances that could be confused with bubonic plague includes Staphylococcus aureus and group A -hemolytic streptococcal infections, cat-scratch illness, tularemia, and-in filariasis-endemic areas-acute filarial lymphadenitis. The bubo of plague is distinguishable from lymphadenitis of most other causes, however, by its rapid onset, its extreme tenderness, the accompanying indicators of toxemia, and the absence of cellulitis or obvious ascending lymphangitis. The pain and swelling of bubonic plague may be confused with a strangulated hernia or trauma. Treated within the uncomplicated state with an applicable antibiotic, bubonic plague normally responds shortly, with resolution of fever and alleviation of different systemic manifestations over 2�5 days. Buboes often remain enlarged and tender for per week or extra after the initiation of remedy and might turn into fluctuant. Without effective antimicrobial remedy, patients with typical bubonic plague manifest an increasingly poisonous state of fever, tachycardia, lethargy resulting in prostration, agitation and confusion, and (occasionally) convulsions and delirium. Septicemic Plague Primary septicemia, which accounts for 20% of instances within the United States, develops within the absence of a detectable bubo. Septic patients typically current with gastrointestinal signs of nausea, vomiting, diarrhea, and stomach ache, which may confound the correct analysis. In the United States in 1947�2001, 55 instances of primary septicemic plague with 13 deaths have been reported, for a case-fatality rate of 24%. The differential prognosis of septicemic plague includes sepsis of other gram-negative bacterial etiology, meningococcemia, and acute severe viral infections similar to hantavirus sickness. Pneumonic Plague Pneumonic plague is essentially the most life-threatening form of the illness. The incubation period for primary pneumonic plague is often 3�5 days (range, 1�7 days). The onset is most frequently sudden, with chills, fever, headache, myalgias, weakness, and dizziness. Pulmonary signs, together with tachypnea and dyspnea, cough, sputum production, and chest pain, usually come up on the second day of sickness and may be accompanied by hemoptysis, increasing respiratory distress, cardiopulmonary insufficiency, and circulatory collapse. In primary plague pneumonia, the sputum is most often watery or mucoid, frothy, and blood-tinged, but it could turn into frankly bloody. Pulmonary signs in main pneumonic plague could point out involvement of a single lobe in the early stage, with rapidly growing segmental consolidation before bronchopneumonic spread to different lobes of the identical and opposite lungs. Liquefaction necrosis and cavitation may happen early in areas of consolidation and may or may not depart significant residual scarring. Secondary plague pneumonia, which occurs in 10�15% of bubonic plague cases within the United States, usually manifests first as diffuse interstitial pneumonitis in which sputum manufacturing is scant; as a result of the sputum is extra more probably to be inspissated and tenacious in character than the sputum found in primary pneumonia, it could be less infectious. In the United States in 1947�2001, 46 instances of secondary pneumonic plague and 8 circumstances of primary pneumonic plague have been described, with no recognized transmission to contacts and an total case-fatality rate of 41%. In the United States, there were 17 meningitis instances among the many 409 evaluable plague circumstances reported during 1947�2005. All circumstances of meningitis had been complications of bubonic plague, and all but three patients survived. Although meningitis could also be a part of the preliminary presentation of plague, its onset is commonly delayed and is a manifestation of insufficient treatment. Recent cases in the United States have occurred in affiliation with remedy of bubonic plague with tetracyclines, that are bacteriostatic against Y. Chronic relapsing meningeal plague over intervals of weeks and even months was described within the preantibiotic era. The affected patients sometimes current with fever, headache, meningismus, and neutrophilic pleocytosis. Plague Pharyngitis Plague pharyngitis presents as fever, sore throat, cervical lymphadenitis, and headache and is commonly indistinguishable clinically from pharyngitis and tonsillitis of different infectious etiologies, especially streptococcal pharyngitis. Plague pharyngitis may be tough to distinguish from cervical bubonic plague arising from an infective flea bite on the head and neck area. When the diagnosis of plague is being thought-about, shut communication between clinicians and the diagnostic laboratory and between the diagnostic laboratory and a certified reference laboratory is crucial. Tests for plague are extremely dependable when conducted by laboratory personnel skilled with Y. When plague is suspected, specimens must be collected promptly for laboratory studies, chest roentgenograms should be obtained, and specific antimicrobial remedy ought to be initiated pending confirmation. Since early buboes are sometimes exquisitely tender and are seldom fluctuant or necrotic, they normally require aspiration underneath local anesthesia after the injection of 1�2 mL of normal saline (sterile however nonbacteriostatic) into the bubo with a 20- to 22-gauge needle. A variety of appropriate culture media (including brainheart infusion broth, sheep blood agar, and MacConkey agar) must be inoculated with a portion of each specimen. When a affected person dies and plague is suspected, acceptable post-mortem tissues for tradition, direct fluorescent antibody testing, and immunohistochemical staining embody buboes, all strong organs (especially liver, spleen, and lung), and bone marrow.
Infants and aged adults are mostly stricken impotence yoga postures proven silvitra 120 mg, and the severity of systemic toxicity varies xeloda impotence purchase 120 mg silvitra with mastercard. In the absence of those findings impotence for erectile dysfunction causes 120 mg silvitra cheap mastercard, the bacterial etiology of cellulitis is troublesome to set up, and in some circumstances staphylococcal and streptococcal cellulitis might have similar features. Even with needle aspiration of the main edge or a punch biopsy of the cellulitis tissue itself, cultures are positive in solely 20% of cases. This statement means that comparatively low numbers of micro organism may cause cellulitis and that the increasing space of erythema within the skin could additionally be a direct impact of extracellular toxins or of the soluble mediators of irritation elicited by the host. Bacteria might gain access to the dermis via cracks within the pores and skin, abrasions, cuts, burns, insect bites, surgical incisions, and intravenous catheters. Recurrent streptococcal cellulitis of the lower extremities may be brought on by organisms of group A, C, or G in affiliation with persistent venous stasis or with saphenous venectomy for coronary artery bypass surgical procedure. It is unclear whether or not this form of cellulitis will (like meningitis) turn out to be much less frequent as a outcome of the impressive efficacy of the H. Fortunately, these organisms occur in such characteristic settings that a good historical past offers useful clues to the diagnosis. Sites of cellulitis and abscesses related to canine bites and human bites additionally comprise a big selection of anaerobic organisms, including Fusobacterium, Bacteroides, aerobic and anaerobic streptococci, and Eikenella corrodens. Pasteurella is notoriously proof against dicloxacillin and nafcillin but is sensitive to all other -lactam antimicrobial agents, in addition to to quinolones, tetracycline, and erythromycin. Ampicillin/clavulanate, ampicillin/sulbactam, and cefoxitin are good selections for the therapy of animal or human chew infections. Treatment consists of surgical inspection and drainage, particularly if the damage also entails bone or joint capsule. Cultures and sensitivity tests are critically necessary on this setting because of multidrug resistance (Chap. The gram-positive cardio rod Erysipelothrix rhusiopathiae is most frequently related to fish and domestic swine and causes cellulitis primarily in bone renderers and fishmongers. Its resistance to vancomycin, which is unusual amongst gram-positive micro organism, is of potential clinical significance since this agent is typically used in empirical therapy for skin infection. With development, dark-red induration of the epidermis appears, together with bullae crammed with blue or purple fluid. The portal can be a malignancy, diverticulum, hemorrhoid, anal fissure, or urethral tear. It usually begins deep at the website of a nonpenetrating minor trauma, similar to a bruise or a muscle strain. In 20�40% of circumstances, myositis happens concomitantly, and, as in fuel gangrene (see later), serum creatine phosphokinase ranges could additionally be markedly elevated. Spontaneous nontraumatic gangrene amongst patients with neutropenia, gastrointestinal malignancy, diverticulosis, or recent radiation therapy to the stomach is brought on by a number of clostridial species, of which C. Synergistic nonclostridial anaerobic myonecrosis, also called necrotizing cutaneous myositis and synergistic necrotizing cellulitis, is a variant of necrotizing fasciitis brought on by combined cardio and anaerobic bacteria with the exclusion of clostridial organisms (see "Necrotizing Fasciitis" earlier within the chapter). However, even the astute clinician might find it difficult to diagnose all infections of the soft tissues by history and inspection alone. These exams are notably priceless for outlining a localized abscess or detecting fuel in tissue. Although myalgia can happen in most of those infections, extreme muscle pain is the hallmark of pleurodynia (coxsackievirus B), trichinellosis, and bacterial an infection. Acute rhabdomyolysis predictably happens with clostridial and streptococcal myositis, however may also be associated with influenza virus, echovirus, coxsackievirus, Epstein-Barr virus, and Legionella infections. Most, but not all, erythromycin-resistant group A streptococci are vulnerable to clindamycin. Approximately 90�95% of Staphylococcus aureus strains are sensitive to clindamycin. Aspiration of the main edge or punch biopsy with frozen part may be helpful if the results are positive, but false-negative outcomes happen in 80% of cases. There is a few evidence that aspiration alone could also be superior to injection and aspiration with regular saline. This chapter supplies an strategy to diagnosis and understanding of the pathophysiologic mechanisms concerned in these infections. N Engl J Med 340:eighty five, 1999 A full description of the therapy of all of the clinical entities described herein is past the scope of this chapter. As a information to the clinician in deciding on acceptable treatment, the antimicrobial agents useful in the most common and probably the most fulminant cutaneous infections are listed in Table 21-2. Appropriate empirical antibiotic remedy for blended aerobicanaerobic infections may encompass ampicillin/sulbactam, cefoxitin, or the next mixture: (1) clindamycin (600�900 mg intravenously every eight h) or metronidazole (750 mg every 6 h) plus (2) ampicillin or ampicillin/ sulbactam (2�3 g intravenously each 6 h) plus (3) gentamicin (1. Group A streptococcal and clostridial an infection of the fascia and/or muscle carries a mortality rate of 20�50% with penicillin remedy. In experimental fashions of streptococcal and clostridial necrotizing fasciitis/myositis, clindamycin has exhibited markedly superior efficacy, however no comparative trials have been carried out in people. Hyperbaric oxygen therapy can also be useful in gas gangrene as a end result of clostridial species. As a helpful framework for evaluating a patient and planning therapy, circumstances are categorized on the basis of the causative agent; the route by which organisms achieve access to bone; the period of infection; the anatomic location of infection; and the native and systemic host elements which have a bearing on pathogenesis and consequence. Trauma, ischemia, and foreign our bodies improve the susceptibility of bone to microbial invasion by exposing websites to which micro organism can bind and by impeding host defenses. Phagocytes try to include the an infection and, within the course of, release enzymes that lyse bone. Bacteria escape host defenses by adhering tightly to broken bone, by getting into and persisting within osteoblasts, and by coating themselves and underlying surfaces with a protective polysaccharide-rich biofilm. Pus spreads into vascular channels, raising intraosseous pressure and impairing the circulate of blood; as the untreated infection turns into chronic, ischemic necrosis of bone results in the separation of large devascularized fragments (sequestra). When pus breaks by way of the cortex, subperiosteal or soft tissue abscesses form, and the elevated periosteum deposits new bone (an involucrum) across the sequestrum. Microorganisms, infiltrates of neutrophils, and congested or thrombosed blood vessels are the principal histologic findings of acute osteomyelitis. The distinguishing characteristic of chronic osteomyelitis is necrotic bone, which is characterised by the absence of residing osteocytes. Mononuclear cells predominate in continual infections, and granulation and fibrous tissues exchange bone that has been resorbed by osteoclasts. A history is commonly obtained of recent blunt trauma to the realm concerned; presumably, this occasion ends in a small intraosseous hematoma or vascular obstruction that predisposes to infection. Adults with hematogenous osteomyelitis may current either in the context of an infection elsewhere. Plain radiographs obtained early in the middle of infection may show delicate tissue swelling, however the first change in bone-a periosteal reaction-is not evident till no less than 10 days after the onset of infection. Lytic modifications may be detected only after 2�6 weeks, when 50�75% of bone density has been misplaced. Bacteria settle in the well-perfused metaphysis of growing bones, a community of venous sinusoids slows the move of blood, and fenestrations in capillaries permit organisms to escape into the extravascular space. Because vascular anatomy modifications with age, hematogenous infection of long bones is unusual throughout maturity and, when it happens, often entails the diaphysis. On presentation, the child with osteomyelitis usually seems acutely ill, with fever, chills, localized pain and tenderness, and-in many cases-restriction of motion or difficulty bearing weight. During infancy and after puberty, an infection might unfold by way of the epiphysis into the joint house. In youngsters of other ages, extension of an infection via the cortex results in involvement of joints if the metaphysis is intracapsular. Organisms reach the wellperfused vertebral physique through spinal arteries and shortly spread from the top plate into the disk space and then to the adjoining vertebral physique. Diabetes mellitus requiring insulin injection, a recent invasive medical procedure, hemodialysis, and injection drug use carry an elevated risk of spinal infection. Many patients have a history of degenerative joint disease involving the backbone, and some report an episode of trauma previous the onset of infection. Penetrating injuries and surgical procedures involving the spine could cause nonhematogenous vertebral osteomyelitis or infection localized to a disk. Most sufferers with vertebral osteomyelitis report neck or again ache; sufferers might describe atypical ache within the chest, the stomach, or an extremity that is because of irritation of nerve roots. More than 50% of sufferers experience a subacute sickness in which a imprecise, uninteresting ache progressively intensifies over 2�3 months. Fever is usually low-grade or absent, however some patients recall having had an episode of fever and chills earlier than or on the onset of pain.
It has been estimated that two-thirds to three-fourths of circumstances of acute respiratory diseases are caused by viruses erectile dysfunction treatment honey 120 mg silvitra trusted. The overwhelming majority of these viral infections contain the upper respiratory tract erectile dysfunction with ms silvitra 120 mg purchase fast delivery, however decrease respiratory tract illness also can develop erectile dysfunction doctors augusta ga purchase silvitra 120 mg without prescription, particularly in youthful age teams, within the elderly, and in sure epidemiologic settings. The sicknesses caused by respiratory viruses historically have been divided into a quantity of distinct syndromes, such because the "common cold," pharyngitis, croup (laryngotracheobronchitis), tracheitis, bronchiolitis, bronchitis, and pneumonia. Each of these common categories of illness has a certain epidemiologic and medical profile; for example, croup occurs completely in very young youngsters and has a attribute scientific course. Some kinds of respiratory sickness are extra doubtless to be related to sure viruses. The syndromes most commonly related to infections with the main respiratory virus groups are summarized in Table 87-1. Moreover, the scientific sicknesses induced by these viruses are hardly ever sufficiently distinctive to permit an etiologic prognosis on scientific grounds alone, though the epidemiologic setting will increase the likelihood that one group of viruses rather than one other is involved. In general, laboratory strategies must be relied on to set up a particular viral analysis. This chapter critiques viral infections caused by six of the main teams of respiratory viruses: rhinoviruses, coronaviruses, respiratory syncytial viruses, metapneumoviruses, parainfluenza viruses, and adenoviruses. Herpesviruses, which often cause pharyngitis and which additionally trigger decrease respiratory tract illness in immunosuppressed sufferers, are reviewed in Chap. Enteroviruses, which account for infrequent respiratory diseases during the summer season months, are reviewed in Chap. Rhinoviruses grow preferentially at 33��34�C (the temperature of the human nasal passages) quite than at 37�C (the temperature of the decrease respiratory tract). These infections are most often launched into families by preschool or grade-school youngsters <6 years old. Of initial diseases in family settings, 25�70% are adopted by secondary cases, with the best assault rates among the youngest siblings at house. Rhinoviruses appear to spread via direct contact with contaminated secretions, often respiratory droplets. In some research of volunteers, transmission was best by hand-to-hand contact, with subsequent self-inoculation of the conjunctival or nasal mucosa. By adulthood, almost all people have neutralizing antibodies to a number of serotypes, though the prevalence of antibody to anybody serotype varies extensively. Relatively limited info is on the market on the histopathology and pathogenesis of acute 768 rhinovirus infections in humans. Examination of biopsy specimens obtained during experimentally induced and naturally occurring sickness indicates that the nasal mucosa is edematous, is often hyperemic, and-during acute illness- is covered by a mucoid discharge. Virus shedding coincides with the onset of illness or might start shortly earlier than signs develop. Therapy within the type of first-generation antihistamines and nonsteroidal anti-inflammatory medicine may be helpful in sufferers with significantly pronounced symptoms, and an oral decongestant could also be added if nasal obstruction is especially troublesome. Systemic indicators and symptoms, such as malaise and headache, are delicate or absent, and fever is unusual. Rhinoviruses may trigger exacerbations of asthma and persistent pulmonary disease in adults. The vast majority of rhinovirus infections resolve without sequelae, but complications related to obstruction of the eustachian tubes or sinus ostia, together with otitis media or acute sinusitis, can develop. Rather, rhinovirus infection is recognized by isolation of the virus from nasal washes or nasal secretions in tissue culture. Given the numerous serotypes of rhinovirus, prognosis by serum antibody exams is currently impractical. Experimental vaccines to sure rhinovirus serotypes have been generated, but their usefulness is questionable due to the myriad serotypes and the uncertainty about mechanisms of immunity. Thorough hand washing, environmental decontamination, and protection towards autoinoculation might help to reduce rates of transmission of an infection. The name derives from the crownlike look produced by the club-shaped projections that stud the viral envelope. Coronaviruses infect all kinds of animal species and have been divided into three antigenic teams. In basic, human coronaviruses have been difficult to domesticate in vitro, and a few strains grow solely in human tracheal organ cultures rather than in tissue culture. Some ill people ("superspreaders") appeared to be hyperinfectious and had been capable of transmitting infection to 10�40 contacts, though most infections resulted in spread either to no one or to three or fewer individuals. The outbreak apparently started in southern China and ultimately resulted in 8096 recognized cases in 28 nations in Asia, Europe, and North and South America; ~90% of instances occurred in China and Hong Kong. The outbreak ceased in 2003; 17 circumstances had been detected in 2004, largely in laboratory-associated settings, and no circumstances have been reported in 2005�2006. Clusters of circumstances recommend that spread could happen by each giant and small aerosols and maybe by the fecal-oral route as properly. Viral replication leads to harm of ciliated cells and induction of chemokines and interleukins, with consequent common-cold signs just like those induced by rhinoviruses. Virus persists in the respiratory tract for 2�3 weeks, and titers peak ~10 days after the onset of systemic sickness. Pulmonary pathology consists of hyaline membrane formation, desquamation of pneumocytes in alveolar areas, and an interstitial infiltrate made up of lymphocytes and mononuclear cells. Chest x-rays can show quite a lot of infiltrates, together with patchy areas of consolidation-most regularly in peripheral and decrease lung fields-or interstitial infiltrates, which can progress to diffuse involvement. Risk elements for extreme disease embrace an age of >50 years and comorbidities similar to heart problems, diabetes, or hepatitis. In studies of volunteers, the mean incubation period of colds induced by coronaviruses (3 days) is somewhat longer than that of sickness caused by rhinoviruses, and the duration of illness is somewhat shorter (mean, 6�7 days). The left lower lung infiltrate seen initially (A) progressed to multiple bilateral opacities (B). Total white blood cell counts are regular or barely low, and thrombocytopenia may develop because the sickness progresses. Elevated serum levels of aminotransferases, creatine kinase, and lactate dehydrogenase have been reported. These analysis procedures can be utilized to detect coronaviruses in uncommon medical settings. Because of recommendations that immunopathology could contribute to the disease, glucocorticoids have additionally been widely used, but their benefit, if any, is likewise unestablished. Supportive care to preserve pulmonary and different organ system capabilities remains the mainstay of therapy. The approach to the therapy of frequent colds brought on by coronaviruses is much like that mentioned above for rhinovirus-induced diseases. Vaccines have been developed in opposition to several animal coronaviruses but not in opposition to recognized human coronaviruses. Antigenic variety is mirrored by differences within the G protein, whereas the F protein is highly conserved. Both antigenic groups can circulate simultaneously in outbreaks, though there are usually alternating patterns in which one subgroup predominates over 1- to 2-year intervals. Infections with group B viruses may be somewhat milder than these with group A viruses. Rates of illness are highest among infants 1�6 months of age, peaking at 2�3 months of age. The attack charges amongst susceptible infants and children are extraordinarily excessive, approaching 100% in settings such as day-care centers where giant numbers of susceptible infants are present. Severe lower respiratory tract disease with pneumonitis can occur in elderly (often institutionalized) adults and in sufferers with immunocompromising issues or treatment, together with recipients of stem-cell and solid-organ transplants. The incubation interval is ~4�6 days, and virus shedding might last for 2 weeks in kids and for shorter durations in adults. Severe bronchiolitis or pneumonia is characterized by necrosis of the bronchiolar epithelium and a peribronchiolar infiltrate of lymphocytes and mononuclear cells. Studies of experimentally induced disease in healthy volunteers point out that the presence of nasal IgA neutralizing antibody correlates more carefully with safety than does the presence of serum antibody.
It is worth mentioning erectile dysfunction causes n treatment 120 mg silvitra order otc, nevertheless impotence jelqing purchase 120 mg silvitra overnight delivery, that patients undergoing intensive chemotherapy for any form of most cancers may have not solely defects due to impotence over 60 silvitra 120 mg generic online granulocytopenia but in addition lymphocyte dysfunction, which may be profound. Thus these patients-especially those receiving glucocorticoid-containing regimens or drugs that inhibit T-cell activation or cytokine induction- ought to be given prophylaxis for Pneumocystis pneumonia. Neutropenic sufferers are unusually prone to an infection with a wide variety of bacteria; thus antibiotic remedy ought to be initiated promptly to cover probably pathogens if an infection is suspected. Because remedy with narrowspectrum agents results in infection with organisms not coated by the antibiotics used, the preliminary routine ought to target pathogens prone to be preliminary causes of bacterial an infection in neutropenic hosts. Many of the related research involved small populations by which the outcomes had been generally good, and most lacked the statistical power to detect differences among the regimens studied. Each febrile neutropenic patient must be approached as a unique downside, with explicit attention given to earlier infections and up to date antibiotic exposures. Several common tips are useful within the initial remedy of neutropenic sufferers with fever. An aminoglycoside or an antibiotic with out good activity against gram-positive organisms. The initial antibacterial routine ought to be refined on the premise of tradition results. Blood cultures are essentially the most related on which to base therapy; floor cultures of skin and mucous membranes may be misleading. Simply including one other antibiotic for concern that a gram-negative an infection is current is a doubtful follow. The synergy exhibited by -lactams and aminoglycosides in opposition to sure gram-negative organisms (especially P. Cephalosporins may cause bone marrow suppression, and vancomycin is associated with neutropenia in some healthy people (Chap. Furthermore, the addition of multiple cephalosporins might induce -lactamase production by some organisms; cephalosporins and double -lactam combinations ought to most likely be avoided altogether in Enterobacter infections. For a long time it has been widespread scientific apply to add amphotericin B to antibacterial regimens if a neutropenic patient stays febrile despite 4�7 days of treatment with antibacterial agents. However, because of the high value of the lipid preparations, their use at many facilities is reserved for sufferers who fail to respond to commonplace amphotericin B. Although fluconazole is efficacious in the therapy of infections due to many Candida spp. In reality, experience indicates that these medication might nicely supplant amphotericin B as the mainstay of remedy due to their lesser toxicity and better penetration into cerebrospinal fluid and other sites. Clinicians ought to be aware that the spectrum of each azole is somewhat totally different and that no drug could be assumed to be efficacious in opposition to all fungi. Recent studies suggest a task for posaconazole as a prophylactic agent in patients with prolonged neutropenia. Echinocandins (such as caspofungin) are useful in the therapy of infections caused by azole-resistant Candida. Studies in progress are assessing using these brokers in combos to determine whether or not remedy with a quantity of antifungal brokers leads to better outcomes. Although medical experience is most intensive with acyclovir, which can be utilized therapeutically or prophylactically, numerous derivative medicine provide advantages over this agent (Table 11-8). Although vaccination with influenza vaccine is beneficial (see below), it could be ineffective on this affected person inhabitants. The availability of antiviral drugs with activity towards influenza viruses gives the clinician extra choices for the remedy of these patients (Table 11-9). The cytokines themselves could have adverse effects, including fever, hypoxemia, and pleural effusions or serositis in other areas. The function of other cytokines (such as macrophage colony-stimulating factor for monocytes or interferon-) in stopping or treating infections in granulocytopenic patients is under investigation. Counseling of sufferers to avoid leftovers, deli foods, and unpasteurized dairy merchandise is really helpful. The affiliation between spore counts and risk of an infection suggests the necessity for a high-efficiency airhandling system in hospitals that care for large numbers of neutropenic patients. Surgeons who specialize in most cancers surgical procedure can provide specific guidelines for the care of such patients, and patients benefit from commonsense recommendation about how to stop infections in susceptible areas. Fluconazole prevents Candida infections when given prophylactically to sufferers receiving bone marrow transplants. Purified proteins and inactivated vaccines are virtually never contraindicated and ought to be given to sufferers even during chemotherapy. For example, all adults should receive diphtheria-tetanus toxoid boosters on the indicated instances as nicely as seasonal influenza vaccine. If sufferers are expected to be receiving chemotherapy for several months and vaccination is indicated (for instance, influenza vaccination within the fall), the vaccine must be given midcycle-as far aside in time as possible from the antimetabolic agents that can stop an immune response. The meningococcal and pneumococcal polysaccharide vaccines should be given to patients earlier than splenectomy, if possible. Infections after transplantation are sophisticated by the use of medicine which may be necessary to improve the chance of survival of the transplanted organ, but that also cause the host to be immunocompromised. Thus what might need been a latent or asymptomatic an infection in an immunocompetent donor or in the recipient before therapy can turn out to be a life-threatening drawback when the recipient becomes immunosuppressed. Careful attention to the sterility of the medium used to process the organ mixed with meticulous microbiologic analysis reduces charges of transmission of bacteria that may be current or develop within the organ tradition medium. From 2% to >20% of donor kidneys are estimated to be contaminated with bacteria-in most instances, with the organisms that colonize the pores and skin or grow within the tissue tradition medium used nedasalamatebook@gmail. In hematopoietic stem-cell transplant recipients, acute pulmonary disease can also happen. The reported price of bacterial contamination of transplanted stem cells (bone marrow, peripheral blood, cord blood) is as excessive as 17% however is most commonly 1%. The use of enrichment columns and monoclonal-antibody depletion procedures leads to a higher incidence of contamination. In one series of sufferers receiving contaminated products, 14% had fever or bacteremia, however none died. In many transplantation centers, transmission of infections that could be latent or clinically inapparent within the donor organ has resulted within the development of specific donor-screening protocols. Because of immune dysfunction ensuing from chemotherapy or nedasalamatebook@gmail. This chapter considers aspects of infection distinctive to varied transplantation settings. Immediately after transplantation, both phagocytes and adaptive immune cells (T and B cells) are absent, and the host is extremely vulnerable to an infection. Nevertheless, most infections occur in a predictable timeframe after transplantation (Table 12-2). Beyond the primary few days of neutropenia, infections with filamentous micro organism corresponding to Nocardia turn into extra widespread. Episodes of bacteremia due to encapsulated organisms mark the late posttransplantation interval (>6 months after hematopoietic stem-cell reconstitution). Because of the anticipated 1- to 3-week duration of neutropenia and the excessive rate of bacterial infection on this inhabitants, many centers give prophylactic antibiotics to patients upon initiation of myeloablative remedy. Quinolones decrease the incidence of gram-negative bacteremia amongst these sufferers. As in most granulocytopenic sufferers, Candida infections are mostly seen on this setting. With elevated use of prophylactic fluconazole, infections with resistant fungi-in explicit, Aspergillus and other molds (Fusarium, Scedosporium, Penicillium)-have become extra common, prompting some facilities to substitute fluconazole with agents corresponding to caspofungin, voriconazole, and posaconazole. The function of antifungal prophylaxis with these completely different brokers, in distinction to empirical therapy for suspected or documented an infection, stays controversial (Chap. Prolonged use of central venous catheters for parenteral nutrition (lipids) will increase the chance of fungemia with Malassezia. Varicella-Zoster Virus Reactivation of herpes zoster might happen inside the first month, however more commonly occurs a number of months after transplantation. Reactivation charges are 40% for allogeneic recipients and 25% for autologous recipients. Some data suggest that administration of low doses of acyclovir for a whole 12 months after transplantation is efficient and should remove most instances of posttransplantation zoster. A positive take a look at (or rising viral load) prompts the initiation of preemptive remedy.
Vitamin K1: Methylphytyl Naphthoquinone (Vitamin K). Silvitra.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96944
Numerous interventions have been examined for their capability to improve survival in patients with extreme sepsis free sample erectile dysfunction pills 120 mg silvitra buy free shipping. Unfortunately erectile dysfunction penile injections silvitra 120 mg discount on line, none of these brokers has improved rates of survival amongst sufferers with severe sepsis/septic shock in more than one giant impotence beta blockers 120 mg silvitra safe, randomized, placebo-controlled scientific trial. This lack of reproducibility has had many contributing factors, including (1) heterogeneity in the affected person populations studied and the inciting microbes and (2) the nature of the "normal" remedy also used. A dramatic example of this problem was seen in a trial of tissue issue pathway inhibitor. The drug appeared extremely efficacious at the interim evaluation in December 2000, however this trend reversed later within the trial. Demonstrating that therapeutic agents for sepsis have constant, reproducible efficacy has been extraordinarily tough, even within well-defined patient populations. Bundling of therapies obscures the efficacy and toxicity of the individual interventions and permits little room for individualizing remedy. Indiscriminate use of antimicrobial agents and glucocorticoids ought to be avoided, and optimum infectioncontrol measures (Chap. Several studies level to associations between allelic polymorphisms in specific genes and danger of extreme sepsis; if these associations prove to be broadly relevant, such polymorphisms can be utilized prospectively to identify highrisk sufferers and to goal preventive and/or therapeutic measures to them. Studies point out that 50�70% of sufferers who develop nosocomial extreme sepsis or septic shock have skilled a less extreme stage of the septic response. Research is needed to develop adjunctive agents that can damp the septic response earlier than organ dysfunction or hypotension happens. Of the individual covariates, the severity of underlying disease most strongly influences the chance of dying. Case-fatality charges are comparable for culture-positive and culture-negative severe sepsis. They are among the most typical causes for visits to primary care providers, and, although the diseases are typically delicate, their high incidence and transmission charges place them among the many main causes of time misplaced from work or faculty. The enormous consumption of antibiotics for these diseases has contributed to the rise in antibiotic resistance among common community-acquired pathogens similar to Streptococcus pneumoniae-a trend that in itself has had an unlimited influence on public health. Because routine, speedy testing is neither out there nor practical for most syndromes, acute infections are identified largely on scientific grounds. Other manifestations, corresponding to fever, malaise, sneezing, and hoarseness, are extra variable, with fever extra common among infants and younger children. Occasionally, clinical features reflect the underlying viral pathogen; myalgias and fatigue, for example, are sometimes seen with influenza and parainfluenza infections, whereas conjunctivitis may suggest an infection with adenovirus or enterovirus. Secondary bacterial infections are normally related to a prolonged course of sickness, increased severity of illness, and localization of indicators and signs. Purulent secretions from the nares or throat have typically been used as an indication of sinusitis or pharyngitis. They are identified by a big selection of descriptive names, including acute infective rhinitis, acute rhinopharyngitis/nasopharyngitis, acute coryza, and acute nasal catarrh, as properly as by the inclusive label widespread cold. In the absence of scientific proof of bacterial infection, therapy stays completely symptom-based, with use of decongestants and nonsteroidal anti-inflammatory medication. Other therapies directed at particular signs are sometimes useful, including dextromethorphan for cough and lozenges with topical anesthetic for sore throat. Although most instances of sinusitis involve multiple sinus, the maxillary sinus is most commonly concerned; subsequent in frequency are the ethmoid, frontal, and sphenoid sinuses. When the sinus ostia are obstructed, nevertheless, or when ciliary clearance is impaired or absent, the secretions can be retained, producing the standard signs and signs of sinusitis. The retained secretions might turn into contaminated with a wide selection of pathogens, together with viruses, micro organism, and fungi. Sinusitis impacts an amazing proportion of the inhabitants, accounts for millions of visits to main care physicians each year, and is the fifth main diagnosis for which antibiotics are prescribed. Differentiating acute bacterial and viral sinusitis on clinical grounds is difficult. Etiology A number of infectious and noninfectious factors can contribute to acute obstruction of the sinus ostia or impairment of ciliary clearance, with consequent sinusitis. Noninfectious causes embrace allergic rhinitis (with both mucosal edema or polyp obstruction), barotrauma. In the hospital setting, nasotracheal intubation is a serious threat factor for nosocomial sinusitis in intensive care models. Acute infectious sinusitis may be brought on by a wide selection of organisms, including viruses, bacteria, and fungi. In these studies that have done so, the viruses most commonly isolated-both alone and with bacteria-have been rhinovirus, parainfluenza virus, and influenza virus. Moraxella catarrhalis causes illness in a big share (20%) of youngsters however less typically in adults. Anaerobes are sometimes found in affiliation with infections of the roots of premolar enamel that unfold into the adjacent maxillary sinuses. The position of Chlamydophila pneumoniae and Mycoplasma pneumoniae within the pathogenesis of acute sinusitis is still unclear. Nosocomial circumstances are generally associated with micro organism found within the hospital surroundings, including S. Often, these infections are polymicrobial and contain organisms which are highly resistant to quite a few antibiotics. Fungi are additionally established causes of sinusitis, though most acute cases are in immunocompromised sufferers and symbolize invasive, life-threatening infections. The best-known example is rhinocerebral mucormycosis attributable to fungi of the order Mucorales, which includes Rhizopus, Rhizomucor, Mucor, Absidia, and Cunninghamella. These infections normally occur in diabetic sufferers with ketoacidosis but in addition develop in transplant recipients, sufferers with hematologic malignancies, and sufferers receiving persistent glucocorticoid or deferoxamine therapy. Other hyaline molds, similar to Aspergillus and Fusarium species, are additionally occasional causes of this illness. A large proportion of patients with colds have sinus irritation, though bacterial sinusitis complicates solely 0. Common presenting symptoms of sinusitis embrace nasal drainage and congestion, facial ache or strain, and headache. Tooth ache, most frequently involving the upper molars, is related to bacterial sinusitis, as is halitosis. Although uncommon, manifestations of superior sphenoid or ethmoid sinus an infection may be profound, together with severe frontal or retroorbital pain radiating to the occiput, thrombosis of the cavernous sinus, and signs of orbital cellulitis. Acute focal sinusitis is unusual however must be considered in the patient with severe symptoms over the maxillary sinus and fever, no matter sickness duration. Lifethreatening issues embrace meningitis, epidural abscess, and cerebral abscess. Patients with acute fungal sinusitis (such as mucormycosis) often current with signs associated to strain results, significantly when the infection has spread to the orbits and cavernous sinus. Signs corresponding to orbital swelling and cellulitis, proptosis, ptosis, and decreased extraocular movement are widespread, as is retroorbital or periorbital pain. Because remedy should goal the offending organism, a sinus aspirate must be obtained, if potential, for culture and susceptibility testing. One scientific feature that has been used to help guide diagnostic and therapeutic determination making is illness duration. Because acute bacterial sinusitis is unusual in sufferers whose symptoms have lasted <7 days, a number of authorities now advocate reserving this analysis for sufferers with "persistent" symptoms. Even among the many patients who meet these criteria, only 40�50% have true bacterial sinusitis. The scientific history and/or setting can typically establish circumstances of acute anaerobic bacterial sinusitis, acute fungal sinusitis, or sinusitis from noninfectious causes. In the case of an immunocompromised Most patients with a prognosis of acute rhinosinusitis based on clinical grounds enhance with out antibiotic remedy. The most well-liked initial strategy in sufferers with gentle to moderate signs of brief length is therapy aimed toward facilitating sinus drainage, corresponding to oral and topical decongestants, nasal saline lavage, and-in sufferers with a historical past of chronic sinusitis or allergies- nasal glucocorticoids. Empirical therapy ought to encompass the narrowest-spectrum agent active against the most typical bacterial pathogens, together with S. No medical trials support the utilization of broad-spectrum brokers for routine cases of bacterial sinusitis, even within the present era of drugresistant S.
In immunocompromised hosts new erectile dysfunction drugs 2014 silvitra 120 mg cheap, varicella vesicles could lack the attribute erythematous base or could seem hemorrhagic webmd erectile dysfunction treatment generic 120 mg silvitra free shipping. However erectile dysfunction doctors in queens ny purchase 120 mg silvitra free shipping, hot-tub folliculitis usually occurs in outbreaks after bathing in scorching tubs or swimming pools, and lesions happen in regions occluded by bathing suits. Variola lesions are most distinguished on the face and extremities, whereas varicella lesions are most distinguished on the trunk. Primary herpes infection is accompanied by fever and toxicity, whereas recurrent disease is milder. In the presence of fever, urticarial eruptions are normally due to urticarial vasculitis. Unlike particular person lesions of traditional urticaria, which last as lengthy as forty eight h, these lesions may last as long as 5 days. Etiologies include serum illness (often induced by medication such as penicillins, sulfas, salicylates, or barbiturates), connective-tissue disease. Patients with disseminated candidiasis (often due to Candida tropicalis) might have a triad of fever, myalgias, and eruptive nodules (Chap. Purpuric nodules might develop on the legs and resemble erythema nodosum but lack its exquisite tenderness. The lesions of persistent meningococcemia and those of gonococcemia could also be indistinguishable when it comes to look and distribution. Cutaneous small-vessel vasculitis (leukocytoclastic vasculitis) sometimes manifests as palpable purpura and has a extensive variety of causes. For instance, the presence of an eschar might counsel the prognosis of scrub typhus or rickettsialpox (Chap. Clin Infect Dis sixteen:199, 1993 -: Cutaneous manifestations of systemic infections, in Textbook of Pediatric Infectious Diseases, vol. The newer definition is broader, stipulating three outpatient visits or three days within the hospital without elucidation of a trigger or 1 week of "clever and invasive" ambulatory investigation. Coincident with the widespread use of antibiotics, more and more useful diagnostic technologies-both noninvasive and invasive-have been developed. Likewise, the widespread availability of extremely particular and delicate immunologic testing has reduced the number of undetected instances of systemic lupus erythematosus and different autoimmune ailments. Intraabdominal abscesses (sometimes poorly localized) and renal, retroperitoneal, and paraspinal abscesses continue to be troublesome to diagnose. It is associated with intracellular bacterial an infection, is seen most frequently in sufferers with defects of intracellular bacterial killing, and is treated with fluoroquinolones or trimethoprim-sulfamethoxazole. Osteomyelitis, particularly the place prosthetic gadgets have been implanted, and infective endocarditis must be considered. Prostatitis, dental abscesses, sinusitis, and cholangitis continue to be sources of occult fever. Virtually all lessons of medication trigger fever, but antimicrobial agents (especially -lactam antibiotics), cardiovascular medicine. It is axiomatic that, as the duration of fever will increase, the chance of an infectious cause decreases, even for the extra indolent infectious etiologies. In a sequence of 347 sufferers referred to the National Institutes of Health from 1961 to 1977, solely 6% had an an infection (Table 9-2). A substantial number of these factitious cases had been in younger ladies in the well being professions. A total of 27% of patients had no actual fever during inpatient remark or had an exaggerated circadian temperature rhythm without chills, elevated pulse, or different abnormalities. The frequency of world travel underscores the need for an in depth journey history, and the continuing emergence of new infectious ailments makes this itemizing doubtlessly incomplete. The chance of worldwide and home terrorist activity involving the intentional launch of infectious agents, many of which cause diseases presenting with extended fever, underscores the need for obtaining an insightful environmental, occupational, and skilled history, with early notification of public well being authorities in circumstances of suspicious etiology (Chap. In this flow chart, reference is made to "probably diagnostic clues," as outlined by de Kleijn and colleagues; these clues may be key findings within the historical past. Certain specific diagnostic maneuvers turn out to be critical in dealing with prolonged fevers. If factitious fever is suspected, digital thermometers should be used, temperature-taking must be supervised, and simultaneous urine and body temperatures must be measured. Thick blood smears should be examined for Plasmodium; thin blood smears, prepared with correct method and quality stains and subjected to expert microscopy, should be used to speciate Plasmodium and to identify Babesia, Trypanosoma, Leishmania, Rickettsia, and Borrelia. Any tissue removed throughout prior related surgery should be reexamined; slides must be requested, and, if want be, paraffin blocks of mounted pathologic materials should be reexamined and extra particular research performed. Relevant x-rays should be reexamined; reviewing of prior radiologic reports may be insufficient. Serum must be set aside within the laboratory as quickly as attainable and retained for future examination for rising antibody titers. Lysiscentrifugation blood culture methods should be employed in instances the place prior antimicrobial remedy or fungal or atypical mycobacterial infection is suspected. Blood culture media should be supplemented with L-cysteine or pyridoxal to help in the isolation of nutritionally variant streptococci. It must be noted that sequential cultures positive for a quantity of organisms may reflect self-injection of contaminated substances. Antinuclear antibody, antineutrophil cytoplasmic antibody, rheumatoid issue, and serum cryoglobulins ought to be measured to rule out other collagen vascular diseases and vasculitis. Elevated levels of angiotensin-converting enzyme in serum may level to sarcoidosis. Noninvasive procedures ought to include an upper gastrointestinal contrast study with small-bowel followthrough and colonoscopy to examine the terminal ileum and cecum. If there are pulmonary signs or symptoms, bronchoscopy with bronchoalveolar lavage for cultures and cytology should be considered. Arteriography could also be useful for patients in whom systemic necrotizing vasculitis is suspected. Saccular aneurysms could additionally be seen, most commonly in renal or hepatic vessels, and may permit prognosis of arteritis when biopsy is troublesome. Ultrasonography of the stomach is helpful for investigation of the hepatobiliary tract, kidneys, spleen, and pelvis. Echocardiography may be helpful in an analysis for bacterial endocarditis, pericarditis, nonbacterial thrombotic endocarditis, and atrial myxomas. Radionuclide scanning procedures utilizing technetium (Tc) 99m sulfur colloid, gallium (Ga) sixty seven citrate, or indium (In) 111�labeled leukocytes may be useful in identifying and/or localizing inflammatory processes. In one examine, Ga scintigraphy yielded useful diagnostic information in nearly one-third of circumstances, and it was advised that this process might really be used before other imaging methods if no specific organ is suspected of being irregular. Granulomatous hepatitis has been diagnosed by liver biopsy, even when liver enzymes are regular and no different diagnostic clues level to liver illness. Likewise, within the absence of clues pointing to the bone marrow, bone marrow biopsy (not simple aspiration) for histology and culture has yielded diagnoses late in the workup. When possible, a bit of the tissue block should be retained for additional sections or stains. Thus, in some instances, a retrospective prognosis could be made on the basis of research of long-fixed pathologic tissues. In a affected person over age 50 (or often in a younger patient) with the suitable symptoms and laboratory findings, "blind biopsy" of one or both temporal arteries may yield a diagnosis of arteritis. Tenderness or decreased pulsation, if famous, should guide the number of a site for biopsy. Lymph node biopsy may be useful if nodes are enlarged, but inguinal nodes are often palpable and are seldom diagnostically useful. Exploratory laparotomy has been performed when all different diagnostic procedures fail however has largely been replaced by imaging and guided-biopsy strategies. Laparoscopic biopsy might present more adequate guided sampling of lymph nodes or liver, with much less invasive morbidity. The original surgical or procedural subject is the place to start a directed bodily and laboratory examination for abscesses, hematomas, or contaminated international our bodies. In this setting, one of the best approach is to concentrate on sites the place occult infections could also be sequestered, such as the sinuses of intubated patients or a prostatic abscess in a person with a urinary catheter. Clostridium difficile colitis may be associated with fever and leukocytosis before the onset of diarrhea. Among these causes are acalculous cholecystitis, deep-vein thrombophlebitis, and pulmonary embolism. Drug fever, transfusion reactions, alcohol/drug withdrawal, adrenal insufficiency, thyroiditis, pancreatitis, gout, and pseudogout are among the many attainable causes to think about.
Septic cavernous sinus thrombosis follows a facial or sphenoid sinus an infection; 70% of circumstances are due to erectile dysfunction treatment with exercise cheap silvitra 120 mg with mastercard staphylococci vasodilator drugs erectile dysfunction silvitra 120 mg order without a prescription, and the remainder is due primarily to aerobic or anaerobic streptococci erectile dysfunction depression purchase 120 mg silvitra visa. Septic thrombosis of the superior sagittal sinus spreads from the ethmoid or maxillary sinuses and is caused by S. Almost half of sufferers are afebrile, and shows are more according to a space-occupying lesion in the brain; 70% of sufferers have headache, 50% have focal neurologic indicators, and 25% have papilledema. The an infection progresses over several days from cerebritis to an abscess with a mature capsule. More than half of infections are polymicrobial, with an etiology consisting of cardio micro organism (primarily streptococcal species) and anaerobes. Abscesses arising hematogenously are especially apt to rupture into the ventricular house, causing a sudden and severe deterioration in clinical status and high mortality. Patients presenting with stroke and a parameningeal infectious focus, corresponding to sinusitis or otitis, might have a mind abscess, and physicians must preserve a high level of suspicion. Prognosis worsens in sufferers with a fulminant course, delayed diagnosis, abscess rupture into the ventricles, multiple abscesses, or abnormal neurologic status at presentation. Fulminant malaria is brought on by Plasmodium falciparum and is associated with temperatures of >40�C (>104�F), hypotension, jaundice, grownup respiratory misery syndrome, and bleeding. By definition, any patient with a change in psychological standing or repeated seizure in the setting of fulminant malaria has cerebral malaria. On bodily examination, symmetric encephalopathy is typical, and higher motor neuron dysfunction with decorticate and decerebrate posturing could be seen in superior disease. Spinal Epidural Abscesses Patients with spinal epidural abscesses often present with again pain and develop neurologic deficits late of their course. The thoracic or lumbar backbone is the most common location; cervical spine infections are associated with worse outcomes. This prognosis must instantly be thought of in patients with a historical past of antecedent back pain and new neurologic signs. Paresthesia, bowel and bladder dysfunction, radicular ache, and weak spot are frequent neurologic complaints, and examination of the affected person may reveal abnormal reflexes and motor and sensory deficits. Rapid recognition and treatment, which may include surgical drainage, can forestall or minimize permanent neurologic sequelae. Rapid medical deterioration and demise can be associated with destruction of the primary web site of infection, as is seen in endocarditis and in necrotizing infections of the oropharynx (in which edema all of a sudden compromises the airway). Patients current with low-grade fever, dull sinus pain, diplopia, decreased psychological status, decreased ocular movement, chemosis, proptosis, dusky or necrotic nasal turbinates, and necrotic hard-palate lesions that respect the midline. Without speedy recognition and intervention, the method continues on an inexorable invasive course, with excessive mortality. The host may have comorbid conditions similar to underlying malignancy, diabetes mellitus, intravenous drug use, or alcoholism. The affected person presents with fever, fatigue, and malaise <2 weeks after onset of an infection. On physical examination, a altering murmur and congestive heart failure could also be noted. Rapid valvular destruction, significantly of the aortic valve, results in pulmonary edema and hypotension. Myocardial abscesses can form, eroding by way of the septum or into the conduction system and inflicting life-threatening arrhythmias or high-degree conduction block. Large friable vegetations can end result in major arterial emboli, metastatic an infection, or tissue infarction. Emboli can lead to stroke, adjustments in psychological standing, visual disturbances, aphasia, ataxia, headache, meningismus, brain abscess, cerebritis, spinal wire infarct with paraplegia, arthralgia, osteomyelitis, splenic abscess, septic arthritis, and hematuria. Pulmonary infiltrates, mediastinal widening, and pleural effusions were the commonest findings. Survival was more probably when antibiotics got during the prodromal period and if multidrug regimens have been used. However, proof of a quickly increasing geographic distribution of the virus throughout the world is of grave concern. Patients current with excessive fever, an influenza-like sickness, and lower respiratory tract signs. Dyspnea develops a median of 5 days after the onset of signs and may progress to respiratory misery syndrome, multiorgan failure, and death within 9�10 days after the onset of sickness. The alert doctor must recognize the acute infectious disease emergency and then proceed with applicable urgency. Cardiovascular: Arterial systolic syndrome") blood strain ninety mmHg or mean arterial strain 70 mmHg that responds to administration of intravenous fluid 2. Hematologic: Platelet rely <80,000/�L or 50% lower in platelet depend from highest worth recorded over previous three days 5. Sepsis is usually reversible, whereas sufferers with septic shock usually succumb regardless of aggressive remedy. In truth, blood cultures yield micro organism or fungi in solely 20�40% of instances of extreme sepsis and 40�70% of circumstances of septic shock. Individual gram-negative or gram-positive bacteria account for 70% of those isolates; the rest are fungi or a mix of microorganisms (Table 15-2). In sufferers whose blood cultures are unfavorable, the etiologic agent is usually established by culture or microscopic examination of infected materials from a neighborhood web site. In some case sequence, a majority of patients with a scientific image of extreme sepsis or septic shock have had adverse microbiologic information. The incidence of severe sepsis and septic shock has increased over the previous 20 years, and the annual variety of circumstances is now >700,000 (3 per a thousand population). Approximately twothirds of the circumstances occur in sufferers with vital underlying sickness. The widespread use of antimicrobial brokers, immunosuppressive medicine, indwelling catheters and mechanical gadgets, and mechanical air flow also plays a job. In Sub-Saharan Africa, for example, careful screening for constructive blood cultures discovered that community-acquired bacteremia accounted for at least one-fourth of deaths of children >1 yr of age. Nontyphoidal Salmonella species, Streptococcus pneumoniae, Haemophilus influenzae, and Escherichia coli had been essentially the most generally isolated bacteria. Staphylococcus aureus, coagulase-negative staphylococci, enterococci, Streptococcus pneumoniae, other streptococci, other gram-positive bacteria. Microbial pathogens, in distinction, are able to circumvent innate defenses by elaborating toxins or other virulence elements. In each circumstances, the physique can fail to kill the invaders despite mounting a vigorous inflammatory response that can lead to severe sepsis. Host Mechanisms for Sensing Microbes Animals have exquisitely delicate mechanisms for recognizing and responding to conserved microbial molecules. The ability to acknowledge sure microbial molecules could affect both the efficiency of the host protection and the pathogenesis of severe sepsis. Most of the commensal aerobic and facultatively anaerobic gramnegative micro organism that set off severe sepsis and shock (including E. When they invade human hosts, usually via breaks in an epithelial barrier, an infection is often localized to the subepithelial tissue. These mucosal commensals appear to induce extreme sepsis most often by triggering extreme local tissue irritation somewhat than by circulating throughout the bloodstream. Systemic responses are activated by neural and/or humoral communication with the hypothalamus and brainstem; these responses enhance native defenses by growing blood circulate to the contaminated space, augmenting the number of circulating neutrophils, and elevating blood ranges of quite a few molecules (such because the microbial recognition proteins discussed above) which have anti-infective capabilities. Cytokines and Other Mediators protein C�protein S inhibitory pathway and depletion of antithrombin and protein C, whereas fibrinolysis is prevented by increased plasma levels of plasminogen activator inhibitor 1. Thus there may be a hanging propensity towards intravascular fibrin deposition, thrombosis, and bleeding; this propensity has been most apparent in sufferers with intravascular endothelial infections such as meningococcemia (Chap. Local Control Mechanisms Severe Sepsis and Septic Shock Cytokines can exert endocrine, paracrine, and autocrine results. High-mobility group B-1, a transcription issue, can be launched from cells and interact with microbial merchandise to induce host responses late in the middle of the septic response. Coagulation Factors Host recognition of invading microbes inside subepithelial tissues sometimes ignites immune responses that quickly kill the invader after which subside to enable tissue recovery.






