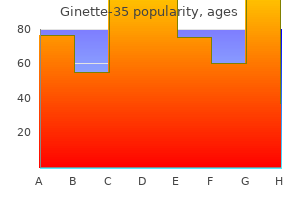
Ginette-35
Ginette-35
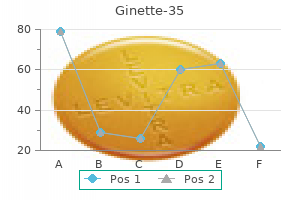
Ginette-35 dosages: 2 mg
Ginette-35 packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills
Thumb surgical procedure to lengthen the flexor pollicis longus and rebalance the extensor is the most common surgery (52) understanding women's health issues a reader discount ginette-35 2 mg otc. The outcome of remedy of clubfoot is best in this syndrome than in other arthrogrypotic clubfeet pregnancy diarrhea ginette-35 2 mg cheap overnight delivery. Scoliosis was not initially acknowledged as a typical function menstruation kits order 2 mg ginette-35 mastercard, nevertheless it affects greater than one-half of the patients. Although the scoliosis could be managed as in idiopathic scoliosis, the curves are extra inflexible and should not respond well to brace therapy (433, 435). The arms demonstrate the basic distal arthrogryposis pattern described earlier (433, 435, 436). There are different contractures, including flexion deformities of the elbow and knee, decreased range of movement of the shoulder, decreased range of motion of the neck, and dislocated hips (77). Operative management rules for the upper extremity are similar to those in distal arthrogryposis. Most of the opposite associated contractures could be handled like those in the different arthrogrypotic syndromes. Clubfoot and vertical talus deformities are difficult to handle utilizing manipulative techniques, however these ought to be tried first before utilizing operative techniques. During infancy, dysphagia and aspiration lead to failure to thrive, and even to death. Anesthesia complications are widespread; some are the results of abnormalities related to the laryngeal cartilages (76, 389, 392, 438). The trigger is unknown, however the buccinator muscle is hypoplastic, and electromyograms and muscle biopsies are equivalent to the peripheral muscle research in basic arthrogryposis multiplex congenita (440), suggesting some similarity in pathophysiology. It could be seen as an isolated malformation in some syndromes, such because the pterygium colli in the neck of patients with Klippel-Feil syndrome. There are two clinically important pterygia syndromes: multiple pterygium syndrome and popliteal pterygia syndrome (397). Several pterygium syndromes are deadly, with the affected sufferers not surviving the fetal or the new child period (398, 471). Lethal pterygium syndrome may be recognized prenatally by detecting hydrops and cystic hygroma colli (399). Both popliteal pterygium syndrome and van der Woude syndrome are caused by mutations within the gene encoding interferon regulatory factor-6 (400). Notice the small chin and mouth, long philtrum, puffy cheeks, deeply set eyes, and small chin cleft. Radiographs of the palms reveal ulnar deviation on the metacarpophalangeal joint, typical of a distal arthrogryposis syndrome. It is unclear how a mutation in this interferon regulatory issue causes these seemingly dissimilar syndromes. There are also webs throughout the neck laterally and anteriorly from sternum to chin, drawing the facial options down. The two features that differentiate this syndrome from classic arthrogryposis are vertical talus and congenital spine deformity. The vertical talus is fairly fixed in a quantity of pterygium syndrome and could be managed only by surgery. Circumferential release and extended safety, as in managing any arthrogrypotic foot deformity, are necessary. Mobility depends a lot on the magnitude of the decrease extremity webs and the residual motion of the joints, with many patients restricted to wheelchairs for locomotion. The kids have regular intelligence, and efforts must be maximized to enable them to function independently. The options embrace a cleft lip and palate, lip pits, and intraoral adhesions (52, 53). Within the popliteal web is a superficial fibrous band, over which lies a tent of muscle working from the os calcis to the ischium, and is understood in the older literature as a calcaneoischiadicus muscle. There is a distinctive foot abnormality on this syndrome: a bifid great toenail and syndactyly of the lesser toes. For example, delicate webs in joints of the upper extremity could also be found in patients with popliteal pterygium syndrome. On radiographic examination, the patella look elongated, and the femoral condyles flattened, due to knee-flexion deformity. From a management perspective, the figuring out elements are the magnitude of scoliosis and the size of the web crossing the knee. Radiograph exhibits severe scoliosis, vertebral abnormalities, and an unsegmented bar from T9 to T12 and from L1 to S1, with an apparent gap between the bars. Severe limitation of trunk development was caused by vertebral fusions and lordoscoliosis. For the lengthy term survivors, administration of the backbone deformity is similar to these with nonsyndromic congenital scoliosis. The knee is the joint that limits mobility in both syndromes and is the joint that most determines future ambulatory potential (39, 41, forty two, 76). Traditionally, remedy of the knee begins with physical remedy, however the effectiveness of this therapy is doubtful. Early popliteal net surgical procedure is beneficial earlier than the onset of adaptive adjustments within the articular surfaces, and before additional vascular shortening. The nerve is often located just under the skin and the online, and care have to be taken to avoid nerve harm. Arteriogram shows that the popliteal artery has been drawn up from its regular place. Gradual distraction techniques can be utilized, but a bonus over traditional techniques has not been demonstrated (448). Posterior soft-tissue procedures can be mixed with distraction strategies to progressively extend the knee. Femoral shortening methods are related to low recurrence rates of the deformity, and have the benefit of lowering tension on the neurovascular constructions. Center for Medical Genetics, Johns Hopkins University and National Center for Biotechnology Information. Congenital malformations in 10,000 consecutive births in a university hospital: need for genetic counseling and prenatal prognosis. Marfan syndrome as a paradigm for transcript-targeted preimplantation prognosis of heterozygous mutations. Targetting of the gene encoding fibrillin-1 recapitulates the vascular aspect of Marfan syndrome. Severe cervical kyphosis complicating halo traction in a patient with Marfan syndrome. Osseous destruction by neurofibroma diagnosed in infancy as "desmoplastic fibroma. Shortening of growing-rod spinal instrumentation reverses cardiac failure in child with Marfan syndrome and scoliosis. Understanding patellofemoral ache with maltracking in the presence of joint laxity: complete 3D in vivo patellofemoral and tibiofemoral kinematics. Vascular issues from anterior backbone surgery in three sufferers with Ehlers-Danlos syndrome. Recent progress toward understanding the molecular biology of von Recklinghausen neurofibromatosis. Paraparesis after posterior spinal fusion in neurofibromatosis secondary to rib displacement: case report and literature evaluation. Modelling neurofibromatosis sort 1 tibial dysplasia and its remedy with lovastatin. Spontaneous dislocation of a vertebra in a affected person who had neurofibromatosis: report of a case with dural ectasia. Neurofibromatosis with dural ectasia and bilateral symmetrical pedicular clefts: report of two cases. The neurofibromatosis type 1 gene and its protein product, neurofibromin [Review]. Case report: hypophosphatemic osteomalacia in von Recklinghausen neurofibromatosis. Hypercalcemic hyperparathyroidism and hypophosphatemic osteomalacia complicating neurofibromatosis.
However menstrual joy studies cheap 2 mg ginette-35 free shipping, in the process women's health richmond va generic 2 mg ginette-35 with mastercard, these cells themselves become a significant supply of proinflammatory cytokines that can mediate hepatocellular harm breast cancer deaths per year discount ginette-35 2 mg online. These circulating acute part proteins are answerable for the clinical phenomena that accompany systemic infection/inflammation in adults, including leukocytosis, fever, altered consciousness, adjustments in lipid metabolism, decreased gluconeogenesis, cachexia, insulin resistance, and muscle weak spot. The importance of this cascade in the control of systemic infection/inflammation is illustrated in a number of animal models during which manufacturing of acute section proteins is blocked. Unfortunately, the identical proinflammatory cytokines that activate the protective arm of the acute section response concurrently inhibit hepatocyte and cholangiocyte transport mechanisms, together with the sodium-dependent bile salt transporter and the multispecific natural anion transporter 2 at the hepatocyte basolateral membrane, and the bile salt export pump, which transports monovalent bile acids, and the conjugate export pump, which transports divalent bile acids, at the canalicular membrane [7]. Alterations in the hepatic microvasculature additionally contribute to sepsis-associated cholestasis. The launch of potent vasoconstrictors and bodily obstruction of the hepatic sinusoids by inflammatory cells and fibrinous microthrombi lead to endothelial cell injury and hepatocyte necrosis. Circulation to the biliary tract, depending on probably the most distal branches of the hepatic arterial tree, is especially sensitive to altered intrahepatic blood circulate. Another element of the innate immune system, the neutrophil, plays a central role within the inflammatory response to systemic an infection. Once neutrophils are activated, they disseminate throughout the physique and might become sequestered within the capillary networks of internal organs, such because the liver. Within the liver, neutrophils can contribute to vital hepatocellular damage; however, they may additionally play a protecting role. Sequestration of neutrophils within liver sinusoids could enhance bacterial trapping and clearance during sepsis, thus limiting the unfold of infection, albeit at a value to the liver itself [8]. The presence of hepatic dysfunction has little prognostic significance; the prognosis is that of the underlying disease and remedy ought to be directed at aggressively treating the first an infection and providing help for the circulatory and different organ techniques. Heart disease and circulatory failure Hepatic dysfunction occurs incessantly in kids with issues of acute or persistent circulatory compromise. Hypoxic liver injury can occur in affiliation with congestive heart failure, pericardial tamponade, hypovolemic or septic shock, cardiorespiratory arrest, asphyxia, prolonged seizures, heatstroke, or cardiopulmonary bypass. Occasionally, the clinical presentation is extreme sufficient to resemble fulminant hepatic failure. The liver is unique in possessing an afferent twin blood provide, with two-thirds of hepatic blood move made up of partially deoxygenated blood rich in vitamins and hormones arriving from the abdominal organs via the low-pressure, low-resistance portal venous system, and the remainder being well-oxygenated blood delivered by way of the high-pressure, highresistance hepatic artery. Of these two systems, only the hepatic artery supplies the main bile ducts, making the biliary tree particularly prone to altered hepatic arterial flow. As blood enters the liver via the portal triad (zone 1) and flows by way of the sinusoids (zone 2) to the central vein (zone 3), the concentrations of oxygen and different vitamins decrease. This oxygen-tension gradient in the hepatic lobule accounts for the elevated susceptibility of pericentral hepatocytes (zone 3) to necrosis associated with hypoxia or poor perfusion. Regulation of hepatic blood move occurs not solely through classic arterial autoregulation (the constrictive response of an artery in the setting of increased arterial pressure), but additionally through the hepatic arterial buffer response. This unique mechanism represents the ability of the hepatic artery to produce compensatory flow changes in response to changes in portal venous circulate. These move changes rely upon the focus of adenosine in the area of Mall, the small fluid-filled area surrounding the terminal branches of the hepatic artery and portal vein. The secretion of adenosine into the area of Mall occurs at a constant fee, whereas the washout of adenosine through the portal venules is dependent on portal flow. When portal vein circulate is lowered, the focus of adenosine will increase, leading to dilatation of the hepatic artery. Adenosine also activates sensory nerves in the area of Mall and initiates renal fluid retention (hepatorenal reflex), thus growing circulating blood volume [9]. The endothelium-derived relaxing factor nitric oxide additionally performs a task in modulating the hepatic microcirculation in both well being and disease. Clinically, ischemic hepatopathy is characterised by a marked and fast elevation of serum aminotransferases inside forty eight hours of the initial insult. Although some definitions require serum aminotransferases of a minimal of 20 occasions the higher limit of regular, ischemic hepatopathy has been histologically confirmed in sufferers with enzyme ranges nicely below this limit [11]. Serum levels of creatinine, lactate, and lactate dehydrogenase are sometimes elevated. The course of hypoxic liver injury is self-limited if the underlying circulatory disturbance is corrected. Serum concentrations could be anticipated to decrease by at least 50% inside seventy two hours of the insult and return to normal within eleven days if perfusion and oxygenation are restored and urine output is regular [12]. The histology in hypoxic liver injury is marked by centrilobular necrosis with preservation of the periportal zone. Prognosis of hypoxic liver injury is dependent upon the underlying illness and therapy must be directed towards restoring sufficient blood circulate and oxygenation whereas addressing the underlying cause of hemodynamic instability. Patients with chronic liver congestion are notably susceptible to hypoxic liver damage when perfusion is compromised. Many stories document the traditional clinical and histologic image of hypoxic liver harm in patients with continual congestive coronary heart illness and an acute event leading to decreased perfusion, sometimes without an obvious or significant lower in systolic blood stress [11]. This elevated propensity is probably going the results of a combination of insults: decreased cardiac output, which may result in continual recurrent subclinical hypoxic occasions; splanchnic vasoconstriction from activation of the reninΡngiotensin system, which can additional decrease hepatic arterial blood circulate; increased sinusoidal strain; and endotoxemia promoted by ischemic and/or congested bowel [11]. In addition to facilitating the event of classical hypoxic liver damage with markedly elevated serum aminotransferases and centrilobular necrosis, continual hepatic congestion is itself related to a distinct liver lesion marked by a spectrum of fibrotic adjustments ranging from delicate sinusoidal fibrosis to the looks of broad fibrous septa to frank cirrhosis (cardiac cirrhosis) [13]. Although most regularly described in affiliation with right-sided heart failure, this lesion can even complicate ischemic coronary heart illness, restrictive lung illness, constrictive pericarditis, pericardial effusion, and another entity resulting in elevated central venous stress. In a study of over 1000 adults with heart failure, cholestatic markers correlated with indices of right-sided coronary heart failure, and serum gamma-glutamyltransferase and alkaline phosphatase levels predicted death or coronary heart transplantation, suggesting that these could serve as biomarkers of coronary heart failure in related populations [14]. In children, the most common causes of coronary heart failure are prone to be congenital heart diseases. Among these, anomalies similar to pulmonary atresia, ventricular septal defect, and transposition of the nice arteries might lead to pulmonary hypertension and chronic passive liver congestion. In addition, as new approaches for surgical and medical management of congenital coronary heart lesions have increased the long-term survival of infants with important complicated coronary heart illness, the long-term impact of those therapies is changing into obvious. One instance is the presence of liver disease in patients with the Fontan circulation. This palliative procedure, used in sufferers with single ventricle physiology, re-establishes normal systemic oxygen saturation by immediately routing systemic venous return to the pulmonary arterial system. Acute dysfunction, usually around the surgery itself, represents basic hypoxic liver injury associated to hypoperfusion, while long-term liver dysfunction might reflect a mixture of continual passive congestion and decreased cardiac index [15]. Hepatic venous outflow obstruction Effective obstruction of hepatic venous outflow can happen at several levels. The commonest causes of inherited thrombophilia related to Buddhiari syndrome are the acquire of operate mutations in factor V Leiden (leading to activated protein C resistance) and prothrombin (leading to excessive prothrombin generation), and loss of anticoagulant operate via protein C, protein S, or antithrombin deficiencies [19]. The reported prevalence of a number of of those inherited defects in sufferers with Buddhiari syndrome is variable, and sometimes both inherited and bought risk factors coexist. In addition, serum ranges of protein C, protein S, and antithrombin can be difficult to interpret in patients with existing thrombosis, as acquired deficiencies, related to the thrombosis or secondary results, are frequent. However, like deficiencies of the pure anticoagulants, homocysteine level in sufferers with existing thrombosis and secondary liver disease can be onerous to interpret [19]. Theoretically, antifibrinolytic issues may additionally potentiate the development of Buddhiari syndrome. Although rare, thrombocythemia, polycythemia, and thrombocytosis may all happen in children and could additionally be related to a threat for venous thrombosis. Other acquired threat components for Buddhiari syndrome embrace the presence of anti-phospholipid and anti-cardiolipin antibodies, typically related to rheumatologic situations; other persistent inflammatory states such as Beh覴 disease, pregnancy, and the peripartum period; and use of oral contraceptives. Each of these components, genetic and/or acquired, is unlikely to lead to Buddhiari syndrome individually. In many instances, multiple thrombophilic risk elements have been recognized in a share of sufferers, and in those for whom only one danger issue was evident, and as but unidentified predisposition could also be at play. Buddhiari syndrome most often presents as chronic obstruction with hepatomegaly, ascites, belly distension, and belly pain. Often, stomach and chest wall collaterals are distinguished and distended, and serum aminotransferase and bilirubin ranges are solely minimally to reasonably elevated [22]. Unlike adults, youngsters could have only firm hepatomegaly and ascites could also be absent. A liver biopsy may help to outline the chronicity of the obstruction and supply clues relating to the prognosis: cirrhosis and the presence of portal hypertension are related to poor outcomes. Regardless of the site of hepatic outflow obstruction, the tip effect on the liver is identical.
Doppler ultrasound examination of the graft may clearly show impaired flow via the hepatic veins and loss of regular phasicity menstrual cramps 9 weeks pregnant ginette-35 2 mg discount without a prescription, and reversal of circulate in the portal vein often indicates venous outflow issues women's health clinic toronto birth control purchase 2 mg ginette-35 amex. Chronic venous outflow obstruction may be more subtle and current with symptoms of portal hypertension together with ascites menopause pillow ginette-35 2 mg order with visa, esophageal and gastric varices, and decrease physique edema. In the acute phase early after transplantation, outflow obstruction may be very difficult to handle since any attempts at revising the venous anastomosis could additionally be accompanied by heat ischemia of an already damaged graft. Repositioning of an acutely misaligned anastomosis by turning the orientation of the liver might help. Chronic venous outflow obstruction could also be corrected by percutaneous balloon dilatation of a venous stricture. The stricture typically happens cephalad to the anastomosis and may be handled with a stent that bridges the stenosis by going from the vena cava above the liver into the hepatic vein, if the graft has a single vein, or into one of many hepatic veins within the case of a whole liver transplant. A gradient throughout the stenosis should be measured earlier than and after the dilatation to make certain that the dilatation or stenting has had the specified impact. Repeated dilatation over years could additionally be essential to keep strictures from reforming. Chronic venous obstruction might in the end trigger scarring, artificial failure, and necessitate retransplantation. Any affected person with continual venous outflow obstruction or repeated thrombosis deserves a examine of the coagulation system to exclude a hypercoagulable condition. Biliary issues Biliary leaks are predominantly an early postsurgical downside as described in Chapter forty three. Visible bile in peritoneal drains and/or increasing fluid collections near the biliary anastomosis or minimize fringe of the liver in affiliation with rising bilirubin and fever are traditional signs. Cut edge leaks frequently resolve spontaneously until an additional segmental bile duct has been missed within the unique anastomosis. Some surgical teams carry out "again table" cholangiography to avoid missing such ducts. Management of a leak from a significant duct or on the anastomotic website almost all the time requires a surgical strategy. Conservative management with local drainage and broadspectrum antibiotics could additionally be attempted if patients have comorbidities that make re-exploration dangerous. Hepatic outflow obstruction Hepatic outflow obstruction is fortunately the least common of all of the vascular issues that may occur after liver transplantation. This complication has been reported extra generally following technical variant grafts [20]. Symptomatic biliary strictures most frequently occur throughout the first post-transplant yr however can occur even in the second decade after liver transplantation [21]. The incidence of biliary strictures varies throughout studies, but most accept a fee that approaches 30% in technical variant grafts notably when follow-up exceeds 12 months [22]. The indicators and signs of biliary obstruction in the liver transplant recipient can be extremely variable and a lot of patients show solely delicate symptoms. Bilirubin and liver enzymes, together with cholestatic enzymes, may be regular till the patient develops secondary cholangitis or the ducts turn into accomplished occluded by stones. A history of intermittent pale stools and fluctuating serum liver enzymes is very suspicious for this downside. Strictures are categorized as either anastomotic, limited to the area of the biliary enteric anastomosis, or intrahepatic. Anastomotic strictures are often the results of scar formation, local ischemia, or technical points. Intrahepatic strictures are frequently the results of world ischemic damage and have a excessive recurrence price that regularly necessitates retransplantation [23]. Strictures from ischemic cholangiopathy usually presents earlier, 3ͱ2 months following surgery, and are characterised by multiple strictures in second- and third-order ducts. In phase grafts, one phase could have normal-appearing ducts whereas the other, which may have had more compromise in blood move, will exhibit a number of beaded ducts. Stone formation is incessantly seen at narrow areas, and persistent bacterial colonization leading to acute cholangitis is also generally noticed. Intrahepatic strictures have also been associated with immunological harm corresponding to persistent rejection and recurrent or de novo major sclerosing cholangitis. Compromised hepatic arterial circulation should at all times be suspected within the setting of biliary strictures, but strictures can develop even within the setting of normal move within the bigger hepatic arterial branches. When arterial move is insufficient, balloon dilatation and/or surgical intervention are not often profitable and could place the patient at risk for biliary perforation and resulting intra-abdominal infection. Since nearly all of biliary anastomoses in pediatric liver transplantation are nonetheless carried out by building of a Roux-en-Y, the option of endoscopic analysis and therapy is restricted. In the setting of excessive medical suspicion, a percutaneous cholangiogram ought to be obtained, even when radiographic research are adverse. Chronic graft hepatitis/de novo autoimmune hepatitis It has been increasingly acknowledged that liver transplantation recipients can develop a pattern of chronic hepatitis, unrelated to chronic viral infection or typical options of rejection, that may result in vital graft damage. Single-center experiences with protocol liver biopsies in long-term follow-up have revealed that the majority of pediatric recipients develop fibrosis over time, in lots of circumstances associated with chronic inflammatory modifications. Despite any pretransplant proof of autoimmune disease, many patients with these chronic inflammatory adjustments have optimistic autoantibodies just like these present in sufferers with a major prognosis of autoimmune hepatitis, and so have been described as having "de novo" autoimmune hepatitis. There is common disagreement as to whether this form of continual graft hepatitis has related pathogenesis to primary autoimmune hepatitis, but all agree that left untreated these changes can result in important irreversible graft damage. The prevalence of this drawback appears to be approximately 5ͱ0% in pediatric liver transplant recipients [25], and differing prevalence throughout research depends upon the strategy of case ascertainment. Many sufferers present with elevated serum liver enzymes detected on the time of routine screening. Liver biopsies performed for clinical causes reveal a sample of interface hepatitis and variable levels of fibrosis. Serum antibodies including anti-nuclear antibodies and anti-smooth muscle antibodies are constructive and serum IgG is regularly elevated. Occasionally, interface hepatitis might be seen on surveillance biopsies within the setting of normal serum liver enzymes. In these cases, elevations of autoantibodies and/ or serum IgG may also be detected. Many descriptions include a regimen of steroids and an antimetabolite corresponding to azathioprine. Investigations of the immunologic phenotype on this disorder counsel that sufferers with this drawback are comparatively overimmunosuppressed and have vital alternations in regulatory T-cell function. Therefore, novel approaches similar to reduction of T-cell immunosuppression coupled with agents corresponding to sirolimus may be successful methods to deal with this injury while nonetheless preventing rejection. Long-term outcomes Patient and graft survival Many bigger pediatric liver transplant programs are reporting 1-year adjusted patient and graft survival rates that exceed 95% and 90%, respectively. Comparing these outcomes by era of transplant reveals that survival statistics have improved slightly over the past 5ͷ years, extra dramatically over the past 10 15 years. Post-transplant complications had been associated with the best relative dangers, with reoperation for any trigger related to an 11-fold enhance in risk for death or graft loss. Technical variant grafts have been independently associated with decrease outcomes, but the hazard ratios were less pronounced when reoperation was added to the model. Outcomes have also been reported to range by major illness, with biliary atresia related to the bottom danger. An evaluation of the causes of patient demise and graft loss in patients that survived the primary post-transplant 12 months implicated infections as the most common trigger for late affected person mortality [28]. In that evaluation, 45% of affected person deaths have been attributed to the aggregated diagnoses of sepsis, multisystem organ failure, and posttransplant lymphoproliferative disease. Recurrent malignancy caused 18% of late deaths and rejection was implicated in only 3%. Conversely, rejection was the most common cause, 49%, of late graft loss in long-term follow-up. Retransplantation Patient and graft survivals after retransplantation are approximately 10% less than following major transplantation. Indications for retransplantation range by interval from transplant, however vascular complications account for a big proportion: 47% at less than 30 days and 26% at >30 days [29].
A advice was made to check novel brokers in homogeneous research populations with clinically defined primary end-points menstruation on full moon 2 mg ginette-35 trusted. In mitochondrial myopathies or cardiomyopathies menopause gift basket cheap 2 mg ginette-35 with visa, occasional patients have shown dramatic improvement in muscle energy and cardiac operate after coenzyme Q supplementation women's health and mental health ginette-35 2 mg generic without prescription. There have now been numerous reports of patients with myopathy and cerebellar ataxia and primary deficiencies of coenzyme Q who responded very nicely to repletion with this substance. There is little reported expertise utilizing coenzyme Q in patients with mitochondrial hepatopathies. Other antioxidants which have been administered to sufferers with respiratory chain defects include menadione (vitamin K3), ascorbic acid, and vitamin E (Table 35. Vitamin E is incorporated into mitochondrial membranes when administered exogenously and is of theoretical but unproven benefit. However, in some sufferers with electron transport complex abnormalities, carnitine has led to elevated liver harm, presumably by way of elevated electron flow and increased technology of oxygen free radicals. Therefore, L -carnitine supplementation in sufferers with mitochondrial hepatopathies must be used fastidiously. Dichloroacetate administration has been proposed to stimulate pyruvate dehydrogenase activity and has occasionally resulted in reduced levels of plasma lactate but has not resulted in a clear change of the natural historical past of respiratory chain problems. These medicine include valproate, barbiturates, salicylates, tetracycline, chloramphenicol, ibuprofen, amiodarone, linezolid, reverse transcriptase inhibitors, and the ingestion of alcohol. Dietary remedy A high-lipid, low-carbohydrate food plan must be instituted in patients with advanced I deficiency [70]. A high-glucose diet is a metabolic problem for patients with an impaired respiratory chain and should have precipitated hepatic failure in patients with Pearson syndrome. Since glucose oxidation is basically aerobic within the liver, the supply of large amounts of dextrose to impaired hepatic mitochondria might end in elevated lactate production and worsening acidosis and ketosis. Based on these concerns, the recommendation is to keep away from a hypercaloric food regimen excessive in carbohydrates and parenteral infusions of options containing excessive concentrations of dextrose. It must be assumed that these patients were fastidiously selected and that these results are perhaps the most effective case state of affairs. This survival rate is much under that expected in pediatric liver transplantation (800%). Gene therapy and cell-based therapy Somatic gene switch remedy is being tested in numerous human genetic disorders, with restricted success thus far. Another uses a self-replicating copy of a normal gene sequence delivered into mitochondria in vitro. Finally, numerous in vitro approaches could be taken to stop recurrence, similar to using donor eggs for future pregnancies. Another chance for the longer term is of nuclear switch from a maternal egg and fertilization in a donor cytoplasm utilizing paternal sperm. Liver transplantation Although the presence of great neuromuscular or cardiac involvement in respiratory chain disorders should preclude using liver transplantation, a selection of patients with defects isolated to the liver have now successfully undergone liver transplantation with excellent long-term outcomes and no extrahepatic disease expression. The prerequisite for considering liver transplantation in this setting is the exclusion of great extrahepatic illness [2,71]. Three of the six sufferers who died developed neurologic options only after liver transplantation. All of the patients who had liver failure and related gastrointestinal illness died shortly after liver transplantation. Currently, prenatal prognosis is beneficial primarily in households affected by a respiratory chain defect brought on by a recognized nuclear-encoded causative gene. A comparison of salient features of six of the first mitochondrial hepatopathies is given in Table 35. Diagnosis is shifting to genotyping probably causative genes, as more nuclear genes are recognized, and next-generation sequencing of nuclear and mitochondrial gene panels in the near future. Treatments are presently not satisfactory; nevertheless, liver transplantation could additionally be profitable in chosen sufferers with isolated liver involvement. The subject of mitochondrial drugs is creating rapidly with hope for model new therapies in coming years. Website information Additional info could be obtained from the following Internet websites. The identification of several secondary mitochondrial hepatopathies stresses the crucial nature of mitochondrial perform within the pathogenesis of liver harm and in the mobile processes of necrosis and apoptosis. Do defects in mitochondrial power metabolism underlie the pathology of neurodegenerative diseases? Mitochondrial toxicity of antiepileptic medicine and their tolerability in mitochondrial disorders. A new syndrome of refractory sideroblastic anemia with vacuolization of marrow precursors and exocrine 2. Epidemiology of A3243G, the mutation for mitochondrial encephalomyopathy, lactic acidosis, and strokelike episodes: prevalence of themutation in an grownup inhabitants. Clinical and genetic spectrum of mitochondrial neurogastrointestinal encephalomyopathy. Mitochondrial respiratory chain complicated I deficiency with clinical and biochemical options of long-chain 3-hydroxyacyl-coenzyme A dehydrogenase deficiency. Generation of hydroperoxides in isolated rat hepatocytes and hepatic mitochondria uncovered to hydrophobic bile acids. Clinical shows and laboratory investigations in respiratory chain deficiency. Comprehensive one-step molecular analyses of mitochondrial genome by massively parallel sequencing. Therapy for mitochondrial issues: little proof, excessive analysis exercise, some promise. Dealing with uncertainties: ethics of prenatal analysis and preimplantation genetic prognosis to stop mitochondrial disorders. It can be present in lean people but typically they too have important visceral adiposity or severe insulin resistance syndromes, such as lipodystrophy [3]. There was an general prevalence of 13% for fatty liver, outlined as 5% of hepatocytes containing macrovesicular fat, with the best prevalence (17. Similarly, a disproportionately higher proportion of Hispanic (45%) and white adults (33%) were affected than black adults (24%), although the prevalence of irregular steatosis in black individuals was a lot larger than that discovered within the pediatric examine (1. As a consequence, many laboratory ranges for irregular are set excessive and may miss clinically vital liver illness. Higher estimates, roughly 40͵0% prevalence, were discovered utilizing ultrasonographic evidence of fatty liver as the screening technique. Elevated fasting triglyceride and glucose levels, waist circumference, hypertension, and obesity are thought-about parts of the metabolic syndrome. Several small case sequence in youngsters document that fibrosis progression can happen even during childhood, with progression to cirrhosis occurring in as brief a time span as 2 years in some instances [23,24]. In adult sequence, potential clinical predictors of development embody extra pronounced insulin resistance, progressive weight gain, age, and irritation. Prognostic indicators in childhood stay unknown due to the small pattern measurement of reported circumstances. Liver disease was the third leading reason for death, occurring in 13% of those who died, compared with the 13th main cause within the basic inhabitants. The two leading causes of demise were malignancy and ischemic heart disease (28% and 25% of the deceased, respectively). The three commonest causes of dying had been coronary artery illness, malignancy, and liver-related dying. The elevated presence of these preclinical markers of atherosclerosis means that these youngsters are likely to face excessive charges of cardiovascular events in the future, in accordance with grownup data. Parallel lipidomic analysis of murine and human liver tissues decided that mice maintained on a high-fat or high-fat high-carbohydrate food plan provide a reproducible model of progressive liver illness. Further, this ongoing mitochondrial damage may be associated with reactive oxygen species launch and progression of disease to extra extreme types [34]. As mentioned above, there are genetic components that can predispose an individual or particular ethnic group to worsening insults from related or fewer dietary mal-influences. A nutritional constituent that has obtained a lot attention and analysis is fructose.
The pharmaceutical kind is D -penicillamine (referrred to as D-penicillamine or penicillamine) menopause fatigue ginette-35 2 mg discount free shipping, as L -penicillamine is poisonous 9gag menstrual cycle ginette-35 2 mg generic on line. The main motion of penicillamine was originally thought to be a "decoppering impact menopause irregular bleeding 2 mg ginette-35 discount visa," though there are conflicting knowledge as to whether it really reduces complete copper content of the liver and other organs. Alternatively, a "detoxing" effect has been proposed in which copper is instantly complexed to the drug and induction of metallothionein synthesis occurs. It is recommended to start penicillamine therapy with 250͵00 mg/day and increase by 250 mg increments each four 7 days to a most dose of 1000ͱ500 mg/day in two to 4 divided doses in an adult, given ideally at least half-hour earlier than or 2 or extra hours after meals as food inhibits its absorption [1]. In youngsters, the goal dose is 20 mg/kg every day, rounded to the nearest a quantity of of 250 mg and given ideally in three divided doses. After stabilization, the dose can be divided into two or three every day doses not to be given with meals. Penicillamine may have an antipyroxidine effect; therefore, all handled patients should also obtain 25͵0 mg pyridoxine daily [1]. During the primary month of penicillamine remedy, the patient ought to be monitored weekly for fever or rash. A full blood count and platelet count, urinalysis, renal and liver blood tests must be obtained each 1 to 2 weeks. If the affected person responds appropriately with decision of symptoms and normalization of liver blood exams, monitoring is carried out every 1 to 3 months for the primary 12 months, and each 6 to 12 months thereafter. Abnormalities in liver blood exams could persist for a minimum of a 12 months of therapy; however, the pattern ought to be towards improvement within the first 6 months of therapy. An annual 24-hour urinary copper excretion is helpful in monitoring chronic penicillamine remedy. Initially, as much as a quantity of grams of copper could additionally be excreted in 24 hours; nevertheless, after months to years of chelation, as little as 200 to 500 g of copper ought to be excreted per day [1]. If urinary copper excretion is <200 g/24 h, poor adherence with chelation remedy ought to be suspected or overtreatment and excess copper removal. In those with non-adherence, non-ceruloplasmin-bound copper is elevated (>15 g/dL) and in those with overtreatment, values are low (<5 g/dL). If copper excretion increases all of a sudden, this implies a lapse in adherence, adopted by resumption of penicillamine a quantity of days previous to the urine assortment. Noncompliance is suspected if, during chronic therapy, the nonceruloplasmin-bound copper is >20 g/dL. For patients in whom K-F rings had been initially detected, serial ophthalmologic examination is useful in documenting disappearance or significant discount of those lesions with enough copper chelation [1]. Serial ophthalmologic examination may also be useful in sufferers with out K-F rings, as the development of rings would also point out poor compliance. For patients that require larger doses of penicillamine, the dose can be decreased to 750 to a thousand mg/day once scientific symptoms have resolved [1]. If compliant, penicillamine remedy will maintain the asymptomatic affected person in good well being. A yearly dialogue with the affected person and household should reinforce the significance of compliance. Patients should be reminded of the important have to take the penicillamine without fail, and the attainable fatal consequences of discontinuing this therapy all of a sudden. In one series, eight of 11 sufferers who discontinued therapy died of fulminant liver failure inside 2. In 10͵0% of sufferers, neurologic signs worsened shortly after penicillamine remedy was started [19]. Continued or reduced dose penicillamine remedy generally resulted in reversal of this worsening, although irreversible neurologic abnormalities have been reported [19]. Therefore, it is recommended that the penicillamine dose be lowered to 250 mg/day if neurologic signs worsen and gradually elevated each 4ͷ days by 250 mg/day till urinary copper excretion exceeds 2000 g/day. Worsening neurologic operate has additionally been reported, although less regularly, following initiation of therapy with trientine, thiomolybdates, and zinc. A seriously neurologically handicapped affected person might respond poorly to penicillamine remedy alone and require mixed therapy with British AntiLewisite. Recent knowledge suggest that the investigational drug ammonium tetrathiomolybdate could additionally be a greater various in patients with neurologic signs [48] but this drug has not been permitted to be used. The effect of penicillamine therapy on psychiatric disturbances is troublesome to predict, though improved faculty efficiency is usually noticed in treated kids. Liver dysfunction typically improves rapidly (by 2Ͷ months) with penicillamine remedy but if overt fibrosis and cirrhosis are present, the signs of portal hypertension present little response though histology might steadily enhance. Hepatic copper content material generally decreases but might stay fairly elevated regardless of years of remedy and clinical improvement. Patients with psychiatric disturbances require not solely copper chelation remedy but also psychotherapy and appropriate psychotropic medicines. Penicillamine may produce each allergic and poisonous unwanted facet effects in up to 30% of sufferers, which has restricted its use in current times. Early unwanted effects of penicillamine include a hypersensitivity response manifested as fever, skin rash, lymphadenopathy, and pancytopenia [1]. After the first year of remedy, late poisonous reactions embody proteinuria, nephrotic syndrome, drug-associated systemic lupus erythematosus, Goodpasture syndrome, optic neuritis, agranulocytosis, thrombocytopenia, myasthenia gravis, low serum IgA levels, loss of taste, and anaphylactic reactions [32]. The most common late reactions with penicillamine are noticed in the skin because of the interference with cross-linking of collagen and elastin. These embrace a dermatopathy (cutis laxa) associated with weakening of subcutaneous tissue, elastosis perforans serpiginosa, lichen planus, aphthous stomatitis, systemic sclerosis-like lesions, and pemphigoid lesions in mouth, vagina, and skin. For therapy of these reactions, penicillamine ought to be briefly discontinued until the lesions resolve, and a pair of or three days earlier than restarting therapy, 0. Penicillamine might then be reintroduced at a decrease dose and elevated gradually with weaning of prednisone when the ultimate dose is reached and tolerated [32]. Alternatively, trientine remedy should be substituted for penicillamine with any important poisonous response. If bone marrow toxicity is noticed, penicillamine must be instantly withdrawn and trientine substituted. Overall, trientine seems to be associated with a decrease frequency of side effects and is really helpful by some authorities as a safer initial chelator for Wilson illness. Penicillamine therapy is ineffective in sufferers with fulminant Wilson disease (acute liver failure), in sufferers who develop hepatic failure after penicillamine therapy has been discontinued, and those with advanced cirrhosis [32]. As in other patients with acute liver failure, survival depends on fast referral to a liver transplant middle, intensive care therapy, and a fast evaluation for liver transplantation. It could be very efficient and lots of advocate it the preferential first-line copper-chelating drug [49], primarily because of its higher security profile. The initial dosage for adolescents and adults and is 750ͱ500 mg/ day in two to three divided doses 30Ͷ0 minutes prior to meals or 2 hours after meals. In youngsters, the dosage is 20 mg/kg daily rounded off to the closest 250 mg in two or three divided doses. Initiation of therapy requires a medical and laboratory assessment and adjustment of doses in an analogous manner to that for penicillamine. Because up to 50% of patients on this collection who had neurologic disease showed worsening of their signs with penicillamine therapy, they proposed using an alternate drug, ammonium tetrathiomolybdate, for preliminary remedy in neurologically affected sufferers [19,48]. This investigational compound acts by forming a steady three-way complex with protein and copper. This drug might exhibit a better affinity for copper than metallothionein in vitro, providing a rationale for its proposed capability to take away copper from cells. An preliminary research of 33 neurologically affected patients treated for 8 weeks as preliminary therapy reported that there was no worsening of neurological symptoms. The drug was given for a total of eight weeks, as 20 mg with meals and snacks and between-meal dose ranging from 20 to 80 mg, 3 times a day. After eight weeks, the drug was stopped and sufferers had been maintained on oral zinc acetate 50 mg thrice a day. In a follow-up research with 22 further patients, the incidence of unwanted side effects was barely larger. Of the 22 patients, three dropped out of the examine, two developed neurologic deterioration and 5 had bone marrow suppression.
Prunus amygdalus var. dulcis (Sweet Almond). Ginette-35.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96105
In a affected person with a supracondylar fracture women's health center tualatin purchase ginette-35 2 mg mastercard, the quick concern is whether or not there are associated neurovascular accidents pregnancy hormones ginette-35 2 mg purchase amex. Prior to therapy menopause joint aches purchase ginette-35 2 mg with amex, a whole neurocirculatory examination of the forearms and palms is performed to doc pulses, capillary fill, ache, gentle touch, power, and range of movement of the fingers. A detailed motor and sensory examination of the median, anterior interosseus, ulnar, and radial nerves is carried out. A supracondylar fracture can interfere with the circulation to the hand by immediately injuring the brachial artery, kinking the artery, or by inflicting an extreme quantity of swelling in the volar compartment of the forearm (21, 22). After a supracondylar fracture, the compartment that most often develops excessive swelling is the volar compartment of the forearm. A compartment syndrome may be first detected by noticing that the affected person is experiencing ache that appears out of proportion to the bodily findings. Early detection is essential as a outcome of once the pulses are absent, the muscle tissue in the forearm may already be necrotic. When the necrotic muscular tissues develop fibrosis and scarring, a "Volkmann ischemic contracture" develops causing a flexion deformity of the wrist and fingers that can markedly intrude with hand operate. The radial nerve is examined checking the sensation in the dorsal internet space between the thumb and the index finger (sensory), and by asking the patient to prolong his fingers (motor). The median nerve is tested by checking the sensation on the volar facet of the index finger (sensory), and asking the affected person to flex the long and ring fingers (motor). The anterior interosseous nerve has no sensory part, but the motor component can simply be evaluated by having him kind a ring between the thumb and index finger. If the patient is unable to kind a hoop between the thumb and index finger due to weak point of the flexor pollicis longus and the flexor digitorum profundus of the index finger (arrow), it signifies an anterior interosseous nerve palsy. The ulnar nerve is tested by checking the sensation on the volar facet of the little finger (sensory), and asking the patient to spread his fingers apart (motor). The last muscle innervated by the ulnar nerve is the first dorsal interosseous muscle. This muscle may be tested by putting a finger on the radial facet of the distal phalanx and one other finger on the muscle stomach of the primary dorsal interosseous muscle. Most individuals have two-point discrimination of 2 to 4 mm in the index (median nerve sensation) and little fingers (ulnar nerve sensation). To check the motor operate of the anterior interosseous nerve, the clinician holds the index finger with the metacarpophalangeal and proximal interphalangeal joints in extension, and asks the patient to flex the tip of the finger (arrow). Inability to flex the tip of the index finger indicates an anterior interosseous nerve palsy. The first dorsal interosseous muscle is tested by flexing the metacarpophalangeal of the index finger to 60 levels and placing a finger on the radial side of the distal phalanx and another finger on the muscle belly of the first dorsal interosseous muscle. The patient is requested to push the index finger in a radial path, and a contraction of the first dorsal interosseous muscle is palpable (arrow) if motor operate is intact. If the patient is apprehensive and experiencing extreme ache, the bodily examination may be compromised. In this case, a supracondylar fracture of the distal humerus is suspected, so anteroposterior and lateral radiographs of the elbow are really helpful. Since the plenty have been pointed out to him, he has noticed that they get larger and smaller most notably with exercise. He has not had any problems with fatigue, weight reduction, or fevers and has otherwise been doing properly. The clinician understands that although soft-tissue lots in children are common and nearly always benign (23), it is extremely necessary and sometimes troublesome to differentiate between benign and malignant soft-tissue lesions. The most common benign and malignant soft-tissue plenty seen in youngsters are listed in Table 4-5. Unlike bone tumors where the bodily examination and radiographs are equally necessary in developing a differential diagnosis, with soft-tissue tumors the differential prognosis is almost completely reliant on the history and bodily examination. The majority of soft-tissue sarcomas are painless lots till they turn out to be massive enough to impinge upon the neurovascular structures. Intramuscular hemangiomas and synovial cysts can present with a waxing and waning boring ache because of adjustments in blood circulate and dimension throughout exercise and relaxation. Benign fibrous tumors, corresponding to nodular fasciitis, myositis ossificans, and glomus tumors may be very painful. Epitrochlear lymph nodes secondary to Bartonella hensela (cat scratch disease), foreign-body granuloma, and intramuscular inflammatory reactions to immunizations are well-known for producing a complicated scientific and radiologic eventualities. Therefore, palpation of regional lymph nodes for will increase in size is an important a half of the bodily examination in this patient. On physical examination, the size, location, consistency, and mobility of the mass or tumor are key parameters to consider. Masses that are >5 cm in diameter, agency, mounted, and deep to the fascia must be considered sarcomas until confirmed in any other case (24). These findings are essential because mobility of the tumor displays the actual fact the tumor has not invaded the fascia and points to a benign lesion. Benign nerve sheath tumors, corresponding to Schwannomas, come up from the epineurium and might be extensively mobile in a medial to lateral path, but firmly fastened in a cephalad to caudad direction in line with the nerve. Lipomas and hemangiomas are described as doughy in texture and cysts are simply compressible. Ganglion cysts will happen adjacent to or connected to a joint capsule or tendon sheath. Fluid-filled lesions such as a popliteal cyst (Baker cyst) will transilluminate with a penlight or flashlight. To carry out this test on a patient with a Baker cyst, the clinician has the patient lie inclined on the exam desk in a darkened room and lengthen the knee while the clinician places a penlight towards the pores and skin. If the affected person has a Baker cyst, the whole cavity ought to be illuminated by the penlight. Absence of any darkish nonilluminated areas within the lesion helps affirm the prognosis of a pediatric Baker cyst. Masses that enhance in size over time should increase a red flag and warrant consideration for biopsy, whereas plenty that have been present for a protracted time are most likely benign. Two exceptions to this rule include synovial cell and clear cell sarcomas as these malignant tumors are identified to frequently develop slowly. Two other exceptions to this rule include nodular fasciitis and desmoid tumors as these benign tumors are rapidly growing and domestically invasive. Large, firm, deep plenty should raise a red flag requiring further workup and sometimes warrant a biopsy. Magnetic resonance imaging with gadolinium distinction is the imaging examine of choice for the differential diagnosis and treatment of soft-tissue tumors. They are comparatively massive, and each tumors are somewhat mobile and transilluminate with a penlight. These discovering are consistent with bilateral Baker cysts that originate from the joint capsule of the knee and protrude between the medial head of the gastrocnemius and the semimembranosus tendons. Since Baker cysts have a excessive likelihood of spontaneous decision in children, shut remark is recommended. A 10-Year-Old Boy Is Referred for Evaluation of Right Heel Pain That Is Aggravated by Playing Soccer. The household seen that he started complaining of proper heel pain 1 month in the past after enjoying soccer. The pain is worse in the evenings, particularly if he played soccer earlier within the day. The historical past is consistent with calcaneal apophysitis, additionally termed "Sever illness," but the differential prognosis includes tumor, an infection, bone cyst, tarsal coalition, leukemia, Reiter syndrome, and juvenile arthritis. Calcaneal apophysitis is the most typical reason for heel pain within the immature athlete and is extra widespread in boys (25). In 1912, Sever described the situation as an inflammatory damage to the apophysis associated with muscle pressure, but latest investigators attribute the symptoms to overuse and repetitive microtrauma. This patient denies any morning ache or stiffness, as one might see in sufferers with juvenile arthritis. He denies any pain at evening, as may be seen in a patient with a tumor or bone cyst. On bodily examination, the backbone, upper extremities, hips, and knees are within regular limits. Ankle dorsiflexion is examined with the forefoot totally supinated, locking the subtalar and tarsal joints, to avoid masking an Achilles tendon contracture secondary to hypermobility at the subtalar and tarsal joints. Ankle dorsiflexion on the left is to 30 degrees and on the best is just to 20 degrees.
Moderate depth exercise will increase hormones similar to adrenaline breast cancer tattoos pink ribbon ginette-35 2 mg buy lowest price, glucagon womens health questionnaire purchase 2 mg ginette-35, and adrenocorticotropic hormone women's health clinic hamilton new zealand purchase ginette-35 2 mg on line, increasing lipolysis of triglycerides in adipose tissue. Increased energy utilization depletes tissue glucose stores and lowers intracellular malonyl-CoA concentrations. Fatty acid oxidation Circulating free fatty acids or fatty acids released from lipoproteins by lipoprotein lipase are taken up into the cell by way of a selection of cell surface fatty acid transporters. All fatty acids are rapidly esterified to acylCoAs via the transporter itself or by acyl CoA synthetase. This enzyme catalyzes the conversion of a longchain fatty acyl-CoA to a fatty acylcarnitine. Oxidation of medium- and short-chain fatty acids is primarily from the successful oxidation of long-chain fat to shorter chain lengths and/or the oxidation of short-chain fatty acids from colonic fermentation. The dehydration response generates a double bond between the - and the -carbon of the acylCoA and varieties the 2-enoyl-CoA product. The medium/short-chain 3-hydroxyacyl-CoA dehydrogenase is a soluble mitochondrial matrix protein with broad exercise toward C416 fatty acids. The product of this reaction is one molecule of acetyl-CoA and a chain-shortened fatty acid. Mediumand short-chain fatty acids are the substrate for the enzyme short-chain 2,3-enoyl-CoA hydratase (crotonase). Both genes are situated on chromosome 2p23 in a head-to-head configuration with coordinately regulated expression [17]. The long-chain acylCoA hydratase and the long-chain hydroxyacyl-CoA dehydrogenase activity are encoded within the -subunit and the long-chain acyl-CoA ketothialase exercise is encoded in the -subunit. Medium-chain ketoacyl-CoA thiolase the medium-chain ketoacyl-CoA thiolase has additionally been known as mitochondrial 3-oxoacyl-CoA thiolase. There is a few substrate overlap between medium-chain and short-chain 3-ketoacyl-CoA thiolases. The medium-chain thiolase former can cleave C4 into 2 acetyl-CoA molecules in addition to cleave longer fatty ketoacyl-CoA moieties, with highest activity towards C10. It cleaves C4 into two molecules of acetylCoA and is thought to be primarily involved in ketone physique synthesis. Oxidation of odd-chain fatty acids Very small amounts of weird chain fatty acid are present in dairy meals merchandise, are digested and absorbed into circulation, and have to be stored or oxidized [22]. These unique fatty acids are oxidized in the same four-step course of as described above to yield a quantity of acetyl-CoAs and one C3 intermediate: propionyl-CoA. The three-carbon propionyl-CoA product of the betaoxidation of an odd-chain fatty acid is transformed to succinyl-CoA by three specialised enzymes. First, propionyl-CoA is carboxylated to D -methylmalonyl-CoA by propionyl-CoA carboxylase, a biotin-dependent enzyme. D -Methylmalonyl-CoA is then converted to its L isomer, L -methylmalonyl-CoA, by methylmalonyl-CoA epimerase. L -Methylmalonyl-CoA is converted to succinyl-CoA by methylmalonyl-CoA mutase, a vitamin B12-dependent reaction. Ketone bodies are released into circulation and supply an alternate gas for the brain. Unsaturated fatty acids Unsaturated fatty acids such as oleic acid (18:1n-9), linoleic (18:2n-6), and linolenic (C18:3n-3) constitute a vital portion (6%) of the whole energy consumed by humans. These fatty acids bear beta-oxidation as described above until the double bond is reached. The trans-2-enoyl-CoA turns into the substrate for long-chain acyl-CoA hydratase or short-chain enoyl-CoA hydratase relying on the fatty acid chain length and continues by way of the beta-oxidation cycle. When the double bond is positioned between the C2 and C3 atoms, 2,4dienoyl-CoA reductase modifications the bond into the trans-3enoyl-CoA. Enoyl-CoA isomerase rearranges the bond to kind 2-enoyl-CoA and the fatty acid proceeds by way of the normal beta-oxidation process. Carnitine transport defects Carnitine is consumed within the food regimen from meat, fish, and dairy merchandise nevertheless it may additionally be synthesized from lysine and methionine within the liver. The beta-oxidation of unsaturated fatty acids is catabolized by two additional mitochondrial enzymes. An isomerase arranges the cis-3 double bond to a trans-2 double bond, and the next hydration by a hydratase permits the rearranged fatty acid to proceed into the normal beta-oxidation pathway. Muscle depletion of carnitine presents with weakness; cardiac depletion causes cardiomyopathy, and hepatocellular depletion may cause hepatic steatosis or fulminant Reye-like syndrome with hepatic failure, any of which could be precipitated during stress or minor periods of starvation. The severe phenotype is characterized by dilated or hypertrophic cardiomyopathy early in life [9]. The presentation may additionally be characterised by hypoketotic hypoglycemia and hepatic steatosis [27]. A cheap strategy would appear to be to use carnitine supplementation judiciously in those with free carnitine ranges below regular. During acute sickness, there are attribute will increase in plasma long-chain acylcarnitines including C14:zero, C14:1, C16:zero, C16:1, C18:zero, C18:1 and C18:2 acylcarnitine esters but significantly in C14:1 [28]. Rhabdomyolysis and myoglobinuria are sometimes associated to a bout of prolonged train, an sickness with fever or poor oral intake, cold temperatures, or a combination of these components. Creatine phosphokinase can be extraordinarily elevated and rhabdomyolysis/myoglobinuria can cause renal failure requiring hemodialysis. A milder kind presents with lipid myopathy, recurrent rhabdomyolysis, and myoglobinuria in young adults. Patients usually current within the neonatal or infancy interval with severe hypoketotic hypoglycemia; hyperammonemia, in all probability from liver failure; and elevated acylcarnitines related to intercurrent illness [26]. In addition, neurological symptoms such as cerebral stroke have been present in all three patients. The typical acute clinical presentation consists of fasting- or illnessinduced hypoketotic hypoglycemia, often associated with metabolic acidosis and hepatocellular dysfunction [34]. Sudden sudden demise has been reported in the first few days after start nearly completely in breast-fed infants, presumably due to the relative fasting status in nursing infants. A985G point mutation, was recognized resulting in a lysine to glutamic acid substitution at position 304 of the mature protein [36]. This missense mutation was subsequently shown to account for a large majority of the alleles in recognized sufferers, although with newborn screening figuring out affected individuals, the prevalence of this mutation may change [30]. A985G mutation leads to decreased but not absent expression of the mutant protein, activity loss being related to defective protein folding [30]. Adults have usually introduced to the emergency room with acute neurological deterioration, and subsequent ventricular arrhythmias. These patients have been hypoglycemic with lactic acidosis and elevated medium-chain acylcarnitines similar to childhood cases. Children sometimes current with hypoketotic hypoglycemia associated with metabolic acidosis, hepatocellular dysfunction, and sometimes cardiomyopathy. A depletion of power or the poisonous results of the buildup of metabolic merchandise are thought to be causative [33]. Deficits in learning and speech/language communication have been reported in symptomatic individuals prior to new child screening but further research is required to determine the prevalence of these problems in screened and early effectively handled populations [38]. Medium-chain 3-ketoacyl-CoA thiolase There has been a single case of deficiency in medium-chain 3-ketoacyl-CoA thiolase described [42]. The affected person had lactic acidosis, hepatic dysfunction, and hypoglycemia in the first few days of life. He continued to deteriorate with hyperammonemia, myoglobinuria, respiratory, and renal failure, and he died on day thirteen of life. Elevated urine C12-C16 dicarboxcylic natural acids have been detected along with decreased fibroblast octanoate oxidation and decreased medium-chain 3-ketoacylCoA thiolase protein expression. Based on this single case, medium-chain 3-ketoacyl-CoA thiolase deficiency seems to be a extreme and lethal condition, but additional patients might want to be recognized earlier than the phenotype may be described with confidence. G625A) however population studies have discovered that up to 14% of the final population is homozygous or compound heterozygous for these frequent missense mutations [39]. A follow-up research of 14 patients who had been recognized by new child screening or who presented symptomatically reported that most sufferers had other medical and neurodevelopmental traits that might have been liable for the symptoms reported [40]. There is clinical heterogeneity, and generally three teams of patients have been described: those with neonatal onset with congenital abnormalities, these with neonatal onset without abnormalities, and those with a late onset with muscle weak spot and carnitine deficiency. Congenital abnormalities embody dysmorphic facial features, rocker-bottom ft, muscular and belly wall defects, and genital abnormalities. Patients with the neonatal-onset type without congenital abnormalities additionally present with hypotonia, metabolic acidosis, hypoglycemia, tachypnea, hepatomegaly, and may develop an acrid odor or odor of sweaty feet. Patients with the milder, late-onset kind current with episodic vomiting, hypoglycemia, and acidosis.
Patients in whom tradition outcomes are unfavorable menstruation symptoms ginette-35 2 mg buy generic on-line, and in whom the scientific picture warrants it women's health clinic gateshead discount ginette-35 2 mg online, should bear a percutaneous hepatic biopsy women's health big book of yoga pdf download order 2 mg ginette-35, for both tradition and histologic examination. Performed in the presence of regular coagulation parameters, this procedure has been proven to be relatively protected, and, at least in grownup series, may be safely carried out in the presence of ductal dilation. Pathologic alterations embody infiltration of the portal triads, bile ductules, and ductule lumens with neutrophils. Therapy of acute cholangitis contains careful consideration to vital indicators and perfusion standing, offering enough fluid resuscitation and strain help if wanted. The affected person is made nil by mouth; nasogastric suction may be required within the presence of ileus. Toxic patients with evidence of biliary obstruction may require emergency intervention, endoscopic, percutaneous or, less generally, operative. In most different sufferers, intervention should be withheld till after a number of days of antibiotic remedy and discount of fever. Choice of antibiotics is ruled by sensitivities of common organisms, and the achievable serum and biliary antibiotic ranges. Potential choices include intravenous ampicillin and sulbactam, thirdgeneration cephalosporins. Alternatively, a broadspectrum penicillin by-product with good biliary penetration. The prognosis of cholangitis in children has not been clearly delineated, but in a single research of cholangitis after the Kasai process, the mortality rate was approximately 1% [13]. Mortality in adult series is considerably greater, presumably due to the higher incidence of malignant lesions and debilitated patients in these teams. Therefore, aggressive diagnostic and therapeutic efforts seem justified on this population. Perihepatitis First famous by Stajano in 1919, Fitz-Hugh (1934) [19] and Curtis (1930) [20] independently described the syndrome of perihepatitis associated with salpingitis that now bears their names. Generally noted in younger ladies, signs embrace acute-onset, extreme right higher quadrant pain, sometimes with radiation to the shoulder and back. The affected person often has each a history of earlier pelvic inflammatory illness and physical findings suggestive of identical. Laparoscopic (laparotomy) findings early in the midst of perihepatitis embrace "violin string" adhesions between the hepatic capsule and the adjacent belly wall and diaphragm. Later findings consist of hemorrhagic spots and white fibrous plaques on the liver floor. The pathophysiology of perihepatitis associated with salpingitis remains unsure. Postulated mechanisms include ascending infection from the genital tract to the perihepatic area, in addition to spread via the bloodstream. Treatment is thru eradication of the underlying an infection with an applicable antibiotic routine. The liver may be involved in patients with gonococcal bacteremia; approximately 50% may have abnormalities of serum aminotransferase levels [21]. The lumen of the bile duct is crammed with acute inflammatory cells and necrotic particles. Neutrophils lengthen into the bile duct epithelium and surrounding portal tract stroma. Mezlocillin used alone has been prospectively in contrast with an ampicillin/gentamicin routine within the treatment of cholangitis in adults and located to have a better price of treatment in addition to a lower incidence of toxicity [16]. Ciprofloxacin has gained acceptance in the therapy of cholangitis in adults but its use in younger kids continues to be debated. Particularly unwell sufferers might require addition of particular anaerobic coverage, as well as the utilization of different antibiotic combos including piperacillin/tazobactam, ticarcillin/clavulanate, imipenem, or meropenem [17]. These procedures have now been safely carried out in important numbers of children [18]. Subsequent cholangiography could delineate the site of obstruction, allowing definitive remedy to be undertaken endoscopically in choose circumstances. Clinical manifestations may embrace encephalitis, pneumonitis, arthritis, osteomyelitis, and neuroretinitis, amongst many others [22]. While hepatosplenomegaly and anicteric hepatitis had beforehand been reported in affiliation with cat scratch disease, the affiliation with hepatic and splenic abscesses was first noted in 1985 [23]. Affected patients often current with systemic signs including fever, chills, myalgia, malaise, and stomach ache. Differential analysis consists of different causes of hepatic granulomas, together with an infection with a wide range of bacterial, fungal, parasitic, and viral brokers. In addition, neoplasms, hypersensitivity reactions, and sarcoidosis must be thought of. In the absence of widely available tradition techniques for the cat scratch bacilli, exact analysis within the correct clinical state of affairs. Therapy within the immunocompetent host stays problematic but some authorities recommend parenteral antibiotic treatment, usually gentamicin [24], for up to three weeks. Potentially effective oral therapy consists of trimethoprimγulfamethoxazole, rifampin, azithromycin dihydrate, and ciprofloxacin [24]. Typhoid hepatitis Typhoid fever, most frequently caused by Salmonella typhi and Salmonella paratyphi (ser. Approximately 27% of patients have hepatomegaly [25], and 5ͱ0% of sufferers will have medical jaundice. Serum aminotransferases and alkaline phosphatase are mildly abnormal in 50% of instances. A recent collection demonstrated irregular liver chemistries in 36% of sufferers with Salmonella enteritidis enterocolitis [26]. Less-frequently noted have been ballooning degeneration of hepatocytes, steatosis, and hepatic granulomata [27]. Typically, findings have been famous together and could be present in biopsies from patients with out hepatomegaly. Hepatic abnormalities typically resolve with remedy of the underlying infection. Yersinia enterocolitica Yersinia enterocolitica has been implicated within the improvement of hepatic abscesses in the setting of hemochromatosis in adults [33]. Toxic shock syndrome Toxic shock syndrome is described as a complication of tampon use but is a consequence of bacterial an infection generally attributable to staphylococcal and streptococcal species. Hepatic involvement in toxic shock syndrome has been described by several investigators. Cholestasis, as delineated by elevated serum bile acid and bilirubin ranges, has been famous in conjunction with elevated serum aminotransferases. Hepatic abnormalities resolve with adequate anti-infective remedy, generally consisting of a beta-lactamase-resistant antistaphylococcal agent at the facet of clindamycin, which inhibits bacterial protein synthesis [24]. Brucellosis Brucellosis, in people typically attributable to Brucella melitensis, B. Complications could embody abscess formation, meningoencephalitis, pneumonitis, osteomyelitis, nephritis, and endocarditis. Infection is usually acquired by way of contact with contaminated animals or ingestion of contaminated milk products. Approximately 25% of affected kids have hepatosplenomegaly on physical examination [28] and 84% have irregular hepatic enzyme research [29]. Clinical jaundice is relatively infrequent, as is cholecystitis, both calculous or acalculous [30]. Liver biopsy findings embody portal irritation and focal hepatocyte necrosis in 90% of patients [31], whereas non-caseating granuloma formation could also be noted in as a lot as 70% of sufferers, primarily throughout the first one hundred days of illness. In rare circumstances of hepatic abscess secondary to Brucella infection, surgical procedure made be required along with medical remedy. Streptococcal infection Infections with Group A -hemolytic streptococci have long been associated with hepatic dysfunction. Jaundice has been reported as both an early and late complication of scarlet fever; the late-onset component might have mirrored use of serum remedy in the early 1900s [35]. Early-onset jaundice was famous in association with hepatic tenderness and hepatomegaly. Pathologic findings embody focal areas of hepatocyte necrosis, in addition to portal inflammatory infiltrates consisting of polymorphonuclear leukocytes and lymphocytes. The etiology of noticed alterations is unclear but might involve direct infection versus toxin effect. Pneumococcal infections (Streptococcus pneumoniae), together with these manifested as pneumonia, are also associated with a high incidence of hepatic enzyme abnormalities and, much less incessantly, jaundice [37].






