Trileptal
Trileptal
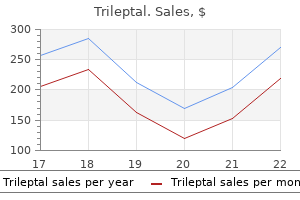
Trileptal dosages: 600 mg, 300 mg, 150 mg
Trileptal packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

However symptoms internal bleeding buy trileptal 300 mg free shipping, one should be cautious decoding immunoreactivity for these markers as a result of entrapped nonneoplastic cells inside a dermatofibroma may specific both of those antigens medications not to take after gastric bypass trileptal 150 mg purchase on line. This distinction is normally easy but could additionally be tough in a small biopsy pattern medications versed purchase trileptal 300 mg on line. Pleomorphic tumor cells are scattered in a lesion with options otherwise typical of dermatofibroma. A nested somewhat than storiform progress sample and extra oval or rounded nuclei with occasional intranuclear inclusions typical of melanocytes are useful in this distinction. Blue nevi even have extra uniform cytologic options in contrast with dermatofibromas. An immunostain for S100 protein or Melan-A would readily distinguish a melanocytic proliferation from a dermatofibroma. The tumor cells in der- Atypical fibrous histiocytoma (dermatofibroma with monster cells) must be distinguished from atypical fibroxanthoma, pleomorphic fibroma, and an undifferentiated pleomorphic sarcoma of the skin. Age may be useful as a end result of atypical fibroxanthoma and pleomorphic sarcoma more often come up in older adults, usually on sun-damaged skin of the head and neck. Histologically, as with other variants of dermatofibroma, key to the analysis is recognizing the conventional development sample of more typical dermatofibroma with characteristic collagen trapping. Pleomorphic fibroma may be distinguished from atypical fibrous histiocytoma by its far lower cellularity and absence of dermatofibromalike areas and foam cells. Pleomorphic fibroma, atypical fibroxanthoma, and undifferentiated pleomorphic sarcoma sometimes extend to the overlying dermis and lack the "grenz zone. The tumor is often restricted to the reticular dermis however might show limited involvement of the subcutis in a manner just like dermatofibromas. The individual tumor cells have elongated vesicular nuclei and faintly eosinophilic cytoplasm. The fibroblasts in scars are normally aligned parallel to the skin floor and lack the everyday collagen trapping seen with dermatofibroma. The vasculature of a dermatofibroma is typically skinny, branching, and evenly distributed in contrast to the irregular, reactive vessels arranged perpendicular to the dermis in a scar. However, for the mobile and atypical variants, conservative complete excision is price contemplating given their propensity for local recurrence (the local recurrence fee of those variants is 20%) and less favorable cosmetic outcome after continued development and local recurrence. Very uncommon cases of visceral metastases from fibrous histiocytoma have been reported, however metastatic lesions appear to behave in an indolent style and maintain the histologic look of the unique tumor. Dermal scars could be confused with dermatomyofibroma due to the parallel association of spindled cells. Bland myofibroblasts arranged in fascicles, which run parallel to the overlying epidermis. Superficial fibromatosis (Dupuytren contracture) shows significant cytologic overlap with dermatomyofibroma, but the scientific setting (involvement of tendons on the palmar surfaces of arms and feet) is quite distinct. Desmoid-type fibromatosis may present appreciable overlap with dermatomyofibroma histologically, nevertheless it often presents as a larger, deeply situated, and extra infiltrative lesion. Finally, the differential diagnosis from a fibroblastic connective tissue nevus (discussed within the following) could additionally be tough. Histologically, fibroblastic connective tissue nevus consists of haphazardly organized bundles of bland spindle cells involving the dermis and subcutaneous tissue in contrast to extra orderly arrangement of spindle cells in dermatomyofibroma. Excision could also be essential for definitive prognosis when only a small portion of the tumor has been sampled for histology. A, Dermal-based proliferation of bland fibroblasts with overlying epidermal papillary hyperplasia. B, the cells arranged in haphazard fascicles, which entrap cutaneous appendages and may extend into subcutis. The age vary at presentation is broad, though the lesion seems to be most typical in youngsters (median, 10 years). The lesion presents as a solitary, slowly growing agency plaque-like or nodular skin lesion, up to 2 cm in dimension, most frequently on the trunk, but the extremities and head and neck space may be involved. Another distinctive feature of fibroblastic connective tissue nevus is the presence of adipose tissue very superficially within the reticular dermis. Cytologically, the cells show features of bland fibroblasts or myofibroblasts with oval tapering nuclei and pale amphophilic cytoplasm. Dermatomyofibroma (discussed earlier) similarly presents as a fascicular dermal-based lesion. However, it sometimes presents in an older age group, and the fascicles of spindle cells are inclined to run distinctly parallel to the dermis in distinction to the more haphazard appearance of the fibroblastic connective tissue nevus. Histologically, pilar leiomyoma is more nodular in look, and the spindle cells present the features of easy muscle differentiation: elongated nuclei with blunt ends and brightly eosinophilic fibrillary cytoplasm. Superficial fibromatosis may resemble fibroblastic connective tissue nevus histologically however happens in a distinctly totally different medical setting (involvement of tendons on the palmar surfaces of the palms and feet). The stroma is often densely collagenous, however myxoid change may be seen and barely is a prominent feature. Scattered hyperchromatic, typically multinucleated tumor cells are present in a collagenous background. In the autosomal dominant neurocutaneous syndrome (tuberous sclerosis), angiofibromas (adenoma sebaceum) usually manifest in childhood as multiple small papules or nodules on the central face, particularly the nasolabial fold. Fibrous papules, one other kind of angiofibroma, are solitary acquired lesions of adulthood. Pearly penile papules are another type of angiofibroma that happens in groups on the penis, primarily the coronal margin and sulcus in up to 10% of young adults. They may be a quantity of in tuberous sclerosis however usually present as solitary acquired lesions on the digits, particularly around the nail fold. The stroma in these two tumors tends to be extra myxoid, and the fibroblasts are more slender. Spindle and stellated cells are present in a collagenous stroma with ectatic, thin-walled blood vessels. Acanthotic epidermis surrounds vertically oriented spindle cells within the collagenous stroma. Careful attention to the cellular density and distribution of melanocytes as well as scientific correlation is critical for the proper prognosis. Clear cell fibrous papule could also be confused with a sebaceous neoplasm or even metastatic renal cell carcinoma, however immunohistochemical stains can resolve this concern readily. However, all age ranges may be affected in addition to all kinds of anatomic sites. The major entity in the differential analysis of acral fibrokeratoma is a supernumerary digit, but acral fibrokeratomas lack the vestiges of neural structure seen in supernumerary digits. Fibrous papules of the nostril could at times be related to a slight hyperplasia of intraepidermal melanocytes. It has been instructed that a few of these lesions could characterize regressed nevi (melanocytic angiofibromas). A, Loose proliferation of bland myofibroblasts in a tissue culture-like progress pattern admixed with reactive vessels, extravasated red blood cells, and continual inflammatory cells. B, High-power view showing plump myofibroblasts with oval nuclei, nice chromatin, and small nucleoli. The fascial variant of nodular fasciitis is similar in appearance apart from the pattern of development, extending along fascial planes of the subcutaneous septae and imparting an infiltrative appearance. The vasculature is usually more prominent than in typical circumstances of nodular fasciitis. Intravascular fasciitis exhibits an intravascular myofibroblastic proliferation similar to nodular fasciitis. Multinucleated osteoclast-type large cells are usually extra outstanding in this variant. The spindle cells are usually admixed with scattered lymphocytes, extravasated pink blood cells, and occasional osteoclast-type large cells. Most circumstances present various cellularity and myxoid stroma, which sometimes shows cystic breakdown. Nodular fasciitis is usually negative for desmin, cytokeratin, and S100 protein. Dermatofibromas are typically dermal primarily based, have a more storiform sample of growth with peripheral collagen trapping, and have a extra heterogeneous inhabitants of cells.
Isotretinoin additionally markedly affects keratinization and probably exerts an effect on the cohesiveness of the follicular keratinocytes medications with weight loss side effect trileptal 300 mg buy on-line, thus decreasing microcomedone formation 10 medications that cause memory loss discount trileptal 150 mg fast delivery. Less essential actions include anti-inflammatory results medications 122 generic trileptal 150 mg line, antibacterial effects, and inhibition of microbial enzyme activity. Between 1982 and 1989, the producer received 151 stories of patients who carried their fetuses to term. In 47% there were important congenital malformations, with most being cardiovascular, craniofacial, or central nervous system in nature. Patients who turn out to be pregnant whereas taking the drug ought to think about the desirability of constant the pregnancy. Relative contraindications for oral retinoid therapy embrace sufferers with pseudotumor cerebri, inflammatory bowel disease, hyperlipidemia, hepatitis, and these that are youngsters. Patients should initially have complete counseling about the potential unwanted effects of this drug. At a minimum, all patients should have pretreatment blood lipid and liver operate research. An preliminary pregnancy take a look at is required to enter the iPledge program, adopted by a second being pregnant check at an accredited laboratory earlier than actually receiving the drug. Women of childbearing age should begin therapy on the second or third day of their subsequent normal menstrual period after having had a negative serum being pregnant test. If important acne remains to be current after a 2-month period, a second course of isotretinoin remedy could additionally be considered. More than 50 totally different acute and persistent adverse reactions of oral retinoid remedy have been documented in the literature (Table 55-4). More than 90% of patients receiving oral isotretinoin at therapeutic levels reveal cheilitis or xerosis to some extent. There are quite a few current lawsuits and pending litigation concerning this alleged and controversial affiliation. The most typical adjunctive remedy is lip balm for the lips and moisturizers for the pores and skin. While each medicine are orally administered retinoids, they usually have many of the identical therapeutic effects, they also reveal important differences. They appear to be of equal efficacy in disorders of keratinization, such because the ichthyoses and pityriasis rubra pilaris, although good comparative research are lacking. Like isotretinoin, acitretin has been utilized in many different cutaneous illnesses (Table 55-5). Dogra S, Yadav S: Acetretin in psoriasis: an evolving scenario, Int J Dermatol fifty three:525�538, 2014. The therapeutic response of pustular psoriasis, pustular eruptions of the palms and soles, and subcorneal pustular dermatosis means that this drug also modifies neutrophil operate. After applicable counseling and laboratory exams (liver operate checks, serum lipid checks, pregnancy tests), oral acitretin is initially taken with food twice per day in a dosage vary of 25 to 50 mg/day. Studies have shown that larger doses are only marginally simpler, but the dose-related unwanted effects are much more frequent and severe. After the preliminary response to remedy, which often takes eight to sixteen weeks, the upkeep dose can typically be lowered to 25 mg/day or every different day. The physiologic results of vitamin A and retinoids are broad, however crucial features include tissue differentiation (especially epithelial tissues), general progress, visual function, and copy. The contraindications are the same as for oral isotretinoin (previously discussed). As for isotretinoin, acitretin is a being pregnant class X drug and is absolutely contraindicated in pregnant sufferers. In distinction to isotretinoin, which has a terminal elimination half-life of 10 to 20 hours, acitretin has a longer half-life of 2 to four days. Women of childbearing age ought to begin effective contraception for a minimal of 1 month earlier than beginning therapy and continue for no much less than 3 years after discontinuation of therapy. While oral bexarotene administration shares some potential opposed effects with isotretinoin and acitretin. Close monitoring of free thyroxine (T4) levels is important throughout therapy, and sufferers typically require thyroid hormone supplementation. Women of childbearing age will have to have a unfavorable being pregnant test within 7 days of starting bexarotene therapy and should use two dependable types of birth control during and for 30 days after remedy ends. They may be generalized or disseminated or happen within the perianal area in a breech-delivered baby. They may current as aplasia cutis congenita�like pores and skin findings with atrophic areas and scarring. About 70% of infected infants show lesions shortly after delivery, with disseminated disease occurring during the first 2 weeks of life. Viral culture is essentially the most correct means of analysis, but can take a quantity of days to be processed. Intrauterine an infection with varicella-zoster virus that occurs between weeks thirteen and 20 could end in fetal varicella syndrome. These infants are born with chorioretinitis, hypoplasia, and/or paresis of the extremities. Cutaneous findings seem scarlike and happen in a dermatomal distribution with underlying tissue atrophy. The age of onset of varicella lesions is often inside the first 5 to 10 days of life. Neonatal varicella is deadly in about 30% of sufferers whose mothers developed lesions from 5 days before to 2 days after supply. Early identification of an infection and initiation of therapy are crucial aspects of remedy. Ophthalmologic examination could also be needed and enough isolation precautions have to be instituted. The threat is highest if maternal exposure happens through the first 12 weeks of gestation, at which level fetal tissue is quickly dividing. The risk of fetal infection is 90% in the course of the first trimester; nearly all of these infants undergo from congenital defects. Between the 12th and twentieth weeks of gestation, the an infection danger drops to 50%, and about one third of these infants have sequelae. The triad consists of congenital cataracts, deafness, and congenital coronary heart malformations. The syndrome additionally includes microcephaly, microphthalmia, and intrauterine development restriction. These infants represent potential risks to other pregnant ladies, as 5% to 10% of affected infants might shed virus for 12 to 18 months. Human parvovirus B19, the etiologic agent of erythema infectiosum, readily infects erythroblasts and will, subsequently, end in hydrops fetalis and fetal dying. This risk is small, with current research showing a 2% to 9% danger after an infection in the course of the first 16 to 28 weeks of pregnancy. Fortunately, about 50% of pregnant girls have serologic proof of prior publicity to parvovirus B19. Tolfvenstam T, Broliden K: Parvovirus B19 an infection, Semin Fetal Neonatal Med 14:218�221, 2009. The different 5% to 10% often have disease manifested by hepatosplenomegaly, hemorrhagic diatheses, and jaundice. The infant can present with voice modifications or a persistent abnormal hoarse cry as a outcome of laryngeal papillomatosis acquired throughout passage through an infected birth canal. The time between rupture of the amnion and delivery is a important think about vertical transmission price. Tenti P, Zappatore R, Migliora P, et al: Perinatal transmission of human papillomavirus from gravidas with latent infections, Obstet Gynecol 93:475�479, 1999. The combination of cesarean supply and antiretroviral therapeutic compliance can lower this threat to zero. American Academy of Pediatrics, Committee on Infectious Diseases: Herpes simplex, varicella-zoster infections, human immunodeficiency virus, and parvovirus. Both eyes are usually affected, and the corneal clouding could additionally be spotty or diffuse. Eighth nerve deafness normally happens after interstitial keratitis, is usually bilateral, and is usually preceded by tinnitus and vertigo. Bone involvement is widespread with periostitis of long bones, leading to thickened and bent tibias (saber shins) and other bony abnormalities. Syphilitic rhinitis is crucial and frequent physical finding in early congenital syphilis.
Ogungbemi A et al: Computed tomography options of luetic osteitis (otosyphilis) of the temporal bone medications vertigo trileptal 300 mg cheap mastercard. These findings are according to early fibroosseous substitute of regular inner ear fluid symptoms viral infection cheap 150 mg trileptal visa. Demographics � Age Pediatric illness � Epidemiology Meningogenic labyrinthitis is commonest explanation for acquired childhood deafness � Most commonly from Streptococcus pneumoniae or Haemophilus influenzae 6-30% have a point of listening to loss following meningitis 6 medicine bow national forest trileptal 300 mg quality. Note otospongiotic plaques in halo round cochlea, with concurrent fenestral otosclerosis. Concurrent fenestral otosclerosis is noted as bony lucency alongside cochlear promontory extending from fissula ante fenestram. This represents a therapeutic (sclerotic portion) but lively (lucent portion) plaque of fenestral otosclerosis. This predisposes to stapes prosthesis failure and makes cochlear implantation more challenging. Regions of demineralization may be multifocal as in this case or band-like as in earlier case. Basilar impression and craniocervical junction stenosis result in hydrocephalus in this patient, requiring shunting. Note delicate tissue depth changing the traditional perilymphatic tissue of the membranous labyrinth. When these tumors are small, they may be handled conservatively unless the patient has intractable vertigo or the tumor shows signs of interval development. Natural History & Prognosis � � � � � Very slow-growing, benign tumor of membranous labyrinth History of progressive listening to loss could date again 20 years Often grows to fill inside ear, then stops growing Total deafness in ear will outcome finally if untreated Deafness sure if tumor eliminated 7. The slight distinction in enhancement traits is related to volume averaging. Important options embody its vascular nature, tendency to fistulize in inside ear, & bone fragments within tumor matrix. Note diffuse irregular signal in left globe indicating retinal angioma with detachment seen in von Hippel-Lindau illness. Kaya S et al: Effects of intralabyrinthine hemorrhage on the cochlear parts: a human temporal bone study. Klopp-Dutote N et al: A radiologic and anatomic study of the superior semicircular canal. The wire enters the round window and traverses the basal turn of the cochlea to reach the cochlear 2nd flip. The wire enters the round window on its approach to the basal flip of the cochlea, extending well into the cochlear 2nd flip. The regular beaded look from electrodes on the distal cochlear implant wire is properly appreciated on this picture. This "empty cochlea" signifies an irregular extracochlear location of the cochlear implant wire. Note severe obliterative labyrinthine ossificans with bone replacing the basal turn of the cochlea, likely responsible for problem inserting the cochlear implant on this case. Malfunction of cochlear implant is secondary to break in mastoid portion of stimulator wire. Natural History & Prognosis � Very slow-growing lesion � Complete surgical elimination arrests symptom development Treatment � Surgical approaches Removal through transpetrous strategy Middle fossa approach also used 11. The congenital cholesteatoma remodels bone into the world of the medial petrous apex. Notice that trapped fluid in the petrous apex has no related growth or trabecular breakdown. Also notice the absence of fluid opacification of the middle ear and mastoid air cells. The differential diagnosis is congenital cholesteatoma, ldl cholesterol granuloma, and mucocele. T1 sign was low (not a cholesterol granuloma) and there was no restricted diffusion (not a congenital cholesteatoma). The mastoid fluid is intermediate signal, most probably as a result of protein in the fluid. Cortical irregularity of petrous carotid canal raises suspicion of unfold into canal. The presumptive imaging diagnosis of superinfection of trapped fluid was made, & signs responded to antibiotics. Shapiro M et al: Toward an endovascular inside carotid artery classification system. With 3T imaging, more normal enhancement of constructions inside the temporal bone is seen. Dehkharghani S et al: Redefining normal facial nerve enhancement: wholesome topic comparability of typical enhancement patterns-unenhanced and contrast-enhanced spin-echo versus 3D inversion recovery-prepared quick spoiled gradient-echo imaging. Facial nerve prolapse can create important surgical difficulties throughout stapedectomy. Remember that the geniculate ganglion and posterior genu/upper mastoid segment of the facial nerve could normally enhance. Swelling of the facial nerve is feasible outdoors the bony facial nerve canal within the temporal bone. A whole of 8 factors can be obtained if each the eyebrow and the oral commissure both transfer 1 cm. This could be defined by the reality that the geniculate ganglion, together with the posterior genu/upper mastoid facial nerve, may normally enhance. Yue Y et al: Retrospective case collection of the imaging findings of facial nerve hemangioma. B�ck L et al: Management of facial nerve schwannoma: a single establishment experience. Liu R et al: Facial nerve schwannoma: surgical excision versus conservative administration. The intervening tympanic section (not shown) appeared normal, hence the time period skip lesion. Brainard L et al: Association of benign intracranial hypertension and spontaneous encephalocele with cerebrospinal fluid leak. Note the labyrinthine phase of the facial nerve canal is visible, but the lesion includes the geniculate fossa. Multiple different foci are obvious, together with the best occipital bone, clivus, sphenoid bone, and frontal bone. Yang H et al: Surgical treatment of monostotic fibrous dysplasia of the temporal bone: a retrospective evaluation. Notice the thickened ligament linked to the malleus and the erosion of the otic capsule. The petrous apices are enlarged however demineralized, which indicates that earlier, extra energetic disease is current. The lesions lack the typical aggressive periosteal response of metastatic neuroblastoma. The tumor extends into the middle ear cavity & erodes the anterior wall of the jugular foramen. Smaller metastases are simply missed, secondary to aerated/varied appearance of the T-bone. Wierzbicka M et al: Efficacy of petrosectomy in malignant invasion of the temporal bone. The getting into cochlear nerve fibers pierce the brainstem and bifurcate to form synapses with both the dorsal and the ventral cochlear nuclei. These 2 nuclei are discovered on the lateral floor of the inferior cerebellar peduncle. Their location could be precisely determined by taking a look at highresolution T2 axial images and figuring out the contour of the inferior cerebellar peduncle. The coming into vestibular nerve fibers divide into 4 branches to form synapses with the superior, inferior, medial, and lateral nuclei. The vestibular nuclei are clustered within the inferior cerebellar peduncle just anteromedial to the cochlear nuclei.
In distinction to cutaneous epithelioid angiomatous nodules symptoms of anemia order trileptal 600 mg on line, epithelioid angiosarcoma is an ill-defined symptoms of ms order trileptal 300 mg otc, infiltrative tumor that demonstrates a larger diploma of nuclear atypia and pleomorphism medications given im trileptal 600 mg buy generic on-line. Epithelioid hemangioendothelioma has comparable in appearance epithelioid cells and will have intracytoplasmic lumina, but the tumor cells are sometimes distributed in a cordlike pattern or singly in a distinctive myxoid matrix somewhat than the sheetlike pattern of cutaneous epithelioid angiomatous nodule. Cavernous lymphangiomas manifest congenitally or in infancy as ill-defined doughy lots, normally in the head and neck area. Cystic hygroma is a specialised form of cavernous lymphangioma often associated with Turner syndrome. They are composed of dilated vascular spaces that will prolong into the overlying epidermis. The vessels regularly have papillary projections into the lumen representing valves. The lumina are sometimes crammed with eosinophilic proteinaceous fluid, which typically exhibits scattered erythrocytes. The vascular lumens of both tumors are lined by cytologically bland endothelial cells. The absence of valves and presence of numerous erythrocytes in hemangiomas is beneficial in distinguishing them. It is histologically characterized by an elevated density of small blood vessels within the superficial dermis, with many multinucleated cells embedded in a fibrotic stroma. A circumscribed space concerned by dilated vessels lined by bland endothelial cells and containing intravascular valves. Complex proliferation of vessels lined by bland endothelial cells in the reticular dermis and subcutis. Atypical vascular proliferation within the superficial dermis characterized by ectatic vessels lined by plump, barely hyperchromatic endothelial cells. These entities present a minimum of some nuclear enlargement, atypia, and endothelial multilayering. Clinical correlation and cautious consideration to the cytologic options of the endothelial cells are important. Postradiation angiosarcoma typically presents with a larger, clinically more ill-defined lesion and could additionally be multifocal. Because angiosarcomas present important heterogeneity (areas of high vascular density and atypia might alternate with areas of low vessel density and delicate atypia), sampling errors are an issue. The tumors may be violaceous or have an indistinct scientific appearance that belies its vascular nature. The differential diagnosis should always embrace an adenocarcinoma, which can be very similar on morphologic grounds and in addition expresses cytokeratins; nonetheless, adenocarcinoma is adverse for vascular markers. The nuclear atypia is often gentle, and mitotic figures are rare, though overtly cytologically malignant cases have been described exhibiting nuclear pleomorphism, mitotic activity, and necrosis. They could additionally be associated with Kasabach-Merritt syndrome (consumptive coagulopathy and thrombocytopenia). This association is especially frequent however not exclusive to tumors arising in the retroperitoneum. The tumor may show areas with well-formed capillaries as well as multiple glomeruloid nodules composed of tightly clustered epithelioid endothelial cells and pericytes. Kaposi sarcoma is the primary histologic differential prognosis, however it occurs in a very different medical setting and lacks well-formed capillaries and glomeruloid nodules containing epithelioid endothelial cells. These glomeruloid nodules are also just like these seen in tufted angioma, which is believed by some to symbolize the histologic spectrum with kaposiform hemangioendothelioma. More superficial tumors are generally amenable to excision, however full resection is most likely not attainable in deeply located tumors. Death is uncommon except in deeply located tumors associated with Kasabach-Merritt syndrome. In addition to excision, adjuvant chemotherapy could play a role in administration of this tumor. The retiform hemangioendothelioma is extra widespread in young adults and the Dabska tumor in children, although the age range is wide. The retiform hemangioendothelioma usually includes the dermis and should extend into the subcutaneous tissue. Nodular progress of carefully packed vessels (A) composed of uniform, spindled endothelial cells (B). Irregular lymphatic channels with intraluminal tufts lined by columnar or hobnailing endothelial cells with minimal cytologic atypia. Angiosarcoma would sometimes present an infiltrative growth sample with irregular, anastomosing vascular channels, endothelial multilayering, and a higher degree of nuclear atypia. A, Complex progress of branching blood vessels lined by hobnail endothelial cells paying homage to rete testis at low energy. The Dabska tumor demonstrates dilated lymphatic-like areas within the dermis and subcutis harking again to lymphangioma at low power. Retiform hemangioendothelioma is associated with a excessive risk of native recurrence and lymph node metastasis, but dying secondary to the underlying tumor was not reported. All types of Kaposi sarcoma can current with violaceous patches, plaques, or nodules. Hyaline globules representing degenerating erythrocytes are seen within stable areas of the tumor. Kaposi sarcoma typically has a predominance of fusiform cells, but occasionally its tumor cells might have a small epithelioid appearance. B, Nodular lesions are composed of intently packed, spindled endothelial cells with slitlike vascular spaces. Nuclear atypia and pleomorphism are variable, and necrosis and mitotic figures may be noticed. Spindle cell hemangioma, as discussed earlier, has a much less infiltrative sample of development and demonstrates characteristic ectatic vascular spaces and phleboliths. The presence of epithelioid cytologic options might make it difficult to distinguish a lesion of Kaposi sarcoma from epithelioid hemangioma. Lesions of Kaposi sarcoma may present an angiomatoid sample, leading to potential confusion with an ordinary hemangioma in limited biopsy samples. Opportunistic infections play a large role in the mortality rate on this subset of sufferers. Treatment options rely upon the extent of illness and the scientific course and should embody observation; topical modalities similar to cryotherapy for native management; and radiation, chemotherapy, or both. It usually arises as multiple discrete nodules on the extremities and less generally the trunk in young adults and has a male predilection. B, the tumor is composed of epithelioid to brief spindle cells with ample eosinophilic cytoplasm growing loosely in a fibromyxoid stroma. The differential analysis also consists of spindle cell sarcomas with myogenic differentiation such as leiomyosarcoma or rhabdomyosarcoma, but the immnunophenotype of the lesional cells (expression of keratins and adverse desmin, H-caldesmon and myogenin) argues against these possibilities. Rarely, epithelioid angiosarcoma may enter the differential analysis because both tumors coexpress cytokeratins in addition to the vascular markers. Identification of vasoformative architecture and a much larger diploma of cytologic atypia seen in an epithelioid angiosarcoma help in this distinction. These circumstances have a shorter latency (5 years) than different postradiation sarcomas, and a significant quantity might happen in lower than 5 years, even inside 1 12 months after radiation remedy. Primary cutaneous angiosarcoma occurs on sun-damaged skin of the pinnacle and neck of elderly patients, implying that ultraviolet exposure could additionally be a threat issue for the illness. Lymphedema-associated angiosarcoma can occur within the postmastectomy setting or in other settings of continual lymphatic obstruction (Stewart-Treves syndrome). The cytology of the endothelial cells may range from small hyperchromatic cells to large pleomorphic cells with vesicular nuclei. Epithelioid cells with plentiful cytoplasm may also be present in some circumstances (epithelioid). A, Angiosarcoma with dissecting growth sample of complex interanastomosing vessels lined by atypical endothelial cells. Careful examination often reveals the infiltrative pattern of angiosarcoma and cytologic atypia not seen in hemangiomas. Angiosarcoma with a distinguished epithelioid morphology may be confused with carcinoma, but evidence of vascular lumen formation helps establish the prognosis.
It is necessary to observe that certain populations of patients such as diabetic patients or individuals with peripheral neuropathy have a higher danger of problems from their onychomycosis symptoms celiac disease generic trileptal 150 mg otc, necessitating prompt therapy of their nail illness medications made easy trileptal 150 mg. Additionally symptoms quotes cheap 600 mg trileptal, patients should undergo lab monitoring month-to-month while on these agents as a outcome of the chance of hepatotoxicity. Elewski B, Tavakkol A: Safety and tolerability of oral antifungal brokers within the therapy of fungal nail illness: a proven actuality, Ther Clin Risk Manag 1(4):299�306, 2005. Tinea versicolor (pityriasis versicolor) is a hypopigmented, hyperpigmented, or erythematous macular eruption. The correct taxonomic nomenclature of the lipophilic yeast that produces this infection is debatable. Studies point out Malassezia globosa is the organism most incessantly associated with tinea versicolor, though older references list M. Immunosuppression, systemic corticosteroids, and sweaty or greasy skin may even trigger this illness to flare. In the previous, Malassezia has been advised to induce hypopigmentation by production of dicarboxylic acid. The darkish lesions of tinea versicolor could additionally be due to a variation in the inflammatory response to the an infection. Tinea versicolor is recognized by scraping some of the scale from a lesion and in search of the attribute "macaroni and meatballs" under the microscope. The yeast could be demonstrated by skin biopsies or direct examination of purulent material. The severity of seborrheic dermatitis has been reported to be associated with an increase in Malassezia microflora. Patients normally current with a number of tender boggy papules or plaques on the legs or, much less generally, arms. Piedra refers to adherent deposits on the hair shaft attributable to superficial fungal infections. Black piedra, which is attributable to Piedraia hortae, presents as firm black nodules on the hair shaft. Trichosporon beigelii is the etiologic agent that produces white piedra, which results in the formation of less-adherent white concretions on the hair shaft. Candida albicans is the most typical organism isolated from lesions of candidiasis. The medical presentations differ with the websites involved, period of an infection, and immune standing of the host (Table 30-2). The components that predispose to the development of candidiasis are each endogenous and exogenous. Endogenous elements can embrace immunosuppression, diabetes mellitus, other endocrinopathies, antibiotics, oral contraceptives, Down syndrome, malnutrition, and being pregnant. Wagner D, Sohnle P: Cutaneous defenses in opposition to dermatophytes and yeasts, Clin Microbiol Rev eight:317�335, 1995. Thymoma, myasthenia gravis, myositis, and aplastic anemia have been associated with the development of persistent mucocutaneous candidiasis after the third decade of life. Cutaneous candidiasis showing an erythematous plaque with attribute satellite tv for pc lesions in a body fold space. These medication ought to be used with caution, because the primary effect of azole antifungal drugs on hepatic enzyme metabolism is inhibition. This leads to an elevation of the serum stage of any drug that requires hepatic metabolism by the cytochrome P-450 3A4 enzyme in order to be removed. Asymptomatic dermatophyte carriers in households of youngsters with tinea capitis are a supply of therapy failures. Malassezia globosa is the organism most commonly isolated from lesions of tinea versicolor. When combined with azole antifungal agents, these drugs could cause extreme or life-threatening reactions. Elevated levels of cisapride, astemizole, and terfenadine are related to cardiac arrhythmias, particularly torsades de pointes. The metabolism of lovastatin is markedly decreased and can outcome in rhabdomyolysis. Simvastatin, atorvastatin, and cerivastatin are metabolized by the identical hepatic cytochrome and also ought to be averted. Any drug that raises the gastric pH reduces the absorption of itraconazole and ketoconazole. Rifampin reduces the levels of oral azole and allylamines by induction of hepatic cytochromes. Topical nystatin and amphotericin are both ineffective towards dermatophyte infections. Azole antifungal agents block the cytochrome P-450 enzyme lanosterol 14-demethylase, which depletes ergosterol from cell membranes, whereas allylamine antifungals block ergosterol manufacturing by way of inhibition of squalene epoxidase. Systemic antifungals itraconazole, fluconazole, and ketoconazole all inhibit the cytochrome P-450 3A4 enzyme and thereby slow the metabolism of generally used anticoagulants, hypoglycemic, and antihypertensive medicines. In contrast to the superficial dermatophytes, that are usually confined to dead keratinous tissue, sure mycotic infections have the capacity for deep invasion of the skin or production of pores and skin lesions secondary to systemic infection. They are sometimes acquired through direct inoculation, ingestion, and/or inhalation of spores from soil or different organic matter. In this text, the deep fungal diseases are organized into three classes based mostly on medical presentation (Table 31-1). Subcutaneous mycotic infections are attributable to a heterogeneous group of fungi and are infections of implantation (inoculated immediately into the pores and skin through native trauma). The 4 most necessary infections are sporotrichosis, chromomycosis, phaeohyphomycosis, and mycetoma. As a bunch, these infections involve primarily the pores and skin and subcutaneous tissues and rarely disseminate to produce systemic disease in the immunocompetent host. Examples of ailments attributable to dimorphic fungi embody sporotrichosis, histoplasmosis, blastomycosis, paracoccidioidomycosis, and penicilliosis. This organism is found worldwide, except within the polar areas and is commonest in subtropical and tropical climates. The habitat consists of soil, thorny vegetation (especially roses), hay, sphagnum moss, and animals. Cats might carry Sporothrix on their paws and can cause infection by scratching their homeowners or animal handlers. Occupations vulnerable to cutaneous inoculation embrace farmers, gardeners (especially rose), florists, masonry employees, Christmas tree farmers, veterinarians, and animal handlers (especially cats, rodents, and armadillos). The organisms rarely disseminate hematogenously to the joints, bone, meninges, or eye. Pulmonary disease is often as a outcome of inhalation and usually happens in alcoholics and immunocompromised or debilitated sufferers. In the immunocompetent affected person, fungal elements are only found in about 60% of instances even when particular stains are utilized. Itraconazole (100 to 200 mg/day) for a number of months is the treatment of choice for lymphocutaneous and glued cutaneous sporotrichosis, with successful rate of 90% to one hundred pc. The therapy of alternative for disseminated disease is itraconazole 300 mg twice a day for six months, adopted by 200 mg twice a day for 6 months. Several other diseases may present with a distal ulcer, proximal secondary nodules along the lymphatics, and regional lymphadenopathy. The most necessary include nontuberculous Mycobacterium (Mycobacterium marinum, Mycobacterium kansasii, Mycobacterium fortuitum complex), Nocardia, leishmaniasis, cat scratch disease, and tularemia. A patient with this clinical presentation ought to have tissue biopsies for routine histology and cultures to embrace micro organism, mycobacteria, and fungi. They are gradual rising and can be discovered in the soil, decaying vegetation, rotting wooden, and the forest carpet. There are three broad categories of dematiaceous fungal infections together with chromomycosis, phaeohyphomycosis, and eumycotic mycetoma (Madura foot). Medlar our bodies, additionally known as copper pennies or sclerotic bodies, are diagnostic of chromomycosis, differentiating it from phaeohyphomycosis. Tissue biopsies of phaeohyphomycosis are characterized by lightly pigmented filamentous hyphae. Diagnostic golden-brown, yeastlike fungi (Medlar bodies) within a multinucleated foreign body large cell. Other organisms embrace Phialophora verrucosa, Fonsecaea compactum, Rhinocladiella aquaspersa, and Cladophialophora carrionii.
Small vascular lesions called angiokeratoma corporis diffusum are mostly present in a bathing go properly with distribution space symptoms 7 discount trileptal 300 mg line. Nephrogenic systemic fibrosis is a recently described disease characterised by papules treatment efficacy trileptal 600 mg buy otc, plaques 20 medications that cause memory loss 150 mg trileptal buy, and thickened pores and skin of the trunk and extremities. It is related to impaired renal function and deposition of gadolinium in tissues from gadolinium-based contrast media. It is inherited in an X-linked recessive sample, with almost all patients being male. Heterozygous females are typically asymptomatic, though they often have characteristic corneal opacities. They are sometimes distributed in the "bathing swimsuit space," the realm between the waist and the knees. A skin biopsy may assist in establishing the diagnosis because special stains similar to Sudan black B, scarlet purple, or periodic acid�Schiff might reveal glycolipid deposition within the pores and skin. Electron microscopy is incessantly used to assist establish the prognosis because it demonstrates characteristic cytoplasmic glycolipid deposits (typically, within endothelial cells). In adult life, cardiac ischemia and infarcts, transient ischemic assaults, stroke, and progressive kidney failure may develop. Recently, therapy with enzyme alternative remedy has turn out to be available in Europe (-Gal A) and the United States (agalsidase [Fabrazyme]). A pores and skin biopsy demonstrated amyloid deposited in the dermis and subcutaneous tissue. Vessel involvement could range from small postcapillary venules (leukocytoclastic vasculitis) to medium-sized arterioles (polyarteritis nodosa). If vasculitis is confirmed, further testing to embody blood strain, renal perform tests, urinalysis for proteinuria, hematuria, and pink cell casts, ought to be accomplished to determine if the kidneys are additionally involved. Cutaneous lesions because of amyloid deposits are not often seen in this type of amyloidosis. Clinically, normal pores and skin, abdominal fat, tongue, rectal, and minor salivary gland biopsies have been used to confirm the prognosis, thus avoiding the necessity for more invasive biopsies of internal organs. It presents as thickened or edematous pores and skin that primarily impacts the extremities and trunk. In severe instances, there may be restriction of movement or disabling contracture of the joints. Fibrosis can also involve extracutaneous sites including the sclera (yellow scleral plaques), the heart, lungs, and the skeletal muscle. By power dispersive spectroscopy, particles of gadolinium can be detected within involved tissues. Calciphylaxis is a form of metastatic calcification in patients with continual renal failure characterised by acute, painful, ischemic necrosis of the skin and soft tissues. It might current initially with retiform purpura that progresses to painful, gray, bullous, or gangrenous cutaneous lesions, typically resulting in sepsis and death regardless of medical intervention. In renal failure, impaired excretion of phosphate and impaired manufacturing of 1,25-dihydroxyvitamin D3 are theorized to be initiating occasions. A subsequent set off similar to trauma, inflammation, an infection, medicine, administration of calcium, phosphate binders, enemas with phosphate components, or different triggers then causes acute thrombosis and calcification of small vessels. A skin biopsy that features subcutaneous fats is critical to make the analysis and to rule out other situations corresponding to warfarin necrosis, heparin necrosis, oxalosis, or sepsis. Treatments embrace parathyroidectomy, calcium and phosphorus restriction, bisphosphonates, non-calcium phosphate binders, and sodium thiosulfate may be helpful. Calciphylaxis of the lower stomach in a patient with chronic renal failure demonstrating pores and skin necrosis. In one study of a hundred serial outpatients, a 92% prevalence of skin illness was noted. Other common dermatologic situations include bacterial infections, such as Staphylococcus aureus skin infections. Fungal infections, such as mucocutaneous candidiasis (oropharyngeal and vulvovaginal) and dermatophytosis (tinea pedis, tinea cruris, tinea manuum, and onychomycosis), are also generally encountered. Frequently seen viral infections embrace human papillomavirus infections (condylomata acuminata, frequent and plantar warts), as well as infections with herpes simplex virus, varicella-zoster virus, molluscum contagiosum, and Epstein-Barr virus (oral bushy leukoplakia). They are located primarily over the trunk but additionally are seen on the palms and soles. Less widespread manifestations embody impetigo, ecthyma, furunculosis, cellulitis, abscesses, and botryomycosis. As within the general population, infections with community-acquired methicillin-resistant S. Common areas of involvement embrace the trunk, extremities, face, and oral cavity. Early lesions consist of erythematous macules, patches, or papules which will have a bruiselike halo. They enlarge at completely different charges and have a tendency to be oval or elongated in form, following the traces of skin cleavage. The shade varies from pink to pink, purple, or brown and can simply mimic purpura, hemangiomas, nevi, sarcoidosis, pityriasis rosea, secondary syphilis, lichen planus, basal cell carcinoma, and melanoma. Disfigurement and pain secondary to edema can happen, particularly on the face, genitals, and decrease extremities. Therapy of localized disease could additionally be with intralesional vinblastine, radiotherapy, liquid nitrogen cryotherapy, surgical excision, and topical alitretinoin. Treatment of more extensive disease consists of -interferon in addition to single- or multiple-agent chemotherapy with vinblastine, vincristine, bleomycin, or liposomal doxorubicin. Lues maligna, a uncommon manifestation of secondary syphilis, can happen and consists of pleomorphic skin lesions with pustules, nodules, and ulcers with necrotizing vasculitis. Vertically oriented white plaques with a corrugated appearance are seen on the lateral edge of the tongue. Seronegative secondary syphilis, in addition to exaggerated antibody responses, has been reported. It can occasionally also contain the dorsal and ventral aspects of the tongue, the buccal or labial mucosa, and the soft palate. Histologically, parakeratosis, acanthosis, and ballooning cells (koilocytes) are seen. Pseudomembranous candidiasis appears as whitish, cottage-cheese�like or creamy plaques at any website in the oropharynx. Erythematous candidiasis appears as well-demarcated patches of erythema on the palate or dorsal tongue. Lesions of erythematous candidiasis on the tongue can look clean and depapillated. Angular cheilitis consists of erythema, cracking, and fissuring of the mouth corners. Transverse histologic sections are superior to vertical sections in the diagnosis of this disease. Histopathologic findings embrace a perivascular and perifollicular combined infiltrate with variable numbers of eosinophils and spongiosis of the follicular infundibulum or sebaceous gland with a blended infiltrate. Treatment choices embody potent topical corticosteroids, antihistamines, ultraviolet B phototherapy, itraconazole, oral metronidazole, permethrin cream, and isotretinoin. Ellis E, Scheinfeld N: Eosinophilic pustular folliculitis: a complete review of therapy choices, Am J Clin Dermatol 5:189�197, 2004. Lesions can be large (>1 cm, giant molluscum) or hyperkeratotic; can simulate pores and skin cancers, widespread and genital warts, and keratoacanthomas; and may turn into confluent. Lesions can even involve the follicular epithelium with sparing of the interfollicular epithelium. Molluscum lesions can be related to a localized chronic dermatitis surrounding a centrally situated lesion (molluscum dermatitis). With progressive immune dysfunction, lesions enhance in number and become diffuse. Disseminated cryptococcosis, histoplasmosis, and Penicillium marneffei infection can mimic facial molluscum contagiosum.
The excised tissue and Mohs map is transferred to the Mohs laboratory for processing medications japan 300 mg trileptal buy with mastercard, with cautious attention to preserving tissue orientation treatment resistant anxiety trileptal 300 mg generic mastercard. The surgical defect is bandaged and the affected person awaits margin ends in a waiting space medicine 6 clinic 300 mg trileptal discount with mastercard. The excised tissue is processed within the adjacent Mohs laboratory by a specifically educated histotechnician under the supervision of the Mohs surgeon. First the tissue is subdivided into smaller items as needed, sequentially numbered, and reduce edges are shade coded with dyes for accurate identification. The subdivision, numbering, and inking pattern are rigorously recorded on the Mohs map. To enable examination of the complete peripheral and deep margin, tissue is inverted and the angled pores and skin edge is oriented such that the deep margin and skin edge are aligned in a horizontal airplane. Tissue is sectioned in the horizontal aircraft with frozen sections (5 to 7 �m thick). Subclinical tumor extensions are marked on the Mohs map, corresponding tissue is excised in a subsequent stage, and the whole process is repeated till tumor-free margins are achieved. The Mohs method allows examination of the complete margin (similar to en face sectioning) in distinction to bread-loaf sectioning of traditional excision specimens. Total margin control enhances ability to microscopically track irregular subclinical tumor extension and results in the best potential cure charges for high-risk pores and skin cancers. Mohs surgical procedure maximizes conservation of normal tissue in cosmetically and functionally delicate areas (nose, mouth, eyelid, and ear) and minimizes extent of subsequent reconstructive surgery. Mohs surgery is also value efficient given the outpatient setting, avoiding hospital and working room expenses. Given that the whole surgical margin is evaluated with frozen sections, reconstruction of the defect may be carried out immediately. Indications for remedy include bigger tumors, poorly defined scientific margins, location alongside embryonic fusion planes (nasolabial fold, lip, nose, periocular, periauricular), and aggressive histology similar to infiltrative or morphea basal cell carcinomas. These clinicopathologic features correlate to irregular subclinical tumor extension beyond normal excision margins and better recurrence charges. Other indications for Mohs surgical procedure embody incomplete excision, recurrence, or tumor in a young affected person. Basal cell and squamous cell carcinomas are the most common pores and skin cancers handled with Mohs surgical procedure. Mohs surgery can also be used within the administration of much less common pores and skin cancers with propensity for irregular tumor extension, excessive risk for native recurrence, want for tissue conservation, and poorly defined medical margins. Tumor standards for remedy with Mohs surgical procedure embrace contiguous tumor development, accurate interpretation on frozen sections, and successful remedy with slender excision margins. Mohs surgical procedure has been used for the therapy of dermatofibrosarcoma protuberans, atypical fibroxanthoma, verrucous carcinoma, microcystic adnexal carcinoma, sebaceous carcinoma, and different tumors. Cumulative knowledge from small retrospective collection suggest that excision with Mohs surgery may reduce local recurrence charges in these tumors. Limitations of these studies embody differences in clinical and histologic variables and relatively brief follow-up instances. In these tumors, usually an additional margin is excised (after negative Mohs margins) for processing with permanent sections. However, utilizing the accuracy of assessing margins of melanoma with frozen sections is problematic. Furthermore, an unexpected desmoplastic melanoma is more likely to be missed on frozen than permanent sections. Evaluating histologically delicate atypical melanocytic proliferations on the trailing edge of a lentigo maligna is particularly tough and requires high-quality frozen sections (thin sections with even staining and no tissue folds). Because immunohistochemical stains can facilitate visualization of melanocytes, which allows better judgment of their cellular density and distribution, some have adopted this technique to frozen sections. The most sensitive markers to detect intraepidermal melanocytes on frozen tissue are tyrosinase-related protein 1 and Melan-A/Mart-1. Sending the final Mohs layer for permanent sections can also be an option for high quality assurance of the status of the margins. Because histologic examination of melanocytic lesions by permanent sections is extra dependable than on frozen material, modifications of the Mohs technique have been used to overcome frozen section limitations such as excising and mapping tissue in the Mohs manner but processing with en face paraffin-embedded everlasting sections. Other approaches embrace staged excision with peripheral margins excised with geometric angled borders to facilitate vertical section processing. Preserving the integrity of the Mohs specimen requires meticulous consideration to every step of the complete procedure. Obtaining deeper cuts or re-embedding tissue is usually essential to consider the whole epidermal margin. Other processing pitfalls can embody mislabeled tissue, freezing artifact, or floaters. High-quality Mohs frozen sections could be achieved with appropriate coaching and experience. There are instances in which complete tumor eradication might not all the time be potential with Mohs surgical procedure. V-1) is another situation by which tumors can recur despite reaching unfavorable Mohs margins. This problem mostly occurs in recurrent tumors with the scar tissue from previous remedy obscuring tumor. False-negative Mohs margins can also happen in tumors with potential skip areas similar to superficial basal cell carcinomas. The Mohs surgeon ought to concentrate on potential diagnostic challenges in assessing surgical margins on frozen sections. Knowing the particular histologic characteristic of the tumor enhances the flexibility to establish tumor foci. Often tumors can have different histologic subtypes on Mohs excision margins compared with original biopsy histology. Dense inflammatory infiltrates must be examined carefully as a end result of they might be tumor associated or obscuring the tumor. However, in different cases, particularly within the setting of rosacea, perifollicular irritation can be a widespread finding. Differentiating a basal cell carcinoma from a basaloid proliferation or adnexal structure is another potential drawback. Another situation is distinguishing pseudocarcinomatous hyperplasia or tangential sectioning from residual squamous cell carcinoma. For optimum affected person care, it is recommended that debulked tumor tissue of a large invasive carcinoma is distributed for permanent sections to doc the histologic features of the tumor, similar to depth of invasion or the presence or absence of neural or vascular invasion. Lack of such data can become problematic when a patient presents with recurrent or metastatic carcinoma and a history of a quantity of prior pores and skin cancers. If the histologic attributes and stage of the primary tumors are unknown and never discoverable, it can be impossible to judge which, if any, of the cutaneous tumors could be the most probably major tumor. Patients could additionally be subjected to otherwise unnecessary further diagnostic procedures, similar to workup for primary mucosal tumors. The Mohs surgeon might need to seek the advice of a dermatopathologist to help assess margins in uncommon and troublesome tumors. Often an additional margin is shipped for paraffin-embedded everlasting sections in these cases after a adverse Mohs margin to rule out residual disease or for added immunohistochemistry studies. Other points which will require dermatopathology session are assessment of perineural involvement and unsure frozen section analysis of bizarre proliferative lesions. By reviewing Mohs slides at common intervals, the requirement for proficiency testing for the Mohs laboratory can be satisfied. In addition, review of inauspicious Mohs frozen sections with the dermatopathologist and correlating the findings on frozen sections with those on permanent sections can serve to enhance high quality of take care of patients and serve as ongoing peer review for the Mohs surgeon and ongoing learning course of. Difficult frozen sections are best reviewed and discussed on the microscope in the Mohs laboratory. However, telepathology has also been successfully used to facilitate case discussions between surgeon and dermatopathologist. The historical past and evolution of Mohs micrographic surgical procedure, Dermatol Surg 26:303�307, 2000. Clinical worth of paraffin sections in association with Mohs micrographic surgical procedure for nonmelanoma skin cancers, Dermatol Surg 10:1631�1638, 2012. Interpretation of Mohs micrographic frozen sections: a peer evaluate comparability research, J Am Acad Dermatol 20:670�674, 1989. Mohs micrographic surgical procedure for the treatment of spindle cell tumors of the pores and skin, J Am Acad Dermatol 44:656�659, 2001. Melanoma of the lentigo maligna subtype: diagnostic challenges and current remedy paradigms, Plast Reconstr Surg 129:288e�299e, 2012.
The floor of the plaques has a mammillated (nipple-like) appearance and often reveals papulovesicles and pustules medicine search trileptal 150 mg discount otc. A handful of instances have been reported with antineutrophilic cytoplasmic antibodies medications hyperthyroidism generic trileptal 600 mg. Acanthosis nigricans with hyperpigmented velvety pores and skin lesions and small tags on the proximal thigh and groin medications quizzes for nurses trileptal 150 mg purchase visa. The mostly related malignancy is acute myelogenous leukemia, but persistent myelogenous leukemia, lymphocytic leukemia, T- and B-cell lymphomas, polycythemia, and, not often, stable tumors also have been reported. Patients with persistent laboratory abnormalities, particularly anemia, thrombocytosis, and thrombocytopenia, require shut observation and thorough diagnostic analysis. A small subset could have monoclonal IgA gammopathy and other hematologic issues. Leukemia is the most incessantly reported malignancy with myelocytic and myelomonocytic leukemia accounting for the majority of instances. This characteristic skin eruption is related to an -cell tumor of the pancreas, and most sufferers have elevated glucagon serum ranges (glucagonoma syndrome). Skin biopsy shows necrosis of the upper portion of the dermis and is normally diagnostic. This uncommon skin eruption is characterized by a widespread figurate erythema composed of concentric rings with a wood grain appearance. The erythematous circinate lesions might have a nice scale and transfer up to 1 cm a day. Almost all patients with this distinctive dermatosis have an related malignancy, most commonly carcinoma of the lung. The pores and skin lesions clear inside a couple of weeks after removing of the malignancy and normally recur if the most cancers returns. This syndrome begins with acral violaceous psoriasiform plaques on the ears, nose, hands, and feet, likening to "blue psoriasis. This syndrome is characterised by follicular atrophoderma, early growth of multiple facial basal cell carcinomas, and, in some patients, hypohidrosis. Tender, linear, erythematous cordlike plaques are seen most commonly on the arms, legs, flanks, and stomach. The basic eruption of dermatomyositis is a reddish-purple erythema involving the face, usually the eyelids (heliotrope sign). In addition to the facial rash, lesions on the scalp, neck, upper trunk, and extensor extremities are frequent. The erythema on the arms happens over the knuckles quite than over the phalanges, as is typical of lupus erythematosus. Cuticular telangiectasias may be seen in both lupus erythematosus and dermatomyositis. The skin lesions of dermatomyositis might precede medical or laboratory evidence myositis by weeks, months, or years. The true incidence of malignancy related to dermatomyositis is tough to define. Several large research have reported a frequency of internal malignancy related to adult dermatomyositis from less than 10% to over 30%. The sort of cancer reported to be associated with dermatomyositis parallels the incidence of cancer discovered in the general population, though a slight enhance in ovarian carcinoma has been noted. Patients newly identified with dermatomyositis should have age-appropriate most cancers screening, and female patients ought to be screened for ovarian carcinoma. Foss F: Mycosis fungoides and the S�zary syndrome, Curr Opin Oncol 5:421�428, 2004. Paraneoplastic pemphigus is a superficial blistering skin disease related to malignancy. The clinical picture might resemble pemphigus vulgaris, bullous pemphigoid, or Stevens-Johnson syndrome, with important oral mucous membrane involvement. Skin and oral mucous membrane biopsy specimens reveal epidermal acantholysis, epidermal spongiosis, suprabasilar clefts, basal cell vacuolar modifications, and dyskeratotic keratinocytes. Sharply demarcated space of erythema and scale crust that had been handled as a dermatitis, showing partial destruction of the nipple. Antibodies have been demonstrated towards desmoplakins, proteins in keratinocyte attachment plaques (desmosomes), and a 230-kDa protein within the basement membrane (bullous pemphigoid antigen). Rat bladder is a useful substrate for indirect immunofluorescent examination and exhibits constructive staining with serum from patients with paraneoplastic pemphigus but will be negative with serum from sufferers with traditional pemphigus vulgaris. Cicatricial pemphigoid (mucous membrane pemphigoid) is a subepithelial blistering disorder with distinguished involvement of mucosal surfaces, together with the oral mucosa and conjunctiva, in addition to the skin. Scarring of the conjunctiva can result in symblepharon formation and finally blindness. Patients with anti-laminin 5 autoantibodies have an elevated relative risk for stable organ adenocarcinomas. It begins as a small eczematous patch on the nipple that steadily spreads onto the areola and eventually to the skin of the breast. Sharply demarcated erosive plaque with erythema and milky white "strawberries and cream" surface in inguinal area. Patient with long historical past of flushing and growth of persistent telangiectasias of the face. The cause of this illness is a plasma cell dyscrasia, including however less commonly multiple myeloma. The intracutaneous bleeding, so referred to as "pinch purpura," is due to infiltration of blood vessel partitions with amyloid protein. Other less frequent pores and skin lesions embrace waxy papules and nodules, alopecia, nail dystrophies, scleroderma-like lesions, macroglossia, cutis verticis gyrata, bullous lesions, and dyspigmentation. Less widespread findings embrace bronchospasm, cardiac valvular dysfunction, and pellagra-like skin adjustments (photodistributed dermatitis). It is estimated that 10% of patients with carcinoid tumors will develop this syndrome. Development of this syndrome has prognostic significance, as liver metastases underlie most instances, and thus it signifies metastatic, unresectable illness. Multiple reddish-pink papules on dorsal hands and nail folds with attribute coral beading. Skin biopsy exhibits a diffuse histiocytic cellular infiltrate with massive multinucleate giant cells with ground-glass cytoplasm. Associated malignancy was reported in 28% of the patients in 82 instances reported within the literature. Erythromelalgia is a uncommon skin illness characterized by erythematous, painful, burning of the toes, ankles, and decrease extremities. Paydas S, Zorludemir S, Sahin B: Vasculitis and leukemia, Leuk Lymphoma 40:105�112, 2000. Generalized pruritus with out skin lesions has been reported as a symptom of inner malignancy. The cutaneous hallmark of the syndrome is epidermoid cysts, which frequently appear earlier than puberty, frequently on the extremities. The syndrome can be characterized by osteomas (typically on facial bones), fibrous and desmoid tumors, irregular dentition, lipomas, hypertrophy of retinal pigmented epithelium, and leiomyomas of the gastrointestinal tract. The syndrome is characterised by the early onset of colonic polyposis and has a very high incidence of colon most cancers. These sufferers even have benign tumors of neural, fibrous, vascular, and epithelial origin. Multiple small tumors of facial hair follicles (trichilemmomas) and sclerotic fibromas are pathognomonic of this syndrome. Fibrocystic disease of the breast is common, and 30% of girls will develop breast cancer. Many different associated cancers have been reported, with thyroid cancer being the second most typical malignancy. Brown to blue-black macules (lentigines) are present at birth or early infancy on the lips, oral mucosa, nasal mucosa, palms, soles, dorsal hand surfaces, central face, and elbows. Polyps of the small gut develop in 90% of sufferers; polyps may also happen in the abdomen, colon, and rectum. As the name implies, this syndrome is characterised by the development of a number of flesh-colored papules on the tongue, lips, and, occasionally, other mucosal surfaces early in life. These sufferers have a characteristic appearance with thick prominent lips and a marfanoid habitus.






