Persantine
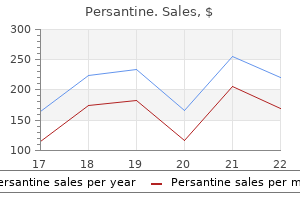
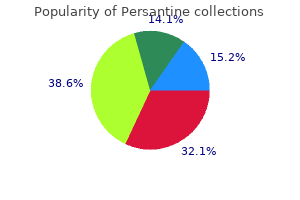
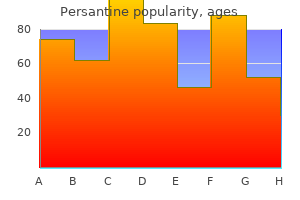
Persantine
Persantine dosages: 100 mg, 25 mg
Persantine packs: 30 pills, 60 pills, 90 pills, 180 pills, 270 pills, 360 pills, 120 pills

A hobnail cell has a slender cytoplasmic stalk at its base and a bulbous apex that harbors a protruding nucleus medications like gabapentin buy persantine 25 mg cheap. Most examples of hobnail cell change have an effect on the endometrial surface and are related to postcurettage regenera� tive atypia medicine 1900s spruce cough balsam fir cheap 25mg persantine fast delivery. The Arias-Stella response is distinguished from hobnail cell change by its usual association with medicine xyzal best 100mg persantine. The medical setting, presentation as a surface*based microscopic discovering quite than an architecturally complicated mass lesion, lack of marked nuclear atypia, absent to inconspicuous mitotic exercise, and absence of stromal invasion assist to distinguish hobnail cell change from pricey cell carcinoma. Atypical hyperplasia is taken into account a most cancers precursor and is often handled with hysterectomy, whereas hyperplasia without atypia is considered sdf-limited and is managed conservatively. Postcurettage regenerative atypia of the epithelium lining the endometrial floor. Simple structure implies outstanding glandular tubule formation with variable levels of cystic dilatation, with outpouches and infoldings being absent, inconspicuous, or focal. In distinction, advanced architecture features abnormal glandular configurations in which branching channels, irregular budding, papillary infoldings, and foci with back-to-hack glands are commonplace. The subjective distinction between easy and sophisticated architectural patterns has not been aided by their various and free definitions. In their seminal article &om 1985, Kurman and colleagues vaguely describe the architecture of straightforward hyperplasia as a rise in the number of glands leading to crowding that ranges from mild to in want of back-to-hack, and glandular shapes that could be altered as a end result of cystic dilatation or delicate irregularities in outline. Just as a villous adenoma with areas of cribriforming is at a much larger threat for the development of colonic adenocarcinoma than the architecturally easy tubular adenoma, endometrial lesions with growing architectural complexity are related to an increasing danger of myoinvasion106. I agree with those that continue to distinguish easy from complex architectural patterns primarily based upon the diploma of contour abnormalities of the constituent glands as described at the beginning of this paragraph, despite the more subjective nature of this approach. Cytologic atypia is acknowledged by variable mixtures of nuclear enlargement, loss of polarity, stratification, rounding, contour irregularities, outstanding nucleoli, and chromatin abnormalities that are most frequently manifested as chromatin clearing. Determinarion of the presence or absence of cytologic atypia is subjective and poorly reproducible, which bas a direct and opposed impression on the power to reliably separate irregular endomet:rial proliferations into the clinically related classes of atypical versus nonatypical bype. I concur with these investigators who emphasize the importance of nuclear atypia re/4tiw to the nuclear features of nonhypcrplastic endometrial glands elsewhere within the speci� males. Artifacts related to fixation and processing can even lead to perceived nuclear abnormalities such as chromatin clearing. Whenever possible, a conscious comparability of the nuclear options of the possibly atypical glandular proliferation must be made to what passes for regular in a given sample, which is in a position to assist to avoid the overdiagnosis of cytologic atypia. This aercise is especially necessary when considering a diagnosis of straightforward atypical bype. In addition to the issues of reproducibly distinguish� ing easy from advanced hype. Bo1h of those examples have been taken from aJthitecturally unremarkable proliferative endometria, and the nuclear features depicted were present throughout the entire glands. Over the course of a long time, pathologists and clinicians have been indoctrinated with the phrases hyperplasia and atypical hyperplasia, and clinip clans an: comfy making treatment selections based upon this classi6cation system. I suspect thar pathologists ha~ problem preserving these terms straight, let alone clinicians. Although this technique has not been validated, it represents a logical amalgamation of what I interpret as probably the most fascinating options of every system. Higbp lights of this hybrid dassi6cation system are outlined under: � As advocated by the Stanford group, a glancJs. For lesions with easy structure, apparent and diffuse atypia is critical earlier than the method is categorized as atypical. To summarize, the diploma of cytologic atypia required for an "atypical� designation is in~rscly propor� tiona! The diploma of atypia that trig� gcrs a malignant diagnosis is depicted in discussions of those entities. When esti� mating this ratio, the area occupied by the gland lumens and villoglandular structures is included in the glandular comparunent. The glands are predominantly tubular, exhibit some cystic dilatation, and are lined by pseudostratified cells wi1hout nuclear atypia. There is ample stroma separating 1he glands, but the glands-to-stoma ratio exceeds 2 to 1. This example consists of intently packed tubular glands of varying caliber that lack cytOlogic atypia and demonstrate a easy rather than complex architectural pattern. The macroglandular items of this hyperplastic proliferation are separated by variable amounts of stroma and contain inside papillary buildings that lack second or third degree branching. This advanced glandular proliferation lacks cytologic atypia and the glands are surrounded by a reasonable amount of stroma. In this lesion, cytOlogic atypia is manifested by nuclear rounding, nuclear enlargement, distinct nucleoli, chromatin clearing, and epithelial stratification. Although the speed of development to carcinoma reported within the 1985 research by Kunnan et al. These information present sturdy help for upgrading the substantial proportion of cases that would historically be considered complicated hyperplasia without atypia to "complicated atypical hyperplasia (based on architecture)� when there are back. Topography of Endometrial Hyperplasia Endometrial hyperplasia may present as a focal. These lesions lack standard options of cytologic atypia and are composed of architecturally advanced, back-to-back glands with threadlike strands of intervening stroma. Although the glands are complex, the mazelike, labyrinthine pattern of adenocarcinoma is absent. A: An island of hyperplasia is present inside a background of proliferative endometrium. B: the hyperplastic focus exhibits some cytOlogic atypia and consists of an admixture of straightforward and complicated architectural patterns with focal morular metaplasia. In addition, the terms focal and di�iUse lack precision and are subjeaively utilized to endometrial lesions. A: this low-magnification view demonstrates a mari<edly thickened endometrium composed of crowded glands with a wide selection of dimensions and shapes. B: Numerous papillary infoldings in these crowded glands creates a pattem of architectural complexity. Foam Cells in Endometrial Hyperplasia Aggregates of stromal foam cells are most often seen within the setting of endometrial hyperplasia or well-differentiated adenocarcinoma. Although originally thought to characterize a modified stromal cell, the constant immunoreactivity of froth cells with the macrophage marker J<P. Hyperplastic glands with cystic dilatation impan a spongy appearance to ponions of the lesion. Whenever attainable, the diagnosis ought to he based mostly upon areas where stromal foam C(:Us arc absent or inconspicuous; if the structure of the entire sample is altered by dusters of froth cells, the repon should embody a cautiorwy note about the potential of underdiagnosis with a advice for shut follow-up with consideration for resampling. Behavior of Endometrial Hyperplasia the chance of development ofsimple hyperplasia without atypia to carcinoma is negligible and within the vary seen in the basic population as a whole. However, this proportion is based upon the experience ofa single patknt out of thirteen equally diagnosed patients who progressed to well-differentiated adenocarcinoma over a 5-year interval. In stark contrast to these knowledge, Longacre and colleagues claim an incidence of myoinw. Differential Diagnosis of Endometrial Hyperplasia the differential prognosis of endometrial hyperplasia includes (a) dissociation, coiling. The distinguishing options of these processes are discussed elsewhere in this chapter, hut a couple of points deserve reiteration. Whenever considering a diagno� sis of localized hyperplasia on the low finish of the spectrum or a loc:al. Another poten� tia1 mimic of a localized endometrial hyperplasia pertains to the frequent finding of elevated glandular density throughout the basalis. Although usually not given more than a passing glance in hysterectomy specimens, this phenomenon could be misinterpreted as hyperplasia (with atypia in instances of "activated" nuclei) when encountered in fragments of tangen� tially cut endometrial samples. Note how tangential sections by way of fragments of basalis may simulate endometrial hyperplasia. Metaplastic hypcrplasias might simply as easily be referred to as hyperplastic metaplasias, but use of the former tertn is most well-liked to emphasize that these processes ought to be considered a form of hyperplasia.
Note the unifonnity of the chromatin sample of the metaplastic cells and the presence of residual mucinous endocervical cells close to the surface symptoms 6 days after embryo transfer 100mg persantine order fast delivery. A: this lesion exhibits some nuclear chromatin abnormalities and has significam mitotic activity symptoms genital herpes persantine 25mg generic with visa. Rarely symptoms anemia persantine 25 mg cheap with amex, the metaplastic process so carefully resembles endomettial epitheliwu that it warrants classification as endometrioid metaplasia. A: Compare the 2 metaplastic glands with the normal endocervical gland at lower proper. A: the metaplastic glands carefully resemble those seen in proliferative endometrium. This distinction is particularly difficult when the metaplastic glands are surrounded by hypercellular stroma, although the stroma in these situations is usually more fibroblastic than endometriotic stroma and tends to blend with the neighboring endocervical stroma. Nuclei arc normally spherical to oval with evenly distributed, finely granular chromatin. Oxyphilic Metaplasia Oxyphilic metaplasia is a uncommon, inconsequential, focal microscopic 6n. Cytologic Features of Tubal Metaplasia and its Distinction from Adenocarcinoma In Situ Although textbook cytologic examples of tubal metaplasia typically present obvious cilia with terminal bars, cilia are delicate constructions which would possibly be easily traumatized and are difficult to discern in follow. Tubal metaplasia usually presents in cytologic preparations as crowded sheets of glandular ceUs that exhibit nuclear enlargement, excessive nuclear to cytoplasmic ratios, hyperchromatidty, and gentle levels of nuclear pleomorphism Transitional Cell Metaplasia Transitional cell metaplasia is an uncommon form of metaplasia that normally presents in postmenopausal women as an incidental discovering. It features a multilayered epithelium composed of uniform, spindiNhaped cells with. The eosinophilic cytoplasm of the metaplastic gland within the decrease left conttasts with cytoplasmic look of the traditional endocervical gland in the higher right. The inset exhibits a Pap smear with metaplastic transitional cells with characteristic longitudinal nuclear grooves. In Pap smears, transitional cell metaplasia could also be recognized as streaming groups of cohesive, spindle-shaped cells with bland nuclear features and longitudinal nuclear grooves. The cysts are normally crammed with translucent, mucoid material, however the contents may sometimes be purulent. A conglomerate of superficially positioned Nabothian cysts is seen distorting the endocervical canal within the left half of the image. This instance is lined by columnar mucinous epithelium and contains purulent particles. Cystic (type B) tunnel dusters are far more common than the noncystic (type A) variant, and are composed of carefully packed, variably sized, mucinp6lled microcystic tubules that type lobular aggregates. By contrast, noncystic tun� nel dusters are chara(:terized by lobulated aggregates of intently packed, small, round to owl, variably compressed glands that often surround a bigger endocervical cleft. Frequently, noncystic tunnel clusters are fOund in association with these of the cystic type. Cysts span the complete thickness of lhe cervical wall in this longitudinal part lexocervix is at left). A: At low magnification, a circumscribed proliferation of small glands is obvious. B: In this instance, the nuclear features resemble these of papillary carcinoma of the thyroid. These nuclear changes are considerably reminiscent of these seen in papillary carcinoma of the thyroid, albeit without distinguished nuclear grooves or pseudoinclusions. The absence of a symptomatic cervical mass, its supcr6cial location inside the cervical stroma, the absence ofa periglandular stromal response, and its noninfiluative, lobular structure help to differentiate noncystic tunnel clusters with nuclear atypia from the usual sort ofendocervical adenocarcinoma and adenoma malignum (minimal deviation adenocarcinoma). The mixture of benign glands with papillary infoldings with patches of squamous me~lasia should raise this risk, which may be confirmed with immunostains for prostate-specific antigen and prostatic acid phosphatase. Heterotopia of Adipose Tissue Adipose tissue is mostly not thought to be a normal constit� uent of the uterine cervix. However, a latest research has sug� gested that fats is present in roughly 15% of specimens of excised cervical tissue, and that its presence must be con� sidered a normal6nding. If the histologic features suggest the presence ofadipose tissue throughout the cervical stroma, a extra likely risk that should first be excluded is pseudolipomatosis (see part on artifacts in cervical samples). The stromal inflammatory infiltrate may be acute (neuttophils) and/or chronic (lymphocytes and plasma cells). Some instances of so-called acute cervicitis may be Prostatic Heterotopia (Ectopia) A rare, intriguing discovering is the presence of prostatic glands inside the uterine cervix. A blended acute and persistent inflammatory infihrate is present within the superficial stroma and metaplastic squamous epithelium. Follicular cervicitis with ill-defined germinal center that incorporates tingible�body macrophages. Since scattered lymphocytes are a norp mal component of the endocervical stroma, the diagnosis of persistent cervicitis should be reserved for conditions in which the number of persistent inflammatory cells is noteworthy and includes the presence of quite a few plasma ceUs. The lining epithelium lacks both mobile strarification and nuclear atypia, which helps to distinguish this incidental continual inflammatory process from nicely. Follicular Cervicitis An uncommon type ofchronic cervicitis is follicular cervicitis, in which germinal facilities secondary lymphoid follicles) kind within the supcr6cial stroma as a part of the chronic inflammatory infiltrate. Papillary Endocervicitis On event, continual inflammation of the endocervix takes the type of micropapillae that project into the endocervical canal. The massive lym� phoid cells are mitotically lively, and a few have the looks of immunoblasts, with single, centrally located macronucleoli. The inset reveals an concerned vessel with fibrinoid necrosis and an related inflammatory infiltrate. Patients are sometimes postmenopausal, and their arteritis may he isolated and asymptomatic or associated with systemic illness. Arteritis Necrotizing arteritis with features resembling polyarteritis nodosa rarely occurs within the feminine genital tract; when it does, it tends to pttferentially involve the cervix. This course of consists of an admixture of huge lymphoid cells/immunoblasts with mitotic exercise. Scattered multinucleated large cells are present inside the vessel wall, which is also chronically inflamed. The microorganisms discussed in tlili section may cause no signs or produce illness which may be primarily based in the vulvovaginal area or other extracervjcaf web site, but are presented here because proof oftheir presence could additionally be present in Pap smears. Emphasis is placed on those microorganisms that either have a attribute morphology or induce comparatively specific epithelial alterations. A: Pap smear with multinucleated cells with a quantity of Cowdry sort A herpetic inclusions. B: Highmagnification view of a histologic section of a multinucleated cell with Cowdry kind A inclusions. Infected cervical tissue not often exhibits vesicles, since thc:y are quickly transfOrmed into shallow ulcers. Since the analysis is commonly primarily based on the clinical analysis, cytology, andlor tradition oflesions in the vulvovaginal n:gion, cetvical tissue samples with proof of herpetic infection are unusual. When cervical biopsies are obtained, viral inclusions are more than likely to be recognized within altered squamous cells from the margins of the ulcerated tissue. Less widespread is the Cowdry type A inttanudear herpetic inclusion, which features a large, centrally positioned, eosinophilic or purple inclusion surrounded by an expensive halo and ~. This type ofinclusion seems to represent a later stage during which virus partides are further concentrated throughout the nucleus. A: Characteristic �ground glass� herpetic inclusions are current within several squamous epithelial cells from the margin of an ulcer. A single characteristic viral inclusion physique is present inside one of the endocervical cells. If the affected person is asymptomatic and immunocompetent, as is usually the case, then no therapy is important. Csndids Species Fungal infection of the cervix by Candida ttlbkans and intently associated organisms corresponding to Candit1a glabrat4 (TorultJpsis) usually represents an extension of vulvovaginal illness. In Pap smears, C albicans seems as an admixture of pseudohyphae and oval, budding~ types ("spaghetti and meatballs"). In liquid-based preparations, squamous epithelial cells might seem to be skew� ered by the pseudohyphae of the extra standard Candida species, creating Cantlid4 "shish kabobs".
If these cardiac conditions exist concurrently symptoms vitamin b12 deficiency persantine 25mg buy amex, then consideration could additionally be given to a heartlung transplant medicine reviews buy 25mg persantine visa. A cardiac catheterization is critical for diagnostic confirmation and evaluation of oxygen and vasodilator response medications in mexico buy 25mg persantine amex. Referral ought to occur when sufferers begin having frequent hospitalizations as a outcome of hypoxemia and/or hypercapnia. Management ought to embrace gastrointestinal and dietary analysis, a bone density scan and therapy of sinus illness. However, with sensitivity testing, directed antibiotic remedy, and lowered ranges of immunosuppression, successful transplantation with acceptable outcomes has been attained. Of course, very few donors will meet all these standards and be categorized as perfect; donors who meet most, however not all criteria are categorized as prolonged donors. Ideally, one of the best lungs within the healthiest recipients provide the very best long-term outcomes. Complications included pulmonary artery thrombosis and extended airleak (>14 days). Living Donor Lobar Lung Transplantation Living donor lobar lung transplantation was first carried out in 1993 on the University of Southern California and was the result of a scarcity of deceased donor organs. These lobes are then implanted into the recipient in lieu of the whole left and right lung. A retrospective evaluate of a prospectively collected database reported in 2006 by Kozower et al identified 39 children who underwent lung retransplantation from 1991 to 2001. Evaluation for transplant is a coordinated effort among a multidisciplinary group of specialized pediatric clinicians, transplant surgeons, pulmonologists, nurse transplant coordinators, dieticians and social employees. In addition, illness specific concerns might involve a psychiatrist, infectious disease specialist, or pediatric cardiologist. At our establishment, gentle tissue flaps are created beneath every breast, before performing a traditional bilateral thoracotomy with sternal division no less than one-third of the sternal distance away from the inferior side of the sternum. A lower division of the sternum leads to instability, patient discomfort and probably the necessity for plate reconstruction. Once on bypass and meticulous hemostasis behind each hilum is achieved, sequential implantation is performed. The implanted lung is gently inflated and ventilated with enough tidal quantity to stop atelectasis. If the lungs are oversized for the pediatric recipient, lobar implantation or wedge resection may be necessary to obtain an appropriate dimension match. One indication could additionally be when a baby has had a earlier pneumonectomy and has vital volume loss into one facet of the chest. When essential, the primary technical Lung Procurement Techniques During procurement, if the guts is being harvested for another establishment, the division of the atrial cuff must be performed at the aspect of the center procurement team. Different strategies of procurement have been performed-en bloc with the trachea or every lung in sequence. In both case, care have to be taken to keep away from procuring too little pulmonary vein or denuding the bronchus. An optimal approach for lung preservation has not been clearly outlined; in one model, hyperinflation to 30 cm H2O with low oxygen concentration (30%) had a protecting position in ischemia reperfusion harm. Exposure through the bilateral thoracosternotomy incision with cannulation for bypass, aortic cross-clamping if needed and excision of both recipient lungs previous to implantation of each donor lung sequentially. Since a peak of forty six heart-lung transplants in 1989 and 40 in 1994, the variety of procedures has steadily declined. Graft half-life has increased in every era for the reason that first heart-lung transplant in 1984. The 5-year survival within the latest period (1999�2008) was forty nine percent, comparable with the 5-year survival after lung transplant in youngsters. The surgical method requires procurement of a heartlung block, dividing excessive on the ascending aorta and the trachea well above the carina. In the recipient, a pericardiectomy is carried out from phrenic nerve to phrenic nerve. Bicaval venous drainage cardiopulmonary bypass is initiated with an arterial cannula high on the ascending aorta. Care should be taken all through the dissection to protect the phrenic and vagus nerves on each side as properly as the recurrent laryngeal nerve around the ligamentum. Daily bronchoscopies are carried out when needed for copious pulmonary secretions or infiltrates on chest roentography. The recipient cardiectomy and bilateral pneumonectomies have been carried out with the patient on cardiopulmonary bypass. Characteristics of worsening dysfunction include radiographic infiltrates consistent with pulmonary edema, PaO2 to FiO2 ratio of < 300 (grade 1), 200 to 300 (grade 2) and < 200 (grade 3). Diligent postoperative care is imperative for a successful consequence and reaching years of optimum graft operate. The 1084 most devastating surgical complication is an airway dehiscence or stenosis. Bronchial stenosis presents with wheezing or an obstructive pattern on a flow-volume loop. Dehiscence could require lobectomy or pneumonectomy, however stents must be averted due to extreme ingrowth of granulation tissue. Other surgical problems could embrace phrenic or vagal nerve harm, chylothorax, or wound infection. Hyperacute rejection occurs from complement-mediated graft injury secondary to preformed recipient antibodies. Treatment for a positive crossmatch includes early plasmapheresis, thymoglobulin and intravenous immunoglobulins. However, diagnosis is simply made by the presence of perivascular and interstitial mononuclear cell infiltrates. Infectious complications because of immunosuppression are additionally a common reason for morbidity. For children who survive to 5 years, 86 % report no limitation in actions. Since the preliminary case in 1987, the sector of pediatric lung transplantation has continued to evolve with vital progress and developments. Perhaps probably the most thrilling future developments will revolve around exvivo lung perfusion. Exvivo lung perfusion promises to provide patients, households, and surgeons the chance to have elective, scheduled transplantation with optimally matched lungs. Until widely obtainable, however, most pediatric lung transplant centers will continue to attempt for elevated long-term survival and decreased morbidity with diligent patient choice and perioperative care. In the earlier decade, lower than 50 % of recipients had obtained induction remedy. The Registry of the International Society for Heart and Lung Transplantation: thirteenth official pediatric heart transplantation report�2010. Registry of the International Society for Heart and Lung Transplantation: Twelfth Official Pediatric Heart Transplantation Report-2009. The Registry of the International Society for Heart and Lung Transplantation: Fourteenth Pediatric Heart Transplantation Report�2011. Registry of the International Society for Heart and Lung Transplantation: tenth official pediatric coronary heart transplantation report�2007. Indications for heart transplantation in pediatric coronary heart disease: a scientific assertion from the American Heart Association Council on Cardiovascular Disease within the Young; the Councils on Clinical Cardiol- outcomes and outcomes the survival fee following lung transplantation in kids is just like that of adult recipients. Improved outcomes of pediatric dilated cardiomyopathy with utilization of heart transplantation. Outcomes of kids with restrictive cardiomyopathy listed for coronary heart transplant: a multi-institutional study. The Journal of heart and lung transplantation: the official publication of the International Society for Heart Transplantation. Ethical issues in listing fetuses as candidates for neonatal heart transplantation. Clinical Report� Guidelines for the Determination of Brain Death in Infants and Children: An Update of the 1987 Task Force Recommendations. Early diagnosis and follow-up by echocardiography of acquired cor triatriatum after orthotopic coronary heart transplantation.
Without a lipid stain medicine to stop contractions buy 100mg persantine visa, it can be troublesome to distinguish Differential Diagnosis � In addition to the usually subje< treatment croup persantine 100 mg buy mastercard. Uular 6brils as demonstrated with a reticulin stain medicine cabinet shelves 25mg persantine order amex, and may be immunoreactive for cytokeratin. The sectioned surface is strong with both gentle gray fibromatous) and yellow (thecomatous) areas. An space of mobile fibroma (top) is adjacent to an area with thecomatous differentiation (bottom). B: In this highmagnification view of the luteinized cells, note the common presence of single outstanding nucleoli. About half of these tumors are related to estrogenic manifestap tions, and one other 10% exhibit androgenic changes. Luteinized thecomas could have both a fibromatous or thecomatous backp floor, with the fOrmer often being mobile and outnumbering the latter by a ratio of roughly 5 to 1. The distinguishing histop logic fi::ature of luteinized thecomas is the presence ofaggregates of luteinized cells that are recognized by their abundant pale to eosinophilic cytoplasm and round nuclei that often comprise single outstanding nucleoli. Rare luteinized thecomas have a peculiar association with sclerosing peritonitis, and have a special set of medical and pathologic options. They may be small to quite massive (average measurement of 10 an), and often exhibit a high mitotic price inside the spindle cell population, stromal edema with formation of microcysts, and entrapped follicular elements. Although occasional sufferers might die related to issues of sclerosing peritonitis, the ovarian masses have behaved in a benign style. The chance that the ovarian lesions truly characterize reactive stromal prolifp erations has rccendy been given severe consideration, and another designation of thecomatosis bas been proposed. Differential Diagnosis the differential prognosis ofluteinized thecoma consists of other rumors in the fibroma-thecoma group, stromal-Leydig cell rumor, steroid cell tumor, and stromal hyperthecosis. In the standard scenario, an ovarian tumor that in any other case has the histologic appearance of a fibroma or cellular fibroma is found to have a number of clusters of luteinized ceUs, at which level the tumor magically transforms into a luteinized thecoma. This view of a bivalved tumor demonstrates a sharplv cin:umscribed, off-white to tannish pink neoplasm with scattered cystic areas. Stewart) Behavior the overwhelming majority of luteinized thecomas are benign, but those with the mixture of high mitotic charges and significant nuclear atypia should be flagged as having recurring potential. The sectioned surface of most tumors is rubbery, predominandy solid, and off-white to pale yellow with edematous areas. Within the cellular islands is a outstanding network of thinwalled vessels which are commonly dilated and irregularly shaped, imparting a resemblance to hemangiopericytoma. When examined at high magnification, the ceUular areas are discovered to be composed of a hodgepodge of rotmd. An alternating sclerotic and edematous area at left merges with a lobulated mobile area at proper. There is an admixture of vacuolated cells with spherical contours and spindle-shaped cells within the mobile regions. These tumors are almost all the time unilateral and are composed ofan admixture ofspindle-shaped sttomal cells with a variably-prominent signet-ring part. In a minority ofsignet-ring stromal tumors, intracytoplasmic and extracellular hyaline globules are present. In contrast, Krukenberg tumors harbor mucin-containing signet-ring cells which are normally admixed with extra obvious epithelial ele-ments. Krukenberg tumors are additionally more doubtless to be bilateral, may be present in association with peritoneal implants and/or ascites, and could additionally be related to a known major malignancy. Note 1he outstanding thinwalled vessels, some of which have a staghom configuration harking back to 1hat seen in hemangiopericytomas. A: Lobulated cellular areas with interspersed microcysts are separated by hyalinizad fibrous bands. Young Immunohistochemistty can be utilized to assist distinguish these two tumors, since signet-ring stromal twnors are typic:ally immunoreactive for vimentin and fall to specific cytokeratin and epithelial membrane antigen, which is the alternative phenotype of that anticipated. Approximately 60% ofcases have focal areas with weird nuclei that seem to characterize a degenerative phenomenon. These tumors should be thoroughly sampled fOr histologic evaluation to exclude the likelihood ofa twnor ofanothet kind with micro cystic change. This lately described tumor is one more example of a particularly rare benign ovarian stromal tumor. The typical presentation is that of a principally strong, unilateral ovarian mass (mean measurement of 9 em) in an grownup girl (mean age of 45 years). The analysis is predicated upon the presence oflobulatcd cellular islands composed of cells with bland nuclear options and minimal mitotic activity that form a microcystic pattern. These lobules are typically separated from one another by bands ofbyalinized fibrous tissue or fibrous plaques. Aside from attainable hormonal manifestations, these tumors may current with belly swelling, stomach pain, incidentally, or not often in affiliation with Peutz. Other widespread architecttual patterns embrace fOrmations of cords, uabeculae, and diffuse sheeu ofsertoliform cells. The fibrous stroma that separates the sertolirorm elements ranges from vin:ually inapparent to thin and delicate to broad and hyalinized. Approximately 10% of Sertoli cell tumors qualify because the lipid-rich variant because of the presence of solid tubules with ample intracytoplasmic lipid, which leads to a transparent, vacuolated look. Another 10% ofcases have ample eosinophilic cytoplasm and are referred to as oxyphil Scrtoli cell tumors. Histologic options that arc extra more likely to he present in those uncommon Scrtoli cell tumors that pursue a maligrwtt scientific course are vital nuclear atypia of a non�degencrative nature, brisk mitotic exercise, and tumor cell necrosis, particu� larly when seen in combination. This instance features stable tubules surrounded by clear spaces which would possibly be associated to retraction artifact. In this instance, the centrally positioned Leydig cell element consists of cells with plentiful eosinophilic cytoplasm. Leydig cells, which have ample cytoplasm that ranges from vacu� olated to eosinophilic, are found in nests inside the stroma. The supporting stroma is variable in quantity and consists of bands of matwe fibrous tissue. Since all well-differentiated twnors reported to date have adopted a benign medical course, unilateral salpingo-oophorectomy is suitable remedy for a younger girl who needs to protect her fertility. B: At excessive magnification, nests of Leydig cells with vacuolated cytoplasm are seen in affiliation with hollow tubules lined by Sertoli cells. Sertoli-Leydig cell tumor of intermediate differentiation with heterologous mucinous components. The sectioned floor of this formalin-fixed tumor from a 17 year-old virilized feminine is composed of pale yellow, lobulated tissue admixed with cystic spaces. Note the presence of inspissated, glistening mucoid materials related to mucinous differentiation. This low-magnification view highlights the mobile lobules which might be a prominent characteristic of most tumors of this type. In this instance, lots of the Sertoli cells type skinny cordlike buildings inside an edematous stroma. Leydig cells, disposed singly and in small clusters, are also present and are significantly evident within the circled area. Subtle evidence ofScrtoli and Leydig cell differentiation is usually best appreciated at the periphery of these lobules. For Scrtoli cells, formation ofepithelial ribbons, cords, and hollow or strong tubules constitute such proof. They can he diffic:ult to diagnose, for the explanation that viable areas typically consist predominantly of solid sheets of mitotically lively ceUs that resemble a sarcoma of no particular type. Sertoli and Leydig cell differentiation is commonly most apparent at tha periphery of cellular nodules. Large portions of these tumors are indistinguishable from sarcomas and other poorlv differentiated malignant neoplasms with a spindle call component. Epitheliallined papillary projections protrude into slit-like areas that are elongated and interconnected. In this situation, massive portions of the polyps present nonspecific fin~, and thorough sampling is nec:cssaty to identifY the retiform dements.
B: this low-magnification view of 1he myometrium reveals several plugs of intravascular tumor surrounded by cleft-like areas treatment for scabies persantine 100 mg order with amex. Jike house that follows the con� tour of the concerned veins symptoms rheumatic fever order persantine 100mg amex, and this ought to be distinguished from leiomyomas with retraction artifact or leiomyomas that are partially surrounded by compressed vascular areas medications 123 cheap persantine 100mg overnight delivery. Dissecting Leiomyoma A very uncommon subset of benign uterine clean muscle tumors exhibits tongue-like extensions that dissect into the neighbor� ing myometrium for a major distance (arbitrarily defined as ~ mm). Recognized as a selected subtype is the coty� ledonoid dissecting leiomyoma, which features an exophytic, bulky. Leiomyosarcoma Leiomyosarcomas are extremely malignant neoplasms that show easy muscle differentiation, both histologically or immunohistochemically. Most occur in patients over 40 years ofage and produce symptoms corresponding to abnormal uterine bleeding. Leiomyosarcomas are generally thought to come up tie Mvo, however current molecular genetic proof suggests that some of these tumors could evolve from preexisting leiomyomas. Leiomyosarcomas are usually solitary tumors of considerable size (mean 10 em) with a gentle. Microscopically, the dassic leiomyosarcoma is a hypercellular spindle cell neoplasm that reveals diffuse important nuclear atypia, a high mitotic rate that includes the presence of atypical division 6gures, infiltration the neighboring myometrium, and geographic foci of tumor ceU necrosis. More subde forms of leiomyosarcoma also exist, similar to people who exhibit only increased cellularity, borderline nuclear atypia, and brisk mitotic activity. This tumor also had a high mitotic index and contained foci of tumor cell necrosis. On gross examination, the rare myxoid leiomyosarcoma is often giant, gelatinous, and well cir<:umscrihed. Epi1helioid Leiomyosarcoma Characteristics of epithelioid histology are mentioned in the section describing epithelioid leiomyomas. The traditional immunoreactivity of epithelioid leiomyosarcomas with no much less than some clean muscle markers and the identification of areas of transition to extra typical easy muscle differentiation with spindle cell morphology facilitate its distinction from poorly differentiated carcinoma, placental site trophoblastic tumor, and other entities with an epithelioid appearance. When deciphering a panel of immunostains on this context, it is important to recall that cytokeratin immunoreactivity may be seen in epithelioid smooth muscle tumors of the uterus. This example features sheets of epithelioid tumor cells with vital nuclear atypia and mitotic exercise embedded inside a hyalinized matrix. A: Sectioned surface of a big myxoid leiomyosarcoma the place the myxoid areas, that are glistening and gelatinous, are most prominent on the periphery and inside a central nodular area. B: the smooth muscle cells in these tumors are extensively separated by abundant myxoid stroma. This hypercellular neoplasm reveals no significant nuclear atypia, sparse mitotic activity, and tumor cell necrosis. The distinction from mobile leiomyoma is predicated on the presence of tumor cell necrosis. It follows that if a quantity of fragments of a well-differentiated endometrial stromal proliferation devoid of glands are encountered in endometrial curettings, a analysis of "endometrial stromal proliferation, nodule vs. Patients with each forms of tumor are commonly beneath 50 years of age, and sometimes present with irregular vaginal bleeding or pdvid stomach ache. The sectioned surfaces of those tumors are fleshy and yellow or tan, with the neoplasm bulging above the neighboring myometrium and missing the whorled appearance of smooth muscle tumors. This tumor has been bisected, revealing its typical fleshy, yellow, nicely circumscribed minimize floor that bulges above the neighboring myometrium. I amounts ofstromaledema may result in a less mobile appearance, and patches ofhyalinized collagen also can alter the architecture. Impact of varying degrees of edema and hyalinization on the appearance of endometrial stromal tumors. Note the concentric whorls of tumor cells swirling around the arterioles, as highlighted within the inset. B: Low-grade endometrial stromal sarcoma with interspersed foamy histiocytes (two separate cases). Hypocellular myxoid stroma is seen adjacent to islands of more mobile tumor with recognizable endometrial stromal differentiation. Endometrioid glandular differentiation in endometrial stromal tumors is often ma. A: Irregular islands of leiomyomatous smooltl muscle interdigitate wim tumor cells that exhibit endometrial stromal differentiation. Note how this sample could be misoonstrued as invasion of myometrium by a low-grade endometrial stromal sarcoma, when this is really a bit from me central side of a sharply circumscribed tumor. B: this high-magnification view reveals the sleek muscle (top) and endometrial stromallbottom! A potential pitfall within the interpretation of endometrial stromal tumors with easy muscle diffi. A radiating focus of central hyalinization inside a paucicellular nodule of easy muscle generates a �starburstw sample. Lowmagnification view demonstrating tumor changing a portion of the endometrium higher right) and infiltrating the myometrium in its characteristic jagged, interdigitating pattern. In approximately half of the cases, there are associated intrauterine worm-like plugs of tumor inside thin-w:illed. In the minority of instances that current with disease extending past the uterus, cords of twnor could additionally be palpated inside the extrauterine veins. Favored websites of recurrences are the pelvis, stomach, and vagina, although metastases are sometimes present in distant websites such as the lung. The major differential diagnostic con� sideration of each twnors is the extremely mobile leiomyoma, distinction from which was discussed earlier on this chapter. Endometrial stromal nodule composed of cells that intently resemble those of regular endometrial stroma from the proliferative phase. Note the sharp demarcation of the endometrial stromal proliferation from the adjoining myometrium (top). Endometrial stromal tumors with sex-cord-like components could be misinterpreted as carcinosarcomas, however the latter tumors typicaily characteristic high-grade carcinomatous and sarcomatous components. Distinction of endometrial stromal tumors with sex-cord-like parts from uterine tumors resembling ovat� ian sex-cord tumors is based upon the absence or inconspicu� ous nature of an endometrial stromal element within the latter. Low-grade endometrial stromal san:oma metastatic to the lung 14 years posthysterectomy. B: Entrapment of nonneoplastic respiratory epithelium can mistakenly recommend the presence of an intrinsic glandular component. The glandular component of adenosarcomas is more regularly dis� ttibuted and options periglandular stromal condensation and/ or formation of epithelial-lined, stromal polypoid constructions that project into cysticaily dilated glands or into the endometrial cavity. Myometrial invasion is usually in the form of a broad entrance of tumor that replaces rather than intcrdigitates with the myometrium. The tumors develop as cellular shecu which will �Not~: the "poody ~tiatl:d ettdometrial RtWrm. Note the permeative pattam of infiltration by geographic islands of tumor; which in 1his case reveal transmural involvement and formation of �colon polyps" 1hat could probably be sampl9d by a gastroenterologist. The sectioned floor of this fixed specimen demonstrates a large, polypoid, intracavitary, fleshy tumor with outstanding areas of hemorrhage and necrosis. The tumor is firmly connected to and impinges upon a thinned myometrium, which it invaded superficially. Since undifferentiated endometrial sarcomas could have histologic features which may be indistinguishable from the sarco� matous component of a carcinosarcoma. Due to their rarity and the variable inclusion standards utilized for such instances, limited follow-up info is available for th. They are sometimes sharply demarcated from the adjacent endometrium and myometrium. The architectural abnormalities and diploma of cytologic atypia of the glandular component vary from th. The squamous morulcs are often outstanding and may comprise foci of central necro� sis. The stromal component consists of interwoven fascicles of cellular, bland clean muscle, and/or myofibromatous tissue. This instance contains a lobulated cluster of crowded endomettial glands with scattered squamous morules. Atypical endometrial glands and a squamous morula are embedded within a cellular fibromuscular stroma.
Syndromes
Serum Human Chorionic Gonadotropin Levels If a optimistic pregnancy take a look at is found when ectopic being pregnant is suspected treatment definition statistics persantine 25mg generic with amex, the rest of the workup should concentrate on evaluating the viability and site of the being pregnant medications 25 mg 50 mg persantine 100 mg order on line. The yolk sac appears between 5 and 6 weeks treatment tmj 100mg persantine discount with mastercard, and a fetal pole with cardiac activity is first detected at 5� to 6 weeks. Care should be taken 417 to differentiate between a uterine gestation and a pseudogestational sac. This one-layer sac is the end result of an intracavitary fluid collection attributable to sloughing of the decidua typically situated within the midline of the uterine cavity, whereas a traditional gestational sac is eccentrically situated. Sagittal transabdominal view of the uterus demonstrates a pseudogestational sac, a group of fluid within the uterus. There is minimal variation in serum progesterone focus between 5 and 10 weeks of gestation; thus a single value is sufficient. A serum progesterone stage of <5 ng/mL has been used to establish a nonviable pregnancy with 98% specificity and with a sensitivity of 75%. Conversely, a serum progesterone of >20 ng/mL has a sensitivity of 95%, with a specificity of roughly 40% to determine a healthy being pregnant. Although intrauterine and ectopic pregnancies can exist concurrently in uncommon circumstances (heterotopic pregnancy), identification of chorionic villi in tissue samples identifies an intrauterine location of the pregnancy and primarily rules out ectopic pregnancy. The presumptive diagnosis of ectopic pregnancy is reportedly inaccurate in almost 40% of cases without histologic exclusion of a spontaneous pregnancy loss. An 18G needle is inserted posterior to the cervix, between the uterosacral ligaments, and into the cul-de-sac of the peritoneal cavity. Aspiration of blood that clots can indicate either penetration of a vessel or such fast blood loss into the peritoneal cavity that the blood clot has not had time to bear fibrinolysis. Aspiration of nonclotting blood is proof of hemoperitoneum (positive culdocentesis), during which the blood clot has undergone fibrinolysis. If nothing is aspirated (equivocal or nondiagnostic culdocentesis), no information is obtained. Purulent fluid suggests a variety of infection-related causes, corresponding to salpingitis and appendicitis. Because none of the possible findings on culdocentesis can definitively confirm the presence or absence of ectopic being pregnant, its use in medical follow is proscribed. With the availability of 421 other diagnostic expertise, notably ultrasound, in many areas the use of culdocentesis has turn into virtually obsolete. Laparoscopy probably the most accurate strategy of identifying an ectopic pregnancy is by direct visualization, which is completed mostly by way of laparoscopy. For instance, an especially early tubal gestation may not be recognized as a end result of it might not distend the fallopian tube sufficiently to be recognized as an abnormality (false negative). Conversely, a false-positive prognosis could outcome from a hematosalpinx (blood in the fallopian tube) being misinterpreted as an unruptured ectopic being pregnant or tubal abortion. Management Management could additionally be both surgical or medical, depending on a selection of components. Due to the inherent risks of each, medical therapy is most well-liked over surgical procedure in applicable sufferers. Medical Management Methotrexate is the medical treatment usually used as an alternative selection to surgical remedy. Methotrexate is a folic acid antagonist that competitively inhibits the binding of dihydrofolic acid to dihydrofolate reductase, which, in flip, reduces the amount of the energetic intracellular metabolite, folinic acid. Relative and absolute contraindications for medical administration are listed in Box 19. Ectopic being pregnant measurement also appears to impact methotrexate success rates. The commonest side effects of methotrexate include nausea, vomiting, diarrhea, gastric misery, dizziness, and stomatitis. Intramuscular methotrexate given as part of a single-dose protocol has been probably the most broadly used medical therapy of ectopic being pregnant. During the first few days following methotrexate administration, as a lot as half of girls expertise stomach ache that may be controlled with nonsteroidal anti-inflammatory medication. This pain presumably outcomes from tubal distention, tubal abortion, and/or hematoma formation. Methotrexate given in a multidose protocol has additionally been used successfully, but the single-dose protocol described appears to scale back the amount of potential problems whereas reaching related success charges. In some cases, an agent may be administered systemically, but sometimes it might be injected directly into the ectopic being pregnant. Conservative surgical methods have been developed that maximize preservation of the fallopian tube. If removing is finished through the laparoscope, definitive prognosis in addition to remedy could be accomplished on the identical operation with minimal morbidity, price, and hospitalization. In a linear salpingostomy, the surgeon makes an incision on the fallopian tube over the positioning of implantation, removes the pregnancy, and permits the incision to heal by secondary intention. Salpingectomy is removing of the whole tube, a procedure reserved for these circumstances in which little or no regular tube remains. Rh-negative mothers with ectopic being pregnant ought to receive Rh immunoglobulin to stop Rh sensitization (see Chapter 23). Non�Fallopian Tube Ectopic Pregnancy Ovarian Pregnancy Ectopic implantation of the fertilized egg within the ovary is uncommon. Diagnosis is predicated on the basic sonographic description of a cyst with a wide echogenic vascular outer ring positioned on or throughout the ovary. Interstitial Pregnancy Also termed cornual being pregnant, interstitial pregnancies implant in the proximal tubal segment that lies within the muscular uterine wall. Swelling lateral to the insertion of the spherical ligament is the characteristic anatomic finding. A being pregnant that implants in the cornual segment of the tube tends to current several weeks later in being pregnant, as a result of the muscular cornu of the uterus is healthier able to broaden and accommodate an enlarging being pregnant. As a outcome, rupture of a cornual pregnancy usually occurs between the eighth and 16th gestational weeks and is often associated with large hemorrhage, generally requiring hysterectomy. Cervical Pregnancy 426 Cervical being pregnant happens in 1 in 9,000 to 12,000 pregnancies, when the ovum implants in the cervical mucosa beneath the extent of the histologic cervical inside os. Two diagnostic criteria are necessary for affirmation of cervical being pregnant: (1) the presence of cervical glands opposite to the placental attachment website and (2) a portion of or the whole placenta should be located beneath both the entrance of the uterine vessels or the peritoneal reflection on the anterior and posterior uterine surface. Both medical and surgical management have been used efficiently to protect the cervix in instances where future fertility is desired. Heterotopic Pregnancy Heterotopic being pregnant (coincident or mixed pregnancy) is the coexistence of an ectopic and an intrauterine pregnancy. As a result of assisted copy, however, the rate of heterotopic pregnancies has elevated to as high as 1 in a hundred pregnancies in some sequence. Mechanisms which have been proposed to explain this embrace (1) hydrostatic forces delivering the embryo into the cornual or tubal space, (2) the tip of the catheter directing switch towards the tubal ostia, or (3) reflux of uterine secretions leading to retrograde tubal implantation. In addition to the option of surgical management of the ectopic being pregnant while attempting to protect the intrauterine pregnancy, medical remedy by which potassium chloride can be injected into the pregnancy sac is an alternative choice. Methotrexate is contraindicated due to potential detrimental effects on the conventional being pregnant. Abdominal Pregnancy the estimated incidence of belly pregnancy ranges from 1 in 10,000 to 1 in 25,000 reside births. Abdominal pregnancies might end result from primary implantation onto the peritoneal surface or secondary implantation via tubal rupture or tubal abortion. Physical findings and signs are broadly variable, relying on gestational age and web site of implantation. Abdominal being pregnant is normally discovered long earlier than fetal viability, and elimination of the being pregnant is the mainstay of therapy. Survival of the fetus occurs in solely 10% to 20% of cases; up to one half 427 of those surviving have significant deformity. The affected person is given the option of continuing the being pregnant to fetal viability with operative supply or operative termination of the pregnancy at the time of prognosis. In either case, elimination of the placenta is normally not attempted due to the chance of uncontrollable hemorrhage. Alternative therapies embrace administration of methotrexate and embolization of placental vessels. Miscarriage (spontaneous abortion) occurs within the absence of any medical or surgical intervention. The incidence of acknowledged miscarriage is often cited as 15% to 25%, with 80% occurring during the first 12 weeks of pregnancy. This rate of miscarriage could also be even higher because losses that happen at 4 to 6 weeks of gestation may be misinterpreted by the patient and her physician as a delayed menstrual cycle.
Other urinary tract problems that will complicate pregnancy include urinary calculi medications side effects persantine 100mg cheap without prescription, nephrolithiasis medicine 906 100mg persantine safe, and preexisting renal disease medications kidney failure 25 mg persantine cheap with visa. Asymptomatic Bacteriuria and Uncomplicated Urinary Tract Infection Compared with nonpregnant women with comparable colony counts on urine tradition, asymptomatic bacteriuria in being pregnant is extra more probably to lead to cystitis and pyelonephritis. The elevated incidence of symptomatic infection during being pregnant is believed to be caused by pregnancyassociated urinary stasis and glucosuria. This relative urinary stasis in pregnancy is a result of progesterone-induced decreased ureteral tone and motility, mechanical compression of the ureters at the pelvic brim, and compression of the bladder and ureteral orifices. In addition, the pH of urine is increased due to elevated bicarbonate excretion, which additionally enhances bacterial development. A urine tradition is obtained on the onset of prenatal care, and patients with asymptomatic bacteriuria are treated with ampicillin, cephalexin or nitrofurantoin. Also, recurrence rates for asymptomatic bacteriuria strategy 30% even with efficient therapy. Consideration must be given to postpartum radiographic analysis of these sufferers to establish renal 464 parenchymal and urinary-collecting duct abnormalities. Acute cystitis occurs in approximately 1% of pregnancies and might manifest with dysuria, urinary frequency, and urgency. Pyelonephritis Patients with pyelonephritis (inflammation of the renal parenchyma, calices, and pelvis) are acutely sick, with fever; costovertebral tenderness; common malaise; and, usually, dehydration. Pyelonephritis happens in 2% of all pregnant sufferers and is amongst the most common medical complications of pregnancy requiring hospitalization, particularly in its context as a serious cause of maternal mortality (septic shock). Treatment After urinalysis and urine culture are obtained, patients are handled with intravenous hydration and antibiotics, generally a cephalosporin or ampicillin and gentamicin. Fever can be known to induce contractions, so antipyretics are required for a temperature >100. Ultrasonography or different imaging study similar to computed tomography will sometimes establish a calculus or abscess. The organisms mostly cultured from the urine of symptomatic pregnant patients are E. Follow-up may be with either frequent urine cultures and/or empiric antibiotic suppression with an agent such as nitrofurantoin. In these sufferers, a complete urologic analysis 6 weeks after being pregnant could additionally be warranted. Symptoms similar to these of pyelonephritis however with out fever recommend urinary calculi. Renal colic (pain) is a typical symptom in nonpregnant women however is seen much less regularly in pregnant ladies because of the hormone-induced relaxation of ureteral tone. Usually, hydration and expectant management, along with straining of urine seeking stones, suffice as management. Occasionally, however, the presence of a stone can result in infection or full obstruction, which may require urology session and drainage by either ureteral stent or percutaneous nephrostomy. Pregnancy end result is expounded to the degree of serum creatinine elevation and the presence of hypertension. Many patients with renal illness also have preexisting or concurrent hypertension. Pregnancy following renal transplantation is generally related to an excellent prognosis if no much less than 2 years have elapsed because the transplant was performed and thorough renal evaluation reveals no proof of active disease or rejection. In early gestation, ectopic being pregnant and torsion of the adnexa should be considered. Later in being pregnant, placental abruption and uterine rupture can cause acute stomach indicators and signs (see Section "Trauma in Pregnancy"). Considerations for Pregnant Patients Surgical remedy of a pregnant woman ought to take into consideration each maternal and fetal well being wants. For procedures similar to radiographs of the chest, an belly protect could additionally be used to avoid unnecessary exposure to the fetus. Exposure to low doses of radiation is protected for the fetus when considered in opposition to failure to treat or to diagnose a situation requiring surgical procedure. In the perioperative period, fetal heart tones ought to be monitored to the extent attainable, according to the stage of gestation and want for intervention, usually by digital fetal monitoring. Instead the affected person ought to be placed in a decubitus lateral tilt to forestall supine hypotensive syndrome, by which strain on the vena cava reduces venous return to the center, causing a drop in blood stress and uterine blood move. In general, clinicians caring for these patients should be constantly aware of each maternal and fetal concerns. For example, the residual lung volume is diminished in being pregnant, which supplies much less reserve for respiratory perform. Delayed 467 gastric emptying makes aspiration of abdomen contents throughout a surgical procedure extra likely. Cholelithiasis can be exacerbated during being pregnant due to hormonal effects that gradual gallbladder emptying and trigger an increase in residual gallbladder volume. If the affected person develops biliary colic, makes an attempt ought to be made to conservatively deal with the patient with hydration, pain control, dietary restriction, and potential nasogastric tube. However, if cholecystitis occurs with common bile duct obstruction, ascending cholangitis, pancreatitis, or acute abdomen, immediate surgical administration is required. Maternal and fetal outcomes are likely to be glorious if surgical removing is undertaken before these severe penalties are allowed to worsen. As with appendicitis, conventional surgical management has been open cholecystectomy; nonetheless, in latest years, more proof helps the protected use of laparoscopic cholecystectomy in being pregnant. Appendicitis in Pregnancy Appendicitis is a standard surgical downside in reproductive-aged girls, and, due to this fact, a typical surgical drawback in being pregnant. Similar signs of the disease happen in pregnancy; of note, leukocytosis associated with appendicitis could additionally be masked with the conventional leukocytosis of being pregnant. The appendix could additionally be displaced upward as pregnancy advances and might cause a shift within the location of belly ache related to appendicitis, though pain continues to be most commonly positioned in the proper decrease quadrant. When appendicitis is identified and treated early (before appendiceal rupture and generalized peritonitis), fetal and maternal outcomes are good. Surgical administration has traditionally been with open appendectomy; nonetheless, laparoscopy is increasingly being utilized for the administration of appendicitis in being pregnant. Adnexal Masses in Pregnancy Abnormal ovarian or adnexal masses can occur in pregnancy. Often, they 468 are found throughout routine ultrasound examination of the fetus. For these causes, expectant administration is usually advocated for adnexal lots in pregnancy. Surgical management is usually reserved for sufferers with symptoms or a excessive index of suspicion for malignancy. In basic, surgical administration is best carried out in the second trimester and could also be safely accomplished laparoscopically. The second most common trigger is physical violence against ladies, most incessantly companion violence. Traumatic harm can outcome in maternal injury and demise, in addition to placental abruption, uterine rupture, fetal�maternal hemorrhage, premature rupture of membranes, or preterm labor. In addition to the above situations, which may compromise fetal well-being, direct fetal harm is also attainable. Management the first goal for analysis of a pregnant trauma patient is maternal stabilization. Vital signs should be assessed and the affected person stabilized, adopted by obstetric assessment. If the gestational age is 20 weeks or past, the patient should be placed in a decubitus lateral tilt place. Fetal evaluation includes verification of fetal heart tones with Doppler, followed by electronic fetal monitoring as quickly as the secondary survey is full. Fetal ultrasound is also helpful for figuring out location of placenta, fetal wellbeing, amniotic fluid quantity, and estimated gestational age. If, during that interval, there are any signs of uterine tenderness, irritability or contractions, vaginal bleeding, rupture of membranes, or nonreassuring fetal standing, continued monitoring for a minimal of 24 hours is advocated. Fetal�Maternal Hemorrhage Fetal�maternal hemorrhage is another complication of maternal trauma, and determination of Rh standing is an important a half of the administration. The extent of fetal�maternal hemorrhage can be determined using certainly one of several checks. Most often, an everyday dose of Rh immunoglobulin is protective for all Rh-negative mothers. If a pregnant woman undergoes cardiopulmonary arrest, makes an attempt at resuscitation should start immediately.
These variable decelerations might start before medicine ok to take during pregnancy generic persantine 100mg fast delivery, throughout medications like xanax persantine 25mg order otc, or after uterine contraction starts medications knee 25 mg persantine purchase fast delivery, therefore the time period "variable. They are usually associated with umbilical cord compression, which can end result from wrapping of the twine around components of the fetus, fetal anomalies, and even knots within the umbilical cord. They are additionally generally related to oligohydramnios, by which the buffering space for the umbilical cord created by the amniotic fluid is misplaced. They are sometimes correctable by changes within the maternal position to relieve strain on the umbilical wire. Four methods are available to stimulate the fetus: 1) fetal scalp sampling, 2) Allis clamp scalp stimulation, 3) digital scalp stimulation, and 4) vibroacoustic stimulation. Each of the primary three techniques includes accessing the fetal scalp by way of the dilated cervix. In vibroacoustic stimulation, the fetus is stimulated when the system is positioned on the maternal stomach over the realm of the fetal head. In digital scalp stimulation, the physician makes use of his or her finger to gently stroke the scalp. Each of these checks is a reliable method to exclude acidosis if accelerations are noted after stimulation. However, using scalp pH has decreased, and it will not be obtainable at some tertiary hospitals. If the pattern persists, initial measures include inserting the affected person in the left lateral position, administering oxygen, correcting maternal hypotension, and discontinuing oxytocin, if acceptable. Uterine tachysystole could be recognized by evaluating uterine contraction frequency and duration and may be handled with -adrenergic drugs. Awaiting vaginal supply is acceptable if it has been determined that supply is imminent. It is composed of amniotic fluid, lanugo (the fine hair that covers the fetus), bile, and fetal skin and intestinal cells. However, the fetus might pass the meconium in utero, which is a sign of fetal stress. Meconium passage is detected during labor when the amniotic fluid is stained dark green or black. Meconium aspiration syndrome, a condition brought on by inhalation of meconium-stained amniotic fluid by the fetus, happens in about 6% of births in which meconium is present. Severe circumstances of this syndrome could trigger pneumonitis, pneumothorax, and pulmonary artery hypertension. In the presence of meconium-stained amniotic fluid, routine suctioning or intubation is now not really helpful; 279 however, a credentialed neonatal resuscitation group should be available in case endotracheal intubation is needed. You evaluate the estimated fetal weight and position of the fetal vertex in the pelvis prior to augmenting her labor. The labor had been unremarkable except for delicate meconium staining of the amniotic fluid till the final minutes of the second stage when descent to supply appeared beyond the expulsive efforts of the exhausted patient, and deep variable decelerations are famous. The estimated fetal weight was 6 lb, and the vertex was occiput-anterior and simply on the level of the perineum. It was instructed to the dad and mom that a vacuum-assisted vaginal supply could be prudent, and, with explanation, they gave consent for the operative obstetric procedure. The preterm new child has special wants; these issues are mentioned in Chapter 15. Immediately following supply, the new child infant ought to be first assessed to determine whether or not resuscitation is critical. Three traits outline a newborn that requires no additional resuscitation: 1. Good muscle tone Ballard Scoring System In an effort to predict which newborns would require more intensive resuscitation, the gestational age ought to be estimated as accurately as attainable before delivery. This allows the appropriate neonatal group to be present and ready for resuscitation. It can also be attainable to assess the infant gestational age after supply utilizing the Ballard scoring system. The Ballard scoring system makes use of a specified set of bodily examinations of neuromuscular and bodily maturity which, when scored, yields an estimated gestational age. The Ballard scoring system uses factors assigned to observations about neuromuscular maturity and bodily maturity. Scores are assigned at 1 and 5 minutes, and at every 5 minutes till 20 minutes thereafter if the 5-minute Apgar rating is less than 7. In the time period and late-preterm infant, a 5-minute Apgar rating of 7 to 10 is reassuring; a 5-minute score of 4 to 6 is considered indicative of a mildly to moderately depressed toddler; and a 5-minute rating of lower than four is suggestive of a severely depressed infant. This term is properly outlined and is addressed in Section "Umbilical Cord Blood Gases. The 5-minute Apgar rating can be used to evaluate the effectiveness of any resuscitative efforts which have been undertaken or to determine an toddler who wants continuing analysis and management. It is important for the delivery team to keep in mind to carry out these duties at a later time for newborns that require resuscitation. Delayed cord clamping after 30 seconds is usually really helpful for both term and preterm infants, though instant wire clamping may be warranted of sure maternal. There is inadequate evidence to suggest an strategy to wire clamping for infants who require resuscitation at birth. The solely antagonistic consequence found was a barely increased level of bilirubin in time period infants, associated with more want for phototherapy. Warming First, the new child toddler is thoroughly dried to preserve applicable physique temperature. Warm blankets, skin-to-skin contact with the mother, or a radiant warmer can all accomplish this task. For healthy, vigorous, time period neonates, skin-to-skin contact promotes maternal�infant bonding and initiation of breastfeeding in the first hour of life. Premature infants have extra problem sustaining their physique temperature and are extra vulnerable to chilly stress. These infants require warming pads, heated towels, and a preheated radiant hotter to keep warm. However, these agents could cut back neonatal morbidity and mortality in low-resource settings. The umbilical twine loses its bluish-white appearance throughout the first 24 hours after delivery. After a number of days, the blackened, dried stump sloughs, leaving a granulating wound. If twine blood banking has been requested, the pattern must be obtained and stored on the time of supply. It is necessary to note that delayed twine clamping will considerably decrease the amount and whole nucleated cell counts of cord blood Vital Signs Another essential element of routine care is the evaluation of significant signs. Practices to Promote Breastfeeding Maternity care practices can affect breastfeeding success and the obstetrician is in a singular position to impact adjustments in postpartum care to positively have an effect on change via encouragement throughout pregnancy and especially postpartum. Randomized controlled research have demonstrated that skin-to-skin care within the first hour of life increased the duration of breastfeeding by over 42 days. Transitional Care Following the preliminary assessment and routine care of a wholesome neonate, continued shut statement is necessary for the following stabilization� transition period (the first 6 to 12 hours after birth) to identify any 286 problems that will arise. The following findings should elevate concern and lead to closer statement: temperature instability; change in activity, together with refusal of feeding; uncommon skin coloration; irregular cardiac or respiratory activity; abdominal distention; bilious vomiting; excessive lethargy or sleeping; delayed or irregular stools; and delayed voiding. Give newborns no food or drink other than breast milk, until medically indicated. Practice rooming-in � enable moms and newborns to remain together 24 hours a day. Foster the institution of breastfeeding support groups and refer to them on discharge from the hospital or delivery middle. Antimicrobial ophthalmic prophylaxis is really helpful for all neonates quickly after delivery however may be delayed till after the initial breastfeeding 287 within the supply room. Every newborn must also obtain a parenteral dose of pure vitamin K1 oxide (phytonadione, zero. This form of administration is efficacious, and no commercial oral vitamin K preparation is approved to be used within the United States at this time. This measure also can be delayed for as a lot as 1 hour to permit breastfeeding in the first hour of life.
The speculum is then directed posteriorly at an roughly 45� angle from horizontal; the angle is adjusted as the speculum is inserted treatment bronchitis 100 mg persantine discount, so that the speculum slides into the vagina with minimal resistance medicine 44 159 buy discount persantine 25mg. As the speculum is inserted symptoms 7 dpo bfp 100mg persantine buy with amex, a slight steady downward pressure is exerted in order that distension of the perineum is used to create space into which the speculum may advance. Taking benefit of the distensibility of the perineum and vagina posterior to the introitus is a crucial concept for the environment friendly and cozy manipulation of the speculum examination (and later for the bimanual and rectovaginal examination). Pressure superiorly causes pain in the sensitive area of the urethra and clitoris and ought to be deliberately averted. With slight tilting of the speculum, the cervix slides into view between the blades of the speculum. Failure to find the cervix most commonly results from not having the speculum inserted far enough, often because of concern of inflicting patient discomfort. When the speculum is locked into position, it often stays in place without being held. For most sufferers, the speculum is opened sufficiently by use of the higher thumbscrew. This could also be obtained by gently increasing the vertical distance between the speculum blades by means of the screw on the deal with of the speculum. With the speculum in place, the cervix and the deep lateral vaginal vault could also be inspected and specimens obtained of any discharge or lesion. Before obtaining samples for the Pap test, the affected person should be advised that she could feel a slight "scraping" sensation however no ache. Specimens are collected to fully evaluate the transformation zone, where cervical forty five intraepithelial neoplasia is extra prone to be encountered. Specimens are obtained from the exocervix and endocervix and either plated on slides, which are immediately fastened with a preservative spray, or positioned in a liquid assortment medium. After telling the patient that the speculum is to be eliminated, the blades of the speculum are opened slightly by putting stress on the thumb hinge, and the thumbscrew is completely loosened. Opening the speculum blades slightly earlier than starting to withdraw the speculum avoids pinching the cervix between the blades. The blades of the speculum are naturally brought together by vaginal wall strain. As the top of the speculum blades approaches the introitus, there must be no stress on the thumb hinge, as in any other case the anterior blade can flip up, hitting the delicate vaginal, urethral, and clitoral tissues. Bimanual Examination the bimanual examination uses each a "vaginal" hand and an "abdominal" hand to entrap and palpate the pelvic organs. The bimanual examination begins by exerting light pressure on the abdomen roughly midway between the umbilicus and the pubic hair line with the stomach hand, whereas inserting the index and center fingers of the forty six vaginal hand into the vagina to approximately 2 in. The patient is requested to feel the muscle tissue being pushed on and to loosen up them as much as possible. Then both the index and center fingers are advanced into the vagina until they rest at the limit of the vaginal vault in the posterior fornix behind and below the cervix. Occasionally, only the index finger of the vaginal hand could be comfortably inserted. During the bimanual examination, the pelvic buildings are "caught" and palpated between the belly and vaginal arms. Whether to use the dominant hand as the belly or vaginal hand is a query of personal desire. A frequent error on this a part of the pelvic examination is failure to make efficient use of the belly hand. Pressure must be utilized with the flat part of the fingers, not the fingertips, beginning halfway between the umbilicus and the hairline, shifting downward in conjunction with upward movements of the vaginal hand. The bimanual examination continues with the circumferential examination of the cervix for its dimension, form, position, mobility, and the presence or absence of tenderness or mass lesions. Bimanual examination of the uterus is achieved by lifting the uterus up toward the belly fingers in order that it might be palpated between the vaginal and stomach hands. The uterus is evaluated for its measurement, form, consistency, configuration, and mobility; for masses or tenderness; and for position. The uterus may tilt on its long axis (from cervix to fundus, version) yielding three positions (anteverted, midposition, and retroverted). It can also tilt on a shorter axis (from just above or at the space of the lower uterine segment, flexion) yielding two positions (anteflexed and retroflexed). A posterior cervix is usually related to an anteverted or midposition uterus, whereas an anterior cervix is commonly associated with a retroverted uterus. The bimanual examination approach varies considerably with the position of the uterus. Examination of the anterior and midposition uterus is facilitated with the vaginal fingers lateral and deep to the cervix within the posterior fornix. The uterus is gently lifted upward to the abdominal fingers and a delicate side-to-side "searching" motion of the vaginal fingers is combined with steady strain and palpation by the belly hand to determine the traits of the uterus. In some cases, the vaginal fingers could also be slowly pushed below or at the level of the uterine fundus, after which gentle stress exerted inward and upward causes the uterus to antevert, or a minimal of to move "upward," somewhat facilitating palpation. Bimanual examination of the adnexa to assess the ovaries, fallopian forty eight tubes, and assist structures begins by putting the vaginal fingers to the aspect of the cervix, deep within the lateral fornix. The stomach hand is moved to the identical side, just inside the flare of the sacral arch and above the pubic hairline. Pressure is then utilized downward and toward the symphysis with the belly hand, on the same time lifting upward with the vaginal fingers. The identical movements of the fingers of each arms used to assess the uterus are used to assess the adnexal constructions, which are introduced between the fingers by these maneuvers to evaluate their dimension, form, consistency, configuration, mobility, and tenderness as nicely as to palpate for plenty. Special care should be taken when inspecting the ovaries, that are delicate even in the absence of pathology. The ovaries are palpable in regular menstrual ladies approximately half of the time, whereas palpation of ovaries in postmenopausal girls is much less frequent. Rectovaginal Examination When indicated, a rectovaginal examination forms part of the entire pelvic examination on preliminary and annual examination as nicely as at interval examinations each time clinically indicated. The rectovaginal examination is begun by changing the glove on the vaginal hand and using a liberal supply of lubricant. The examination could also be comfortably performed if the pure inclination of the rectal canal is adopted: upward at a 45� angle for roughly 1 to 2 cm, then downward. This is completed by positioning the fingers of the vaginal hand as for the bimanual examination, except that the index finger is also flexed. The middle finger is then gently inserted via the rectal opening and inserted to the "bend" where the angle turns downward. The index (vaginal) finger is inserted into the vagina, and both fingers are inserted till the vaginal finger rests within the posterior fornix below the cervix, and the rectal finger rests as far as it might possibly go into the rectal canal. Palpation of the pelvic buildings is then achieved, as in their vaginal palpation. The rectal canal is evaluated, as are the integrity and 49 function of the rectal sphincter. After palpation is full, the fingers are quickly however steadily removed in a reversal of the sequence of movements used on insertion. At the conclusion of the pelvic examination, the affected person is asked to move again up on the desk and, thereafter, to sit up. If a problem exists, the history and bodily findings assist set up a differential diagnosis. A presumptive analysis is made, and a administration plan agreed upon between the affected person and 50 doctor. Amelioration of symptoms and other evidence of remedy success confirm the analysis. If unsuccessful, the physician is led to further evaluation and consideration of latest administration plans. If the patient has had a preventive well being care examination, issues that come up during the historical past and physical examination and a long-term plan for addressing these points must be discussed. The patient and physician agree on a plan of action, which may include behavior modification, lifestyle modification, referral to another doctor or well being care or social companies skilled, or referral to community assets. Screening tests and immunizations which may be acceptable for the patient must also be administered (see Chapter 2). With thyroid hormone alternative, much of her sensation of feeling cold resolves over the subsequent few months with a commensurate enchancment in the quality of her life and a modest lower in weight. They ought to be in a position to describe acceptable screening protocols for most cancers, heart problems, and osteoporosis.

Transmission of 196 the disease-producing genetic mutation to a fetus is dependent upon the intercourse of the mother or father and the variety of repeats within the parental gene medications xerostomia persantine 25mg online. If the number of repeats is between sixty one and 200 68w medications effective 100mg persantine, the person is alleged to have a "premutation medications 5 songs cheap 25mg persantine amex. A male could transmit the unexpanded premutation gene to his offspring, but growth to the full mutation is rare in a male with the premutation gene. A feminine with a premutation gene can also transmit the gene to her offspring; nevertheless, the premutation gene may increase during meiosis and result in a full mutation. Women with a household historical past of boys with developmental delay, extreme hyperactivity, and speech and language problems ought to be supplied fragile X�carrier testing. Women with ovarian failure or an elevated follicle�stimulating hormone degree earlier than age forty years and not utilizing a recognized cause ought to be screened to decide whether they have the fragile X premutation. Mitochondrial Inheritance Mitochondrial inheritance is totally different from other patterns of inheritance. Multifactorial Inheritance Multifactorial problems are brought on by a combination of things, some genetic and a few nongenetic. Many congenital, single-organ system structural abnormalities are multifactorial, having an incidence within the general inhabitants of approximately 1 per 1,000. Other components, corresponding to ethnicity or a household historical past of a illness, may point out that an individual carries a gene for a Mendelian dysfunction. This record is an effective methodology for obtaining data regarding personal and household medical historical past, parental exposure to potentially harmful substances, or other issues that may have an impact on threat assessment and administration. This info may be collected previous to conception throughout a preconception workplace visit or through the first prenatal go to in the first trimester. Some infectious ailments, together with cytomegalovirus, rubella, and sexually transmitted illnesses (see Chapter 24), in addition to sure medication (see Chapter 6) have been linked to an increased danger of delivery defects. Preexisting diabetes mellitus can also predispose a fetus to a congenital anomaly. Ultrasonography is the mainstay of surveillance for infectious and teratogen-induced congenital abnormalities. Advanced Maternal Age Although the risk increases with age, the majority of instances of Down syndrome happen in girls youthful than age 35 years (Table 7. In addition to Down syndrome, different chromosomal abnormalities improve in frequency with advanced maternal age (see Table 7. Some, but not all, intercourse chromosome abnormalities carry an increased threat of recurrence. History of Early Pregnancy Loss At least half of all first-trimester being pregnant losses end result from fetal chromosomal abnormalities. The most common are monosomy X; polyploidy (triploidy or tetraploidy); and trisomies 13, sixteen, 18, 21, and 22. Advanced Paternal Age Increasing paternal age, significantly after age 50 years, predisposes the fetus to a rise in gene mutations that may affect X-linked recessive and autosomal dominant issues, such as neurofibromatosis, achondroplasia, Apert syndrome, and Marfan syndrome. African Americans are at an elevated risk for sickle cell illness, the most typical hemoglobinopathy in the United States. Approximately 8% of African Americans carry the sickle hemoglobin gene, which can be discovered with increased frequency in those of Mediterranean, Caribbean, Latin American, and Middle Eastern descent. Caucasians of Northern European descent are at an increased threat for cystic fibrosis, with an estimated service proportion of 1 in 22. Tay-Sachs, Gaucher, and Niemann-Pick ailments 200 happen with greater frequency in individuals of Ashkenazi Jewish descent. Other illnesses associated with certain ethnic teams are -thalassemia discovered at an increased frequency in people of Mediterranean origin, and -thalassemia in people of Asian origin. Prenatal genetic diagnostic testing is meant to determine, with as much certainty as potential, whether a selected genetic disorder or condition is current within the fetus. A diagnostic test is given if a screening take a look at is constructive, to assess whether or not the disease is present or absent in the developing fetus. In addition, people of sure ethnic teams could be examined to detect whether or not they carry a gene for a specific dysfunction. First-Trimester Screening First-trimester screening tests are used to assess the danger of Down syndrome, trisomy 18, and trisomy 13 in a developing fetus. An benefit of first-trimester screening is that the exams are performed early enough so that decisions may be made relating to persevering with the being pregnant, if essential (Table 7. Detecting pregnancies at high risk for Down syndrome within the first trimester is of low utility if a diagnostic invasive take a look at. The risk of antagonistic being pregnant end result is proportional to the diploma of nuchal translucency enlargement. Measurement is taken of the lucent space within the posterior neck (calipers), with the posterior caliper placed just contained in the echogenic pores and skin (arrowhead). If an enlarged nuchal translucency, an apparent anomaly, or a cystic hygroma is identified on ultrasonography, the affected person must be provided genetic counseling and diagnostic testing for aneuploidy as properly as follow-up ultrasonography for fetal structural abnormalities. Given the excessive danger of congenital heart illness in these fetuses, referral for fetal cardiac ultrasonography should be thought-about. Patients with an enlarged nuchal translucency or cystic hygroma and regular fetal karyotype must be supplied an anatomic evaluation within the second trimester, fetal cardiac 204 ultrasonography, and additional counseling concerning the potential for genetic syndromes not detected by aneuploidy screening. The sensitivity and specificity for trisomies 21, 18, and 13, and intercourse chromosome aneuploidy are all larger than 90%. Second-Trimester Screening Second-trimester screening may be the solely choice if a woman is seen for the first time during the second trimester of her being pregnant. When these check results are interpreted independently, the false-positive rates are additive, leading to many more pointless invasive procedures (11%�17%). When the levels of all three markers (triple screen) are used to modify the maternal age-related Down syndrome risk, the detection fee for Down syndrome is roughly 70%; roughly 5% of all pregnancies will have a constructive screen result. Typically, the degrees of all three markers are lowered when the fetus has trisomy 18. Adding inhibin A to the triple screen (quadruple screen) improves the detection fee for Down syndrome to roughly 80%. Ultrasound Screening In the second trimester, gross abnormalities, corresponding to cardiac defects, in addition to a bunch of refined sonographic markers (soft markers), may be related to an elevated risk of Down syndrome in sure ladies (Box 7. Studies point out that the best detection rate is achieved with systematic combination of ultrasonographic markers and gross anomalies, similar to thick nuchal fold and cardiac defects. However, an irregular second-trimester ultrasound finding identifying a serious congenital anomaly considerably increases the chance of aneuploidy and warrants further counseling and the supply of a diagnostic process. Women with a optimistic screening check should obtain an ultrasound examination to detect identifiable causes of false-positive outcomes. The outcomes are reported only after both first-trimester and second-trimester screening tests are completed. Integrated screening supplies the very best sensitivity with the lowest false-positive price. The decrease false-positive fee leads to fewer invasive tests and, thus, fewer procedure-related losses of normal pregnancies. Another limitation of integrated screening is nonadherence of the second blood draw. Early prenatal genetic diagnosis additionally affords sufferers the choice to terminate affected pregnancies. Alternatively, a diagnosis of a genetic dysfunction could enable the patient to put together for the birth of an affected baby and, in some circumstances, may be essential in establishing a plan for care throughout pregnancy, labor, supply, and the quick neonatal period. In addition, individuals with sure ethnic backgrounds predisposed to genetic problems may endure carrier testing. Carrier screening and counseling ideally ought to be performed earlier than being pregnant as a result of this permits couples to find out about their reproductive danger and think about probably the most complete vary of reproductive choices. For example, the American College of Obstetricians and Gynecologists (College) recommends that people of Ashkenazi Jewish descent must be tested previous to pregnancy or early in pregnancy for Tay-Sachs illness, Canavan illness, cystic fibrosis, and familial dysautonomia. Genes responsible for many illnesses have been situated, and direct testing for the presence of a selected mutation may be carried out. Examples of illnesses for which direct checks exist are Tay-Sachs disease, hemophilia A, cystic fibrosis, sickle cell disease, Canavan disease, familial dysautonomia, and thalassemia.






