Evista

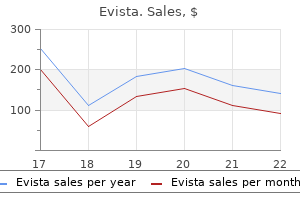
Evista
Evista dosages: 60 mg
Evista packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

During the neonatal interval and for about 1 yr afterwards women's health clinic evergreen park 60 mg evista cheap otc, the adrenals secrete androgens menstrual iron deficiency cheap evista 60 mg fast delivery. This restarts in midchildhood menstrual cramps 7 months pregnant 60 mg evista purchase with visa, round 7 years of age, at which period the zona reticularis produces androgens once more. From delivery through 6�12 months, there are pubertal ranges of luteinizing hormone; in boys, this ends in further testosterone production because of the high levels of luteinizing hormone stimulating the testes. Increased sebum production in the first few months returns to regular at about 6 months. Similar to neonatal acne, it could be related to elevated ranges of androgens produced by adrenal glands in each sexes and by the testes in boys. Associated ailments Prepubertal acne could additionally be associated with underlying endocrinopathies and virilizing tumours. Acne description Neonatal Infantile Midchildhood Preadolescent Adolescent Age of onset Birth to 4�6 weeks 6 weeks up to 1 12 months 1�7 years 7 years up to 12 years or menarche in girls 12 years as much as 19 years or after menarche in girls prepubertal acne 90. Environmental elements Certain medications may be implicated in prepubertal zits as recognized within the section on druginduced zits. Exposure to sure substances including greasy emollients, hair gels, occlusive topical brokers in addition to fragrant hydrocarbons and halogenides could additionally be a set off. Clinical features In the neonatal period, zits might current at start or shortly afterwards up to 28 days [753]. Infantile zits is alleged to be seen more rarely than neonatal zits however is usually misdiagnosed [754]. Neonatal zits typically presents after 6 months and most cases resolve by the age of 5 years however often some remain as a continuum until puberty [743]. Production of androgens from the neonatal adrenal glands ceases round 1 yr of life till the onset of adrenarche around the age of seven years. As outlined beforehand, causes of hyperandrogenism must be ruled out if zits presents in this age group. The growth of midfacial comedonal pimples is taken into account a predictor zits severity [745]. Acute onset, persistent or extreme zits particularly in the presence of virilization between 1 and 7 years of age ought to all the time elevate the potential for an underlying endocrinopathy. Infantile acne has been reported as an initial sign of an adrenocortical tumour in a 23monthold boy with accelerated progress and signs of virilization [746]. In boys, recalcitrant or extreme pimples could also be a presenting signal of nonclassical congenital adrenal hyperplasia [748]. A focused historical past and examination for signs of accelerated progress, precocious puberty and hirsutism or other indicators of hyperandrogenism ought to be employed. The central cheeks are frequently affected [754] with a combination of inflamed papules and pustules with open Predisposing elements See primary section on acne vulgaris. Causative organisms Propionibacterium acnes is implicated in the pathophysiology of acne (see section on the pathophysiology of acne vulgaris). In the case of neonatal cephalic pustulosis, a relationship has been advised between the medical presentation and Malasezzia furfur, Malasezzia sympodialis and different species [750] but not others [751]. A study of 29 patients with infantile/juvenile acne seen in a specialist centre over a period of 25 years [755] demonstrated the median age of onset was 9 months; the disease was delicate in 24%, reasonable in 62% and severe in 14%. Acne creating at an early age should always elevate the suspicion of androgen extra. Acne in prepubertal children normally presents with comedonal lesions with or without some inflammatory papules. Lesions are frequently located in a midfacial distribution and may precede some other indicators of maturation [756]. Clinical variants Neonatal cephalic pustulosis has been thought-about by some as synonymous with neonatal acne but others think about it a separate entity as there are extra inflammatory papules, significant pustules and an absence of comedonal lesions. Acne conglobata is a extreme variant of pimples that can current in infants resulting in extreme inflammatory cystic lesions, sinus tract formation and significant scarring [729]. Neonatal cephalic pustulosis was first described in 1991 [759] and historically referred to as neonatal acne [731]. It is characterized by erythematous papular/pustular lesions particularly on the cheeks but additionally on the chin, eyelids, neck and upper chest. It has been postulated that neonatal cephalic pustulosis develops in affiliation with Malassezia sympodialis and Malassezia globosa; nevertheless, the precise aetiological function of Malassezia is uncertain, as the organism is part of the conventional flora of neonatal skin, and as much as 38% of instances had negative smears in one examine [760]. Another explanation is that neonatal cephalic pustulosis pertains to an overgrowth of lipophilic yeasts at delivery that leads to an inflammatory response resulting in monomorphic papules and pustules in predisposed neonates with extra sebum production. If the situation does persist beyond this time and/or is widespread and unpleasant, topical ketoconazole cream expedites recovery [732,761]. The differential prognosis of childish zits contains neonatal zits, zits venenata infantum, chloracne and hyperandrogenism. The differential analysis of midchildhood acne contains keratosis pilaris and milia alongside endocrinopathies and situations regarding hyperandrogenism as outlined in Box 90. The differential diagnosis of prepubertal pimples contains childhood granulomatous periorifacial dermatitis, lupus miliaris disseminatus faciei and childhood granulomatous rosacea alongside endocrinopathies and problems related to an androgen extra as outlined in Box 90. Severity is assessed as mild, reasonable or severe and the persistence or appearance of scarring ought to be considered as a less beneficial prognostic elements. Investigations It is necessary to think about underlying endocrinopathies and investigate accordingly with the support of a paediatric endocrinologist (see Box 90. Complications and comorbidities Acne scarring can result from pimples lesions as in grownup zits. In one study analyzing instances of infantile acne, secondary scarring affected 17% of the cases [755]. Patients with childish acne may develop a resurgence of their acne as teenagers and the chance of growing pimples in adolescence is larger in these patients than of their friends [743]. Infantile acne may be very rarely associated with other medical features of androgen extra similar to hirsutism or premature closure of the epiphyses; very occasionally, there may be transient or extra persistent excessive plasma levels of testosterone, luteinizing hormone and folliclestimulating hormone. First line Neonatal zits: if lesions are causing concern or are extra average to severe in nature an strategy as outlined in Table ninety. Acne category Treatment options Neonatal Infantile Prepubertal Gentle cleaners, oilfree emollients If marked pustules topical azole cream First line Benzoyl peroxide or topical retinoid (if primarily comedonal) Fixed mixture products if mixed lesions all indicated from 12 years aside from zero. Infantile zits has a more persistent and variable course than neonatal pimples and although most cases resolve by 5 years of age others may persist till puberty. Patients with childish acne might develop a resurgence of their acne as teenagers and mother and father should be advised accordingly [729,732,743,755,763,764]. For gentle disease, topical therapies such as topical retinoids and/or topical antimicrobials are really helpful. Deep nodules could be injected with a low concentration of intralesional triamcinolone acetonide (2. Infantile zits may take a quantity of months to resolve � the extra inflammatory the disease, the longer the duration [755]. Successful treatment with isotretinoin has been reported within the literature using doses of zero. Given that using isotretinoin is an off license indication on this context, clinicians ought to ensure dad and mom are well knowledgeable if using oral isotretinoin for zits in this age group. Evidence based suggestions for the diagnosis and remedy of paediatric acne. However, there are reviews within the literature confirming the safe and profitable use of oral isotretinoin in sufferers ranging from 5 to 20 months of age. Administering capsules could be difficult in kids of this age, isotretinoin is extremely light sensitive and oxygen labile so splitting capsules may cut back potential efficacy if not conducted in dim light. Although mixing with meals has been advocated this will likely have an effect on the steadiness of the drug [767]. Freezing the capsule to a stable constituency allows it to be divided into halves or quarters to ship the desired dose. This prevents drug wastage, minimizes degradation of the drug and masks any unacceptable taste [756]. New insights into the administration of acne: an update from the Global Alliance to Improve Outcomes in Acne Group. An expert view on the therapy of zits with systemic antibiotics and/or oral isotretinoin in the light of the new European suggestions. Powell Charles Institute of Dermatology, University College Dublin, Dublin, Ireland Definition and nomenclature, ninety one.
Although warfarin necrosis might rarely contain acral areas women's health clinic perth evista 60 mg generic without prescription, acral cutaneous purpura in patients on warfarin is extra more doubtless to women's health center bowling green ohio evista 60 mg cheap without a prescription be because of womens health 50 ways to cook chicken buy evista 60 mg cheap cholesterol embolus � socalled purple (blue) toe syndrome. Warfarin necrosis is more prone to occur in areas with ample fatty subcutis, such because the breast, hip, buttocks and thigh [9,10]. The patterns of cutaneous haemorrhage for each of these completely different mechanisms are distinctive, and could be a information to pathophysiology and remedy [13]. Importantly, protein C and protein S are additionally vitamin Kdependent plasma factors, and their inhibition can result in a prothrombotic state. The time period purpura fulminans has subsequently been used for widespread cutaneous haemorrhage in patients with sepsis, including infection with Neisseria meningitidis, Staphylococcus aureus, groups A and B haemolytic streptococci, Streptococcus pneumoniae, Haemophilus influenzae and H. Disease course and prognosis In the absence of appropriate remedy, lesions invariably progress to fullthickness cutaneous necrosis. In a small study, early biopsy of retiform purpuric lesions confirmed microvascular occlusion with fibrin, and perivascular haemorrhage with minimal to no inflammation; these findings correlated with extreme protein C deficiency [12]. Protein C and activated protein C concentrates have been used for the remedy of each acute disease and as prophylaxis against subsequent episodes [14]. Although up to onethird of sufferers with warfarininduced pores and skin necrosis may have partial protein C deficiency, nearly all of cases seem unrelated to inherited deficiencies of protein C [10]. As warfarin motion mimics that of vitamin K deficiency, it would be expected that a depletion of vitamin K would result in warfarin necrosislike findings, however this has not been documented. Restoration of protein C exercise may be achieved by way of protein C concentrates, and presumably also by way of using activated protein C. Clinical options Presentation Retiform (stellate) purpura and necrosis is the most common cutaneous discovering that results from thrombosis inside the cutaneous microvasculature. Skin lesions typically start inside a quantity of hours Antiphospholipid antibody/lupus anticoagulant syndrome a hundred and one. Protein C concentrates and plasma change have additionally been successfully used to replace protein C in purpura fulminans [17,18]. Such antibodymediated dysfunction is troublesome to overcome by the alternative of factor, and concentrated sources of protein S are unavailable. Although thrombocytopenia Epidemiology Incidence and prevalence Antiphospholipid syndrome could occur as a major or secondary disorder. Age In a big examine the imply age was 42 � 14 years at examine entry, and the onset of signs was most frequently in younger to middleaged sufferers (2. Pathophysiology Predisposing elements Precipitating components embody infections, surgical procedures, medication and the discontinuation of anticoagulation. Infectionrelated antibodies, especially in leprosy, are extra often IgM than IgG kind. Investigations A number of serological markers exist, often detected as antibody towards phospholipids (especially cardiolipin) together with antigens from a cofactor molecule. The detection of antiphospholipid antibodies is roughly five instances more frequent than the detection of lupus anticoagulant [11]. Although prolongation of these checks would seem to predict an inclination in course of bleeding, individuals with lupus anticoagulant activity very not often bleed abnormally, however may be paradoxically predisposed to clot formation. Antiphospholipid antibody activity is detected by one of several antibody assays, the commonest being enzymelinked immunosorbent assay screens for IgG or IgM antibody affinity for cardiolipin, a negatively charged phospholipid molecule present in mitochondrial membranes. In one large study, the frequency of those findings was livedo reticularis 24%, leg ulcers 5. Antiplatelet therapy is of uncertain profit; most therapy is dependent upon acute and infrequently chronic anticoagulation, either with standard or lowmolecular weight heparin initially followed by warfarin [5]. Antimalarial remedy could also be of some profit for atrophie blanchelike or Degos like syndromes in lupus sufferers; proof suggests a protective effect in lupus sufferers against arterial or venous thromboses [1]. Livedo racemosa is usually the primary manifestation of Sneddon syndrome, initially affecting the decrease trunk and proximal a part of the legs, but turning into more generalized. Associated Raynaud phenomenon or acrocyanosis may occur, and will be the presenting function [1,2]. Pathophysiology the presence of antinuclear antibodies or of antiphospholipid antibodies/lupus anticoagulant has been reported [4], but some authors solely accept the prognosis of Sneddon syndrome if these antibodies are absent. Differences have been documented between the scientific features of sufferers with Sneddon syndrome depending on the presence or absence of antiphospholipid antibodies. Those with out antiphospholipid antibodies typically have a largersized livedo sample, whereas these with antiphospholipid antibodies have a better threat of seizures, mitral regurgitation and thrombocytopenia [5]. Initial changes are endothelial swelling with a mixed inflammatory infiltrate, progressing to vascular plugging, subendothelial proliferation and eventual vascular occlusion, fibrosis and disappearance of the inflammatory component [12]. It is possible, if not likely, that the histological findings in patients with antiphospholipid antibodies, particularly in association with lupus or lupuslike illness, can be more typical of noninflammatory occlusion. Clinical features Presentation In addition to the cutaneous livedo, there could also be nonspecific neurological prodromal symptoms similar to headache, migraine, dizziness or vertigo. Clinical variants the peripheral nerves can also be affected and hypertension may be current. Hypertension and the neurological aspects are generally aggravated by pregnancy or using oral contraceptives. There could additionally be renal or cardiac involvement, together with valve defects corresponding to mitral regurgitation, although inside organ involvement other than neurological is usually asymptomatic [3]. Differential prognosis the differential prognosis is wide, from both the cutaneous and the neurological perspective. In particular, other causes of livedo and microvascular occlusion syndromes mentioned on this chapter must be thought of in addition to vasculitic causes. Pathophysiology Disease course and prognosis Later neurological features embrace focal paresis or hemiparesis, focal sensory or hemisensory signs, suits and visual defects, and later cognitive modifications. Multiple pathophysiological abnormalities have been implicated, including platelet activation, issue V Leiden, altered fibrinolysis, antiphospholipid antibodies and hyperhomocystinaemia [1,2,3,4]. In one series of 32 sufferers, heterozygous factor V Leiden mutation was found in two of nine sufferers examined (22%), decreased protein C or protein S exercise in two of 15 (13%), prothrombin G20210A mutation in certainly one of 12 (8%), lupus anticoagulant in 5 of 28 (18%), anticardiolipin antibodies in eight of 29 (29%) and elevated homocysteine ranges in three of 21 (14%) [5]. Pathology the most characteristic histological findings in this syndrome are some thickening or hyaline adjustments in the walls of superficial dermal vessels, and luminal fibrin deposition [1,6]. Red cell extravasation and perivascular lymphocytic infiltrates are expected findings. In a collection of 45 pores and skin biopsies from 32 sufferers, all however one confirmed intraluminal thrombus and direct immunofluorescence was constructive in 86% [5]. Management There is usually no very efficient remedy, reflecting the non inflammatory nature of the disease. Corticosteroids could have some benefit but that is variable and infrequently troublesome to assess because of the intermittent nature of the neurological illness; other immunosuppressive brokers are often disappointing. The avoidance of smoking and oral contraceptives, and treatment of hypertension and hyperlipidaemia (both of which are generally present), are essential. Thrombolytic agents and vasodilators have been used in the acute scenario, and antiplatelet brokers seem to be efficient in the long term [5]. Clinical options Presentation Persistent, very painful and often punchedout ulcerations of the legs, especially around the malleoli, in girls are typical of atrophie blanche [6]. Healing results in a porcelainwhite scar, frequently surrounded by telangiectasia. Besides venous hypertension and antiphospholipid antibodyrelated syndromes, sickle cell ulcers can show the identical porcelainwhite scar of atrophie blanche. Introduction and general description this syndrome is common as both an idiopathic or secondary syndrome [1]. Management Antiplatelet, anticoagulant and fibrinolytic therapies have been reported to be helpful on this syndrome, as nicely as anabolic steroids similar to danazol and stanozolol [2]. In patients with lupus and atrophie blanchelike lesions, antimalarial remedy may be effective. Rapid reduction of pain has been reported with the utilization of intravenous immunoglobulins [8], postulated to be due to inhibition of the vasoconstrictor chemical compounds thromboxane A2 and endothelin which thereby improves perfusion. Lipoprostaglandin E1 has been used with good response in a patient with livedoid vasculitis and essential cryoglobulinaemia [9], however this will likely have been mediated by an effect on the cryoprotein ranges, which fell dramatically. There are anecdotal stories of response to tetracyclines [10], and Epidemiology Age this syndrome is commonest in younger to middleaged girls.
Syndromes
Patients present with a mixture of a number of or all of the following inside a single limb: limb size hypertrophy of muscle menopause joint pain order evista 60 mg visa, fat or bone womens health 022013 cheap evista 60 mg fast delivery. The underlying mechanism is assumed to be of somatic mosaicism pregnancy 8 weeks 5 days evista 60 mg purchase amex, and no recognized causal genes have been recognized to date. Swelling sometimes impacts all body elements and sometimes presents in utero with hydrops fetalis. Proteus syndrome is a disease characterized by progressive, segmental overgrowth of the bones, skin and connective tissue. Lymphatic and capillary malformations are the most common vascular changes seen in this syndrome. The analysis could additionally be established utilizing diagnostic scientific standards and/ or molecular analysis [28]. Patients with congenital multisegmental lymphoedema with out systemic lymphatic impairment have been included throughout the yellow part of the classification pathway so as to keep away from confusion with multisegmental lymphoedema occurring in association with systemic lymphatic abnormalities (in the pink section of the pathway). These sufferers have an asymmetrical pattern of lymphatic failure with some limb sparing. It is feasible that somatic mosaicism in gene(s) concerned in lymphangiogenesis could explain this subtype of congenital main lymphoedema. These sufferers have extensive, asymmetrical, multisegmental lymphoedema comprising facial and conjunctival oedema, genital lymphoedema, and epidermal naevi and/or capillary malformations typically of the torso and higher limbs. These sufferers have a sporadic situation, suggesting probable somatic mosaicism [10]. Lymphoscintigraphy in Milroy illness confirms failure of the preliminary lymphatic vessels to take in fluid. The initial lymphatic vessels are current (confirmed on histological examination) however unable to absorb interstitial fluid [33]. Affected individuals usually have all of the medical signs of Milroy illness (congenital lower limb lymphoedema, distinguished largecalibre veins and hydroceles, inherited in an autosomal dominant pattern) but their lymph scans are atypical. The presence of chorioretinopathy is variable but ought to all the time be excluded by an expert ophthalmology opinion. Lymphoscintigraphy demonstrates the identical sample of lymphatic practical aplasia as that seen in Milroy disease. Congenitalonset main lymphoedema Historically, all cases of congenital lymphoedema were categorised as Milroy illness. However, several various varieties of congenital lower limb main lymphoedema have been acknowledged. Milroy disease presents with congenital lymphoedema of the decrease legs (usually symmetrical). The onset of swelling could often be delayed however will occur inside the first yr of life. Lymphoedema is usually confined to the feet and ankles, but could progress as much as the knees. Prominent largecalibre veins are frequently present on the feet and pretibial regions. Milroy illness not often presents in the antenatal Lateonset primary lymphoedema the time period lateonset lymphoedema is used to describe a primary lymphoedema that develops after the first yr of life. This section accommodates numerous assorted conditions, some with lifethreatening related diseases. Emberger syndrome), but they all share the frequent discovering of noncongenital limb swelling. Distichiasis (aberrant eyelashes arising from the meibomian glands) is present in 95% of affected individuals and is regularly current at start however rarely causes signs until childhood [40]. Lymphoscintigraphy of affected individuals demonstrates reflux of lymph throughout the decrease limbs as a outcome of valve failure throughout the lymphatic vessels [43]. It typically presents with bilateral lower limb lymphoedema that rarely extends above the knee. Lymphoscintigraphy regularly demonstrates irregular deep rerouting of decrease limb lymph drainage as evidenced by an elevated uptake of tracer throughout the popliteal lymph nodes and impaired main superficial lymphatic tract filling [10]. Family history is in preserving with an autosomal dominant pattern of inheritance yet the causal gene of basic Meige illness has not but been identified. Emberger syndrome includes lateonset (but in childhood) bilateral or unilateral decrease limb with or with out genital lymphoedema together with myelodysplastic syndrome and/or acute myeloid leukaemia [46]. It may also be associated with a highfrequency, progressive sensorineural deafness. Myelodysplasia could develop at any stage and can progress to acute myeloid leukaemia with a high mortality [47]. Lymphoscintigraphy has not been routinely performed on patients with this situation. Mouse studies suggest the lymphoedema occurs because of irregular lymphatic valve growth [50]. Apart from decrease limb varicose veins, no different related conditions have been reported. Lymphoscintigraphy demonstrates lymphatic tracts that seem regular but with considerably decreased quantification uptake of tracer, reflecting lowered absorption from tissues by peripheral lymphatics in all four limbs [52]. A detailed history, examination (and potential investigation with lymphoscintigraphy or venous duplex imaging) ought to provide the underlying analysis. Classification of severity the severity of the lymphoedema could also be categorised based on the medical features (Table 105. Complications and comorbidities See the part called Complications of lymphoedema later in this chapter. Lipoedema Definition and nomenclature Lipoedema is a dysfunction of adipose tissue that occurs virtually exclusively in ladies, usually at a time of hormonal change. Patients have progressive fatty swelling of the decrease limbs, with associated easy bruising, skin tenderness and ache of the decrease limbs. Synonyms and inclusions � Adiposis dolorosa � Painful fat syndrome � Adipositas oedematosa � Stovepipe legs Differential analysis Secondary lymphoedema that has occurred because of an underlying medical cause needs to be excluded, for example lower limb Lipoedema a hundred and five. It occurs almost solely in females, and is believed to be an inherited disorder. The onset of signs typically occurs at a time of hormonal change similar to puberty or pregnancy. Patients complain of progressive fatty swelling of the lower limbs, with associated easy bruising, skin tenderness and ache of the lower limbs. The lack of a transparent definition of the disorder has led to significant confusion regarding analysis and management. In reality, some clinicians consider it a physiological variant quite than a illness [2]. Genetics Frequent observations of mother to daughter inheritance led to the speculation that lipoedema is a genetic disorder. Patterns of inheritance of the situation within families are consistent with both Xlinked dominant inheritance or autosomal dominant inheritance with intercourse limitation [7]. Patients frequently complain of tenderness and straightforward bruising of the affected areas. The onset of lipoedema is usually at or soon after puberty but can appear to develop at other occasions of hormonal change such as being pregnant and even menopause [7]. Age Onset is usually at puberty or different times of hormonal change such as pregnancy or commencement of the oral contraceptive capsule. Only six cases of lipoedema affecting males have been reported within the literature [7,eight,9]. All have been thought to have developed lipoedema secondary to hormonal disturbances, with decreased testosterone levels being a typical issue [7]. Presentation In the teenager or young adult the lipoedema phenotype is attribute; the basic disproportionate distribution of fat beneath the waist, the coexisting options of tissue tenderness and simple bruising and the dearth of response to weightreducing diets all argue towards a form of weight problems. However, later in life, lipoedema may be sophisticated by weight problems and/or lymphoedema, rendering the prognosis more difficult to make. Whilst lipoedema is confused with obesity by many clinicians, associated weight problems has, nonetheless, been observed in 50% of patients [12]. However, lymphoedema usually results in asymmetrical oedematous swelling as a end result of the accumulation of interstitial fluid inside tissue areas.

This is matched by the resistance of trichocyte keratins to dissolution in robust solvent pregnancy ultrasounds buy cheap evista 60 mg line. Keratin distribution within the nail and related epithelium has been studied in adult [14 womens health specialists appleton wi evista 60 mg purchase without a prescription,15 menstrual ulcers 60 mg evista generic overnight delivery,16], infant [17] and embryonic [32] digits. Immunohistochemistry of the epithelial buildings of the traditional nail demonstrates that the suprabasal keratin pair K1/K10 is found on each features of the proximal nail fold and to a lesser diploma in the matrix. The nail mattress accommodates keratin synthesized in normal basal layer epithelium, K5/ K14, which can additionally be present in nail matrix. An antibody marking the epitope characteristically related to keratin expressed in the basal layer is discovered all through the thickness of the nail mattress, however only basally in the matrix [26]. The nail mattress has very low charges of proliferation [10,33], and it could be that K6/K16 extra precisely illustrates a lack of differentiation, usually associated with proliferation in pores and skin but representing the resting state of nail bed epithelium. The location of K6/K16 is mirrored in the localization of the options of pachyonychia congenita. Trichocyte keratins 31, 34, eighty one, eighty five and 86 have all been demonstrated immunohistochemically in the nail unit [15,16]. Their distribution appears to define a matrix according to the basic description of the germinal matrix. Distal subungual arcade Proximal subungual artery (arcade) Superficial arcade Digital artery figure ninety five. In the occasion of injury to the main provide in the pulp space, such as might happen with an infection or scleroderma, there could also be enough blood from the accent vessels to permit normal growth of the nail. The axis becomes more longitudinal in the nail bed with out the tortuosity � a sample that can also be seen within the distal proximal nail fold. Nail vessel videomicroscopy can be used as a part of a dynamic and anatomical modelling course of establishing the parameters of blood circulate and vessel anatomy [4]. There are many arteriovenous anastomoses beneath the nail � glomus our bodies � which are involved with heat regulation. Glomus bodies are necessary in sustaining acral circulation underneath cold situations: arterioles constrict with chilly but glomus bodies dilate [5]. These occupy the subdermal tissues and enhance in number in a gradient towards the distal nail bed [6]. In this respect, it differs from most hair follicles, which bear periods of quiescence as part of the follicular cycle. Blood provide [1] There is a wealthy arterial blood supply to the nail mattress and matrix derived from paired digital arteries, a large palmar and small dorsal digital artery on either side. The palmar arteries are equipped from the large superficial and deep palmar arcades [2]. Distally, the arteries are extraordinarily tortuous and coiled, which allows them to be distorted with out kinking to occlude provide. There are two primary arterial arches (proximal and distal) supplying the nail mattress and Cell kinetics the kinetic exercise of the matrix has been examined using many techniques. These embrace immunohistochemistry, autoradiography and direct measurement of matrix product. The matrix can also be the location of maximal inclusion of tritiated thymidine Nail indicators and their significance ninety five. These combined components make psoriasis the most typical pathology by which upgrowing nails are seen. In this condition, the nail matrix might turn out to be bucketshaped and the impact of the overlying proximal nail fold is misplaced. Although there was some inclusion of thymidine into the nail mattress, Zaias and Alvarez [3] interpreted the findings as indicating that the nail mattress had no position in the creation of the nail plate. Norton [4] drew a similar conclusion from work with reside human subjects the place labelled thymidine and glycine had been injected locally to act as markers of proliferating and metabolically lively keratinocytes, and each primarily labelled the matrix. However, the sooner work of Lewis [5] suggested on histological grounds that the nail plate is a trilaminar structure originating from three separate matrix zones: the dorsal matrix (ventral aspect of proximal nail fold), intermediate matrix (germinal matrix) and ventral matrix (nail bed). This challenges the interpretation that nail thickens over the nail mattress due to a contribution from underlying structures. An various rationalization may be applicable, corresponding to compaction arising from repetitive distal trauma. Others have also debated this issue [8] and, although the nail bed could have a major contribution to make in disease [9], the proof for its contribution at different occasions is conflicting. Linear nail progress [17,18,19] During the 20th century, many studies were carried out on the linear development of the nail plate in well being and disease; these have been reviewed [20,21] and are listed in Tables 95. However, research on nail progress in psoriasis, and its inhibition by cytostatic drugs [23,24], recommend that cell kinetics and linear growth price do have a direct correlation. Fingernails develop roughly 1 cm every 3 months and toenails at onethird of this rate. Several factors in all probability combine to produce a comparatively flat nail plate: the orientation of the matrix rete pegs and papillae; adherence to the nail mattress; the course of cell differentiation [15]; and moulding of the direction of nail development between the proximal nail fold and distal phalanx [16]. Containment laterally throughout the lateral nail folds assists this orientation, and the adherent nature of the nail mattress is prone to be necessary. Other factors corresponding to bradykinin and serotonin or reactive elements related to hypoxia may have relevance. The listing of diseases associated with clubbing has a pattern where chronic irritation of the bowel and lung are seen with or with out precipitating infection. Vascular causes could be related to central cyanotic ischaemia, as in coronary heart disease, or native factors such because the unilateral softtissue modifications of hemiplegia [11]. An isolated subungual tumour located inside the midproximal zone of the subungual space can displace the nail unit upwards in a kind just like clubbing. However, a few of the different features are typically lacking, such as the fluctuant high quality of the proximal nail and nail fold [12]. This can be included within the category of pseudoclubbing which arises from local pathology corresponding to osteolysis of the tip of the digit seen in systemic sclerosis. The secondary kind has many of the identical benign associations as isolated digital clubbing but is much more strongly associated with malignancy, notably bronchial carcinoma. In mechanics, softening of the nail from contact with oil may be a factor [5], and in hairdressers, permanent wave options could also be causal [6]. Fingers and toes could also be affected, with indicators most distinguished in the thumb or great toe. Koilonychia is widespread in infancy as a benign function of the great toenail, although in some infants its persistence could additionally be associated with a deficiency of cysteinerich keratin [2] in trichothiodystrophy. The most common systemic association is with iron deficiency [3] and haemochromatosis, although nearly all of adults with koilonychia reveal a familial sample, which can be autosomal dominant [4]. In dermatoses such as psoriasis and dermatophyte an infection, nail mattress hyperkeratosis could push the determine ninety five. In this occasion, cautious imaging and surgical exploration ought to be undertaken to exclude an isolated spaceoccupying lesion beneath the matrix [4,5,6]. Pain might come up as a result of embedding of the pincer nail in the lateral nail folds and nail bed, which becomes most pronounced distally. This will sometimes lead to a shift of the nail such that the opposite aspect not embeds. The alternative of corrective surgical procedure in toes has less chance of success, although profitable case series are reported. When treating the thumbs or fingers, the prospect of success with corrective surgery is higher and the cosmetic and functional handicap of ablation will not be acceptable. Again, a lateral ablation may be adequate, however more advanced procedures entail altering the alignment of the matrix [2,7,8], degree of the nail mattress [9] and addressing any midline hypertrophy of the distal phalanx. Nail braces hardly ever produce longterm benefit, though promising outcomes have been reported [11]. This can come up by way of burns, surgery or trauma, or be as a result of inflammatory dermatoses such as lichen planus where the entire nail matrix is scarred and misplaced [4]. This can happen because of an intense physiological or native inflammatory process, within the absence of scarring. This may mirror local or systemic disease and in the latter might result in temporary loss of all nails. In the long run, athletes often develop thickened dystrophic nails matching a historical past of recurrent shedding. More severe trauma may find yourself in a degloving event removing all tissue from the tip of the phalanx. The underlying genetic abnormality of the congenital kind has just lately been identified as a mutation within the Rspondin4, Frizzled6 or Wnt10a genes (see above: nail biology), which play an element in Wnt signalling within the cell [2]. There could additionally be a biological interplay with the underlying phalanx in embryogenesis (see Chapter 69) [3].
In youngsters women's health issues after 50 evista 60 mg purchase otc, potent systemic steroid therapy places them at danger of premature closure of the phalangeal epiphyses and prolonged courses should be administered with the collaboration of a paediatrician breast cancer uggs boots purchase 60 mg evista with amex. Oral steroids at up to menopause weight loss 60 mg evista discount free shipping 60 mg/ day have been used to arrest severe scarring nail lichen planus [2]. There are reviews of average success within the therapy of severe disease in youngsters with systemic brokers including oral prednisolone, dapsone and acitretin normally combined with topical remedy [19]. Ciclosporin may also be of benefit and azathioprine has been used to good impact in erosive disease [20]. Methotrexate is talked about in review articles [21] and alitretinoin [22] in case reviews. In one series of seven youngsters, two wanted surgery because of painful persistence of the issue [4]. The changes related to congenital malalignment of the good toe may subside within 5�10 years in about 50% of youngsters. Normal surface markings of the nail can differ in children from those seen in adults. A herringbone pattern is frequent and steadily diminishes with time [9], which may reflect a gradual change in the pattern of matrix maturation. Elastic tissue adjustments diffusely affecting the nail bed epidermis are sometimes seen histologically. The whole subungual area in old age could show thickening of blood vessel partitions with vascular elastic tissue fragmentation [11]. The nail plate turns into paler, uninteresting and opaque with advancing years, and white nails similar to those seen in cirrhosis, uraemia and hypoalbuminaemia could additionally be seen in normal topics. For particulars of the common traumatic abnormalities and adjustments due to insufficient pedicure or neglect, detailed texts should be consulted [1,12]. Onychomycosis is certainly one of the most typical nail illnesses of the elderly, and is commonly combined with a component of traumatic dystrophy that may predispose to relapse after therapy. There are considerations that drug interactions on this group would possibly make systemic remedy a poor selection [15]. But the examine additionally revealed that full remedy at the conclusion of the trial occurred in only 28% of circumstances, an element which should be considered earlier than instigating remedy [16]. Under the age of 5 years, nails are additionally susceptible to terminal onychoschizia (lamellar splitting). In a extra gross kind, this will present as congenital hypertrophic lip of the hallux, the place soft tissue overgrowth could resemble fibrous tumours of the digit before spontaneously disappearing [3]. It can, nevertheless, be helpful in identifying a spread of pathologies including underlying exostoses, bone determine ninety five. Exposure to vapours of synthetic supplies used within the production of different plastic merchandise may occasionally produce related abnormalities. If publicity is eliminated, therapeutic might occur with coalescence of phalangeal fragments leading to a pseudoclubbing, the thumb being more generally affected than different digits. Pincer nail deformity or trauma, including nail biting, can be related to radiologically detectable osteomyelitis. Benign spaceoccupying lesions might compress the underlying bone with corresponding upward convexity in the nail. Chondroid tumours could additionally be situated externally to the bone, but could also be detected by Xray as a lucency inside the bone. Similarly, Xray might reveal bony invasion by locally invasive or metastatic malignancy: in invasive subungual squamous cell carcinoma, as much as 55% of patients will have radiological evidence of involvement of the underlying phalanx. When present, acro-osteolysis is sort of definitely secondary to vascular compromise. Bony erosions of the phalanges occur in 40�80% of patients with systemic sclerosis. The presence of sclerodactyly and/or calcinosis cutis helps indicate the proper prognosis. In acronecrosis, the ultimate stage of acro-osteolysis, the gentle tissues within the fingertip telescope around the shortened tuft leading to pseudoclubbing. Radiographs are poor at differentiating longitudinal from transverse acro-osteolysis [1]. Investigation of the trigger is predicated more on scientific and laboratory information than on imaging. Occupational acro-osteolysis Workers involved in the polymerization of vinyl chloride have developed acro-osteolysis. Phalangeal microgeodic syndrome is an unusual benign situation firstly described by Maroteaux in 1970 [3]. Clinical manifestations embrace swelling and redness of a number of phalanges of 1 or both arms. Radiological signs embody multiple small osteolytic areas and sclerosis suitable with acro-osteolysis. A relation to cold exposure has been suggested since patients often current this during the colder months of the yr [4]. Acro-osteolysis has been reported in young guitar players [5] most likely related to persistent mechanical injury resulting in vascular compromise and avascular necrosis. The earliest radiological sign of this illness is cortical resorption of the phalangeal tuft [6]. Softtissue haemangiomas are extra widespread and may manifest as native softtissue masses, localized bony overgrowth, phleboliths within the soft tissue and pressure erosion of the underlying bone. This hamartoma of hypertrophied elements of the traditional glomus physique is normally a wellencapsulated, gentle pink or purple mass, smaller than 1 cm in diameter. Mathis and Schulz [7] reviewed 15 such tumours on the digit and found that 9 had characteristic changes of bony erosion. This was smooth and concave typically, however occasionally had a punchedout look on the phalangeal tuft. Bony destruction of the distal phalanx is current in virtually all cases of subungual keratoacanthoma and could also be seen on radiographs even when examined shortly after medical presentation. The destruction is characteristically welldefined, clean, circular and limited to the tip of the phalanx [9]. The machines are capable of detecting the blood circulate of the nail mattress in actual time. The nail unit is comprised of three main areas: the nail plate, the nail mattress and the paronychial tissues. The dorsal and ventral plates current a bilaminar hyperechoic structure (two parallel lines) separated by a very thin hypoechoic layer (interplate space). The distal insertion of the lateral bands of the extensor tendon in the distal phalanx shows a fibrillar hyperechoic pattern, typical of tendinous buildings. Images reflecting the different layers may be either horizontal or vertical (similar to ultrasound). Functional elements corresponding to speckle variation and vascular circulate may be included in some tools. The axial resolution is <5 and lateral decision <7 m; the scanning depth is up to 2 mm, limiting its use to very superficial tissues. It has been widely investigated in dermatology, particularly in non-melanoma skin cancers. It is a small welldefined cystic lucency within the phalanx, generally having scalloped margins or a sclerotic rim, and is mostly located centrally in the bone. In the distal phalanx, the enchondroma is typically situated at the base of the phalanx, abutting the articular surface. Aneurysmal bone cysts and large cell tumours hardly ever occur within the distal phalanges. Both could have related radiological features characterized by lytic expansive lesions involving the whole phalanx [11]. The nail plate can be scanned from the floor to the lower half adjacent to the underlying nail mattress. The superficial layer exhibits a brighter reflection, adopted by a zone with a poorer sign, followed again by a brighter zone within the deepest part. Two main functions have involved dermatologists so far as follows: 1 Confocal microscopy and onychomycosis. T1weighted sequence permits morphological evaluation of lesion contour and anatomical extent; T2weighted sequence defines tissue characterization from signal intensity emitted by the tumour; gadolinium highlights the vascularization of tumours and should improve definition of lesion contours. The indicators obtained within the various sequences are attribute and can distinguish the most common tumours encountered in the nail area.
Lichen simplex Part 10: websites womens health partners st louis cheap evista 60 mg overnight delivery, intercourse pregnancy 70 effaced discount 60 mg evista, age Lichen simplex is common across the male genitalia womens health las vegas 60 mg evista purchase. Giant forms (of Pautrier) occur, giving a Allergic contact dermatitis the dangers of allergic contact dermatitis of the genital pores and skin come about from: (i) direct contact with the allergen. Eczematous symptomatology can appear roughly 1 week after first contact with the allergen if previously unsensitized, or inside a few hours if already allergic. More instant symptoma tology and acute erythema and angiooedema counsel a contact urticaria, which might happen with some of the rubber constituents of condoms and gloves [4,5,eleven,12,thirteen,14]. Allergy to methylisothiozolinone, an ubiquitous preservative, is becoming an typically reported phenomenon [6,15]. Latex allergy could additionally be an issue in sufferers with spinal wire harm using rubber merchandise for the handle ment of urinary difficulties; lifethreatening anaphylactic reactions have occurred [20]. Condoms made from lamb caecum are avail ready for rubberallergic patients, however they could provide much less pro tection towards sexually transmitted disease than latex. Creating hypoallergenic condoms by washing in an ammonium resolution to take away the residues of the accelerator chemicals that actually cause the hypersensitivity has proved unsuccessful [21]. Celandine juice [10] and clothing dye dermatitis of the scrotum [22] have been reported. There could also be clues to these components at presentation but subsequent patch testing is usually required. Allergic contact dermatitis can persist even after withdrawal of the set off allergen. Management is in any other case as for irritant contact dermati tis, lichen simplex and pruritus ani. Treatment of male genital lichen simplex follows the lines of administration relating to irritants, with emphasis on the aid of scratching, soap substitution and moisturization, and occlusion of the world if potential with a bland dressing � moist if the skin is fiercely eczematized. A potent topical corticosteroid ointment can be utilized for a quantity of days after which tailed off. Preparations containing tar or mixtures of antibacterial, anticandidal and antifungal agents are additionally useful. Two circumstances of intensive big lichen simplex of the scrotum have been successfully treated by hemiscrotectomy [1,9,23]. Management of irritant dermatitis follows strains just like these for pruritus ani. Topical corticosteroid ointments, with or with out antibiotic and anticandidal agents, are employed to con trol the dermatitis. Topical native anaesthetics should be prevented because of the chance of sensitization. Occasionally, secondary infection may be severe; a swab must be taken and oral antibiotics and oral antifungals prescribed. A extra acute image (itch, burning or ache, swelling, erythema, vesiculation) may happen if extremely irritant chemicals in excessive con centration are by chance or deliberately used on the genitalia. Treatment is with potassium permanganate soaks, very potent topical corticosteroid lotions (sometimes systemic corticosteroids) and systemic antibiotics. In the persistent state, there could also be pruritus together with the typical poikilo derma. Radiotherapy has been used for the therapy of numer ous anogenital dermatoses through the years, together with Bowen illness, erythroplasia of Queyrat, squamous carcinoma, psoria sis, Peyronie illness and pruritus ani [8,22]. Radiotherapy con fers a longterm increased danger of pores and skin most cancers, particularly basal cell carcinoma. There is concern that radiotherapy for Bowen disease or erythroplasia of Queyrat may increase the subsequent threat of invasive carcinoma. Seborrhoeic dermatitis Genital involvement is frequent with this common dermatosis. A good his tory (including family history) and cautious examination of other sites typically affected assist the prognosis. On the scalp, the face, within the flexures and at anogenital websites seborrhoeic dermatitis and psoriasis may be indistinguishable. However, therapies that diminish the Malassezia load and reduce irritation and eczematization can be success fully and safely used long term. These embrace topical antifungals (such as clioquinol, nystatin and imidazoles) as ointments, lotions, lotions or shampoos, and mixtures of the same agents with gentle and moderately potent topical corticosteroids used alongside emollients and soap substitutes. The evidence suggests that Zoon balanitis is a chronic, reactive, principally irritant dermatosis caused by a dysfunctional prepuce. Although vegetative and nodular presentations have been recorded, atypical or uncommon morphology should be seen with great suspicion and biopsied [7,8]. Differential prognosis the differential analysis includes lichen sclerosus, erosive lichen planus, psoriasis, seborrhoeic dermatitis, contact dermatitis, fixed drug eruption, secondary syphilis, histoplasmosis [13], erythro plasia of Queyrat [14] and Kaposi sarcoma. In other words, the signs of Zoon balanitis may be sec ondary to underlying preputial illness [8]. It is likely that a variety of the medical and histological variants that have been reported [16�18], and a current declare that Zoon balanitis per se is a premalignant situation in a single case report [19], are a consequence of this phenomenon. Zoon balanitis indicates a dysfunctional foreskin Pathology the traditional histology is of epidermal attenuation with absent gran ular and sexy layers, and diamond or lozengeshaped basal cell keratinocytes with sparse dyskeratosis and spongiosis. Extravasated erythrocytes, haemosiderin and vascular prolifera tion are additionally seen. Although Zoon stressed the presence of the plasma cell infiltrate on this condition, the plasma cell numbers can be very variable [7,8,11]. Clinical features the presentation is classically indolent and asymptomatic, though staining of the underwear with blood has been reported [12]. Most sufferers recognized with Zoons balanoposthitis probably have clinically subtler underlying lichen sclerosus. Case stories concerning the usage of topical calcineurin inhibitors have appeared [20,21,22] but these brokers should be used with circumspection in the setting of a dysfunctional foreskin and the attendant threat of penis cancer, long run. Again, the pathologist should be requested to look at the entire specimen for indicators of one other underlying dermatosis. Lichen sclerosus definition and nomenclature Lichen sclerosus is a standard inflammatory dermatosis with a predilection for anogenital skin. The presence of the histopathological features of lichen sclerosus in a share of acrochordons (skin tags) suggests that occlusion of flaccid pores and skin is a pathogenic factor [37]. All the proof factors to male genital lichen sclerosus being as a end result of chronic occluded publicity of sus ceptible epithelium to urine [1,38�40,41]. Nuclear magnetic resonance spectroscopy of urine has not recognized a single culpable chemical constituent of urine [43]. Introduction and basic description Lichen sclerosus is a typical dermatosis of the penis. The diag nosis and administration of lichen sclerosus is a frequent purpose for sufferers to be referred to a male genital dermatology clinic. Sometimes, lichen sclerosus could additionally be tough to differentiate from lichen planus, and standards to assist, within the vulva, have been proposed by Fung and LeBoit [47]. In adults, anogenital lichen sclerosus is claimed to be about 10 instances extra frequent in girls than men. Lichen sclerosus may be much more frequent than is mostly supposed in younger boys, being identified histologi cally in 14�95% of prepuces removed for phimosis [3,4]. Clinical features the development of secondary phimosis in schoolage boys is extremely suggestive of lichen sclerosus [14]. In the older male, persistent major phimosis or the secondary development of phimosis in a beforehand retractable foreskin may be related to lichen sclerosus [9]. Lichen sclerosus of the penis may be asympto matic, but numerous, generally imprecise, symptomatology is usually encountered at rest or during or after sexual congress. Patients might describe itching, burning, bleeding, tearing, splitting, rash, Pathophysiology the aetiopathogenesis of male genital lichen sclerosus has turn out to be clearer in recent years. A credible unifying mechanism must clarify key scientific options and the results of prior investigative analysis: the predilection for the genitalia usually and in males, the uncircumcised [1,5]; the rarity of perianal involvement in men in contrast with women [1]; the inconsistent association with organspecific autoimmune illness [1,6,7�13] and atopy [14]; an Part 10: sites, intercourse, age 111. Predomi nant purpura, angiokeratomas, bullae, erosions and ulceration could additionally be encountered.
Indian Aloe (Aloe). Evista.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96602

While earlier reviews advocated early and extensive native excision to forestall intensive lipomatous infiltration [2 women's health center hagerstown md 60 mg evista purchase with amex,9] breast cancer quotes and sayings order 60 mg evista free shipping, more modern literature favours delayed resection with temporizing measures corresponding to liposuction women's health clinic gympie evista 60 mg, excision of mucosal neuromas and surgery to the upper lip to restore facial symmetry [13]. It has additionally been conjectured that growth hormone might play a job in recurrences, implying that mass discount attempts prior to the end of adolescence may be more more probably to fail [13]. Conditions inflicting contralateral hypoplasia, similar to hemifacial microsomia and progressive hemifacial atrophy (Romberg syndrome) must be excluded [20]. Other disorders of fats tissue infiltration corresponding to liposarcoma or lipoblastomatosis could additionally be dominated out primarily based on histological findings [15,16]. It is related to profound mental retardation, early onset of seizures, unilateral temporofrontal lipomatosis, ipsilateral cerebral and leptomeningeal lipomatosis, cerebral malformation and calcification, and lipomas of the cranium, eye and heart [1,2]. The hallmark pores and skin finding is naevus psiloliparus, a fatty hamartomatous malformation, of the scalp [3]. Incidence and prevalence Encephalocraniocutaneous lipomatosis is a rare disorder with about 60 instances reported within the English literature. The resection is nearly at all times subtotal because of the Age Cutaneous and eye findings are normally present at or shortly after delivery. Complications and comorbidities Complications and comorbidities rely upon the extent of organ system involvement. Pathology the histopathology of naevus psiloliparus exhibits focal dermal fibrosis with subcutaneous fats within the reticular dermis. Naevus psiloliparus of the scalp is the most common pores and skin finding and was present in 44/54 patients studied [6]. Patchy or linear alopecia which is typically nonscarring is usually noticed: it could comply with the traces of Blaschko or sometimes be scarring. Fibromas, lipomas and fibrolipomas current usually as ipsilateral pores and skin taglike cutaneous polyps on the eyelid or following a line from the outer canthus to the tragus. Less frequent cutaneous manifestations embody irregular or disrupted eyebrows and caf�aulait macules [6]. Choristomas, with or with out other eye anomalies, had been noticed in 43/54 patients [6] however other ocular abnormalities may be seen. Brain anomalies primarily involve the tissue surrounding the brain together with blood vessels [4]. Intracranial lipomas are probably the most outstanding function; different options embrace meningeal and meningovascular anomalies and spinal cord lipomas, which can be in depth. Less commonly, skeletal system involvement with jaw tumours or lytic bone lesions may be present; these could also be progressive [5,7�10]. Lipoedema of the lower limbs Definition Lipoedema is characterised by progressive, symmetrical and bilateral enlargement of involved areas because of subcutaneous deposition of fats. Imaging studies verify that oedema is minimal and the swelling is actually as a end result of homogenous enlargement of the subcutaneous compartment [3�8]. It is probably underreported and infrequently misdiagnosed because of unfamiliarity with this disorder [9,10,11,12]. In lymphoedema clinics, up to 15% of referred patients had been recognized with lipoedema [13,14]. Differential prognosis this contains the Proteus syndrome, oculoectodermal syndrome, oculocerebrocutaneous syndrome and epidermal naevus syndrome [11�15]. In the overwhelming majority of circumstances it affects the lower extremities however it may additionally have an result on the upper extremities and the scalp. Hereafter the term lipoedema, if unqualified, shall be used to denote lipoedema of the decrease limbs. However, it could also develop throughout other durations of hormonal modifications corresponding to pregnancy or menopause [24]. Enlargement of the decrease extremities is disproportionate in relation to the trunk, higher extremities, face and neck [15], even amongst obese patients [2,13]. The only signal throughout early levels of disease could be the disappearance of the retromalleolar sulcus. As the disease progress, this attribute bodily signal becomes more distinguished. If the upper extremities are affected, a similar cuff sign that ends sharply above the wrists is seen with sparing of the arms [15]. Although the non to minimal pitting oedema component is mild initially, distinguished oedema could finally develop [15]. Patients typically complain of heaviness and discomfort of the concerned areas with sensitivity to strain. One group of investigators found elevated plasma lipids as nicely as an abnormal fatty acid composition of tissue triglycerides in lipoedema sufferers relative to controls. Hormones appear to play a role within the growth of lipoedema, given that it happens almost exclusively in women with a typical onset close to puberty or during times of great hormonal modifications [1,2,9,16]. Moreover, male lipoedema circumstances occurred in these receiving hormonal therapy for prostate carcinoma or with hepatic cirrhosis [12,20]. The anatomy of the lymphatic vessel system in lipoedema sufferers has been found to be regular or enough, as far as the massive lymph vessels are concerned [15]. The diploma of insufficiency in lipoedema sufferers, if current, by no means nevertheless reached the level of true persistent venous insufficiency or lymphoedema [10,eleven,21,22]. The lymphatic transport in lipoedema decreases as the body ages and the fibrosis will increase [15]. Clinical variants A classification based mostly on the situation of involved areas has been proposed [25]: I Mostly buttocks. Differential analysis Differential prognosis of lipoedema consists of lymphoedema, obesity, persistent venous insufficiency and lipohypertrophy (Table 100. Chronic venous insufficiency is associated with hyperpigmentation and, initially, pitting oedema that can be relieved by leg elevation; with time, however, lymphoedema could supervene. The primary distinction between lipohypertrophy and lipoedema is the absence of oedema and pain in lipohypertrophy [15]. Other differential diagnoses include Dercum illness and benign symmetrical lipomatosis. Predisposing components Although overweight patients could also be overrepresented, individuals with normal weight are additionally affected [1,2,9,16]. Pathology No histological abnormalities have been identified by haematoxylin and eosin (H&E) stains, fats stains or electron microscopy [9,10,thirteen,14,16�19]. Genetics A significant portion (16�64%) of affected ladies have a self reported optimistic household historical past of lipoedema [1,eleven,14]. Pit1 muta- Complications and comorbidities Mobility may be considerably impaired. No specific abnormalities have been found in phlebograms or arteriograms from lipoedema sufferers [16,18,19]. Ideally, it must be performed early, and multiple sessions are sometimes required [15]. Patients expertise important enchancment in swelling, ache, mobility, appearance and quality of life [24,25,31�33]. Decongestion remedy ought to remain an integral a part of postliposuction administration [24]. Lipolymphoedema Definition Lipolymphoedema is the coexistence of lipoedema and secondary lymphoedema. Management of food regimen is essential as a outcome of additional fats laid down in lipoedematous limbs may be abnormally resistant to control by dieting and exercise and will also compound the difficulties of taking adequate exercise, inflicting further frustration and low selfesteem [15,20,27]. Complex physical decongestion therapy, which combines manual lymphatic drainage and compression remedy, is extensively accepted as a conservative therapeutic method [13,20,29,30]. While manual lymphatic drainage reduces the precise volume, compression by stocking or bandage is used to decrease recurrence. Compression remedy could enhance, partly, the symptoms of lipoedema and in addition mitigate the progression of the lymphatic part. Certainly, sufferers with concomitant continual venous insufficiency and/or lymphoedema will benefit from compression remedy [15]. In lipoedema sufferers, nonetheless, regardless of lifelong decongestion therapy, the amount of sub- introduction and general description Secondary lymphoedema may coexist in sufferers with longstanding lipoedema and the distinction between the two entities is usually a problem. The increased strain from expansion of fats tissues in lipoedema contributes to the event of lipolymphoedema by inflicting mechanical obstruction of small lymphatic vessels. However, the increased pressure from the expansion of fats tissues might trigger mechanical obstruction of the small lymphatic vessels within the septa, resulting in delicate lymphostasis and oedema of the subcutaneous tissue. Furthermore, lymphatic transport in lipoedema also decreases as fibrosis will increase with age, and this could exacerbate the secondary lymphoedema [1].
The septa of the subcutaneous fat additionally include a outstanding lymphatic plexus menopause the musical chicago discount evista 60 mg overnight delivery, which comes from the dermis and traverses the subcutis menstrual yoga poses evista 60 mg cheap otc, first menstruation 2 weeks after ovulation 60 mg evista cheap otc, parallel to the floor of the skin after which vertically penetrating the underlying fascia and draining into regional lymph nodes. The connective tissue septa, that are contiguous with the overlying reticular traverses and with the underlying fascia, provide stability to the subcutaneous tissue by compartmentalizing it. The regular septa are skinny, from 200 to 300 m, and are composed mostly of collagen bundles and thin elastic and reticulin fibres. Mature regular individual adipocytes are comparatively large cells with a diameter up to 100 mm and, in formalinfixed and H&Estained sections, appear as empty cells with signetring morphology. Predominantly septal panniculitides With vasculitis Veins Arteries No vasculitis Lymphocytes and plasma cells predominantly With granulomatous infiltrate in septa No granulomatous infiltrate in septa Histiocytes predominantly (granulomatous) With mucin in centre of palisaded granulomas With fibrin in centre of palisaded granulomas With massive areas of degenerate collagen, foamy histiocytes and ldl cholesterol clefts Without mucin, fibrin or degeneration of collagen, however with radial granulomas in septa Predominantly lobular panniculitides With vasculitis Small vessels Venules Large vessels Arteries No vasculitis Few or no inflammatory cells Necrosis on the centre of the lobule With vascular calcification Lymphocytes predominant With superficial and deep perivascular dermal infiltrate With lymphoid follicles, plasma cells and nuclear mud of lymphocytes Neutrophils predominant Extensive fats necrosis with saponification of adipocytes With neutrophils between collagen bundles of deep reticular dermis With micro organism, fungi or protozoa With foreign our bodies Neutrophilic lobular panniculitis (subcutaneous Sweet syndrome) Histiocytes predominant (granulomatous) No crystals in adipocytes With crystals in histiocytes or adipocytes Superficial migratory thrombophlebitis Cutaneous polyarteritis nodosa ninety nine. Frozen sections and particular stains similar to oil purple O or Sudan B are required to reveal the lipid contents throughout the cytoplasm of mature adipocytes. Perivascular adipocytes have been additionally demonstrated to be highly effective endocrine cells able to responding to metabolic adjustments and transducing alerts to adjoining blood vessels. Cross talk between perivascular adipose tissue and blood vessels is now being intensely investigated. There is evidence suggesting that perivascular adipose tissue regulates vascular function via quite a lot of mechanisms and plays an necessary position in irritation and vasoreactivity in subcutaneous tissue [6]. Normal subcutaneous fat incorporates T lymphocytes situated between adipocytes of the fat lobule. They differ from those of different tissues and differ between completely different regions of the physique [7]. It has lately been demonstrated that cytotoxic T lymphocytes precede the buildup of macrophages during the means of irritation of the fat lobule. In vitro cocultures have proven a vicious cycle of interplay between cytotoxic T lymphocytes, macrophages and adipocytes, suggesting that adipocytes activate cytotoxic T lymphocytes with subsequent recruitment and activation of macrophages [8]. Immunohistochemically, adipocytes categorical S100 protein, with staining around the periphery of the cell, and vimentin [10]. In distinction with the multivacuolated cytoplasm of sebocytes and foamy histiocytes, which categorical adipophilin, the only large cytoplasmic vacuole of the adipocyte is adipophilin adverse [11,12]. Patternbased histopathological classification of panniculitis with massive vessel vasculitis also requires ascertainment of whether or not the involved vessel is an artery or a vein. Nevertheless, many authors continue to promote the deceptive notion that arteries of the subcutaneous fats of the lower legs have a thicker muscular layer than veins, when in reality veins typically have a thicker muscular layer than arteries [13]. Some authors, nonetheless, believe that when inflammation is present within and across the wall of the vessel, all of the studied histological features turn out to be much less reliable, and that the interobserver reliability of distinguishing arteritis from thrombophlebitis is low [14]. In classical histopathology, nuclear abnormalities such as pyknosis, karyorrhesis and karyolysis are signs of mobile necrosis. In contrast, necrotic adipocytes, regardless of the aetiology of the cell demise, show great variability and will appear as both anucleate cells or with complete disintegration of the cellular construction. Unfortunately, these distinctive types of adipocyte necrosis have little worth for diagnostic specificity. Often, the only sign of necrosis of the adipocytes is the dearth of nuclei within the concerned cells, and lifeless fat cells seem as round empty baggage with no inflammatory infiltrate among them. The most frequent type of adipocyte necrosis is lipophagic necrosis, which consists of the alternative of necrotic adipocytes by foamy macrophages fashioned by the engulfing of lipid merchandise launched from dead adipocytes by macrophages. These lipophages seem fairly completely different from normal adipocytes, with giant pale microvacuolated or granularlike cytoplasm and spherical central vesicular nuclei. Lipophagic granulomatous irritation, nonetheless, is completely nonspecific and plenty of lobular panniculitides present this pattern of fat necrosis at their late or resolving phases. It is normally seen in lipodermatosclerosis and traumatic panniculitis, but may be current in erythema nodosum and erythema induratum of Bazin. Necrotic adipocytes injured by this mechanism appear as granular wisps of amphophilic detritus and their cellular buildings are no longer evident. Enzymatic fat necrosis is a particular kind of liquefactive fats necrosis characteristically noticed in pancreatic panniculitis. It is as a outcome of of saponification of the adipocyte lipid contents by pancreatic lipase, with secondary deposition of calcium salts, leading to socalled ghost adipocytes, which include adipocytes with no nuclei and granular basophilic cytoplasm. Hyalinizing fat necrosis is characteristically noticed in lupus panniculitis and panniculitis associated with dermatomyositis. In this pattern, necrotic adipocytes seem as mummified anucleated cells, which are surrounded by glassy homogeneous proteinaceous materials, effacing the structure of the fat lobule. When membranous fat necrosis is extensive, formation of cystic buildings devoid of cellular components and lined by hyalinecrenulated membrane can be noticed. Membranous and membranocystic fats necrosis are almost at all times seen in lipodermatosclerosis, but like other kinds of fats necrosis, they could also be seen in latestage lesions of several kinds of panniculitis. Ischaemic fat necrosis is extra regularly seen at the centre of fats lobules and is characterised by pallor of adipocytes, that are smaller than regular as a result of extreme impairment of blood provide. Ischaemic fat necrosis is incessantly seen in erythema induratum of Bazin, but can also be observed in other panniculitides, including calcific uraemic arteriolopathy (calciphylaxis), infectious panniculitis and cutaneous polyarteritis nodosa. Finally, basophilic fats necrosis results from necrosis of adipocytes intermingled with nuclear dust of neutrophils and granular basophilic materials, which characterize aggregations of bacteria and is characteristically seen in circumstances of infectious panniculitis. There are some disorders that ought to no longer be thought of as specific variants of panniculitis. Weber�Christian illness is the time period that has been classically used to refer to circumstances of predominantly lobular panniculitis with out vasculitis in association with systemic manifestations together with fever and involvement of visceral fats tissue. Additional phrases similar to idiopathic nodular panniculitis, nodular panniculitis and relapsing febrile non suppurative nodular panniculitis have been used as synonyms for Weber�Christian disease. However, many cases originally thought of as examples of Weber�Christian illness have been later reclassified when other variants of lobular panniculitis, together with erythema induratum of Bazin (nodular vasculitis), pancreatic panniculitis and 1antitrypsin deficiency panniculitis had been separated as specific illnesses. The authors concluded that the time period Weber�Christian illness should be abandoned as a diagnosis for cases of lobular panniculitis as a end result of now a more particular diagnosis may be reached within the majority of circumstances. The same is true for Rothmann�Makai disease, a term that was used previously to describe cases of relapsing nodular panniculitis much like that of Weber�Christian illness but with no fever or other systemic manifestations. Varicosities and erythematous nodules with linear association involving the proper decrease extremity. The causes of secondary hypercoagulable states are various, but within the majority of instances venous insufficiency of the decrease extremities is the only precipitating factor. The process is more inflammatory than thrombotic, with distinguished fibrinoid necrosis of the tunica intima, resulting in the socalled targetlike arteritis, in which an eosinophilic ring of fibrinoid necrosis replaces the intima of the affected arteriole. Some authors, nonetheless, imagine that when irritation is present within and around the wall of the vessel, the identification of the internal elastic lamina of the concerned vessel is less dependable even with elastic tissue stains, and the graceful muscle sample has the highest sensitivity and specificity for distinguishing arteries from veins [17]. In early lesions, the inflammatory cell infiltrate is composed principally of neutrophils, whereas in later stages there are lymphocytes, histiocytes and occasional multinucleated giant cells. Direct immunofluorescence studies of lesions of cutaneous pol- yarteritis nodosa have demonstrated IgM and complement deposition in the concerned vessel walls and constant absence of IgG [3]. The concerned vessel appears with a thickened wall, within which an inflammatory infiltrate is seen. In early lesions, a neutrophilic infiltrate and leukocytoclasis are sometimes seen and, in some cases, eosinophils may be outstanding [4]. Characteristically, the intima of the involved artery displays an eosinophilic ring of fibrinoid necrosis, giving a targetlike look to the damaged vessel. A rare complication is the formation of periosteal new bone beneath the cutaneous lesions [5]. Often, arterial involvement is segmental and serial sections all through the whole specimen are required to demonstrate the pathology. As is the case in superficial thrombophlebitis, lesions of cutaneous polyarteritis nodosa show little or no involvement of the adjacent fats lobule, and the process is completely a septal arteritis. It is associated within the majority of but not all cases with underlying diabetes, the onset of which it could precede. There are palisading granulomas with histiocytes surrounding areas of degenerate collagen within widened septa. The most attribute characteristic supporting a prognosis of necrobiosis lipoidica as the cause for an inflammatory course of involving the subcutis is the coexistence of comparable lesions within the dermis, with alternating horizontal bands of inflammatory cells and fibrosis involving the whole dermis [2]. Early lesions present an inflammatory infiltrate composed predominantly of neutrophils scattered within the septa, whereas in later lesions, histiocytes, lymphocytes and plasma cells, sometimes with lymphoid follicle formation [3], are predominant. Multinucleated big cells involving the septa are sometimes distinguished and in those cases histopathological findings resemble erythema nodosum. In persistent longstanding lesions, the dermis and the superficial subcutaneous tissue are replaced by horizontal fibrosis with sclerotic collagen bundles arranged parallel to the dermis and scattered by plasma cells, intently resembling the findings seen in morphoea.

The etiology of external ear malformations and its relation to abnormalities of the middle ear menstruation after tubal ligation evista 60 mg cheap otc, internal ear women's health center plainfield il order 60 mg evista with mastercard, and other organ systems menstrual cramps 9 months pregnant buy 60 mg evista with amex. Are tattooing and body piercing indicators of risk-taking behaviours amongst high school students Decrease in nickel sensitization in a Danish schoolgirl inhabitants with ears pierced after implementation of a nickelexposure regulation. Keloids and hypertrophic scars: outcomes with intra-operative and serial post-operative corticosteroid injection remedy. Advances in the understanding of chondrodermatitis nodularis chronica helices: the perichondrial vasculitis principle. Effective remedy of chondrodermatitis nodularis chronica helicis using a conservative method. Self-adhering foam: a simple technique for strain relief throughout sleep in patients with chondrodermatitis nodularis helicis. Intralesional triamcinolone for chondrodermatitis nodularis: a follow-up research of 60 patients. Topical nitroglycerin: a promising remedy option for chondrodermatitis nodularis helicis. The long-term outcomes of cartilage removing alone for the remedy of chondrodermatitis nodularis. Simplified surgical remedy of chondrodermatitis nodularis by cartilage trimming and sutureless pores and skin closure. Chondrodermatitis nodularis helicis successfully handled with photodynamic remedy. Clinical traits and comparative research of various modalities of remedy of pseudocyst pinna. Recurrent auricular pseudocyst: a model new treatment suggestion with curettage and fibrin glue. Treatment of recurrent auricle pseudocyst with intralesional injection of minocycline: a report of two circumstances. Comparative analysis between Pseudomonas aeruginosa genotypes and severity of symptoms in patients with unilateral or bilateral otitis externa. Papules in the auricular concha: lichen amyloidosus in a case of biphasic amyloidosis. Solitary congenital nodular calcification of Winer located on the ear: report of two cases. Purpura of the ears: a particular vasculopathy with circulating autoantibodies complicating long-term treatment with levamisole in youngsters. High-risk cutaneous squamous cell carcinoma of the pinnacle and neck: results from 266 handled sufferers with metastatic lymph node disease. Cutaneous squamous cell carcinoma in organ transplant recipients: a study of the Swedish cohort with regard to tumor website. Five-year outcomes of curettage-cryosurgery for a hundred consecutive auricular non-melanoma skin cancers. Radiotherapy of pores and skin carcinomas of the pinna: a examine of a hundred and fifteen lesions in 108 patients. Maintenance versus reduction of immunosuppression in renal transplant recipients with aggressive squamous cell carcinoma. Squamous carcinoma of the external auditory canal 1 Arriaga M, Curtin H, Takahashi H, et al. Staging proposal for exterior auditory meatus carcinoma based on preoperative scientific examination and computed tomography findings. Squamous cell carcinoma of the exterior auditory canal: an analysis of a staging system. The role of facial palsy in staging squamous cell carcinoma of the temporal bone and external auditory canal: a comparative survival evaluation. Prognostic components for squamous cell carcinoma of the temporal bone: in depth bone involvement or intensive gentle tissue involvement Surgical strategy for therapy of carcinoma of the anterior wall of the exterior auditory canal. Treatment and prognosis of squamous cell carcinoma of the external auditory canal and middle ear: a multi-institutional retrospective evaluation of 87 sufferers. Primary radical radiotherapy for squamous cell carcinoma of the middle ear and exterior auditory canal-an historical series. Cholesteatoma of the external ear canal: etiological components, symptoms and clinical findings in a sequence of 48 instances. Erosive external otitis: a novel distinct scientific entity of the external auditory canal in nonimmunosuppressed individuals. Otomycosis in immunocompetent and immunocompromised sufferers: comparative study and literature evaluation. Ceruminous adenomas: a clinicopathologic examine of forty one cases with a evaluate of the literature. Prognostic factors for native recurrence, metastasis and survival rates in squamous carcinoma of the pores and skin, ear and lip. The primary focus is on those situations that generally happen in clinical apply and that present a problem with management. It can also be supposed to alert the dermatologist to circumstances that might threaten visible acuity and require pressing referral to an ophthalmologist. Also, many systemic illnesses affect both the pores and skin and eyes, and ophthalmic evaluation shall be of help in making the right analysis and in the longterm management of such sufferers. Eyebrows this hairbearing space rests on a very cell fat and muscle pad overlying the superior orbital ridge. The grey line, an necessary anatomical landmark for surgical restore and pathological conditions of the lid margin corresponding to blepharitis, divides the lid into an anterior lamella (skin and muscle) and a posterior lamella (tarsus and conjunctiva). The gray line represents the placement of the marginal area of the orbicularis muscle (muscle of Riolan) seen by way of the lid skin. It contains sebaceous glands associated with the fantastic hairs of Anatomy and physiology of the attention [1,2] the attention and pores and skin share a standard embryological origin. The structure of the lid, conjunctiva, lacrimal gland and associated drainage apparatus are of floor ectodermal origin whereas the remainder of the attention arises from epithelium of the ectodermal neural plate. There are about 300 eyelashes, arising in two rows along the eyelid margin, twothirds of which are within the upper lid. Some lashes, significantly those of the lower lid, are associated with ancillary apocrine sweat glands (of Moll). The ducts of these glands open both into the lash follicles and directly onto the anterior lid margin between the lashes. Each lash follicle has a rich nerve plexus, which is definitely excited � mild touch initiates reflex closure. They comprise dense, fibrous tissue surrounding modified sebaceous glands (meibomian glands). These secrete the outer lipid layer of the precorneal tear film through openings alongside the mucocutaneous junction of the eyelid margin. Meibomian glands have as much as 20 acini surrounding a central vertical duct and are seen via the conjunctiva. It is mirrored over the anterior portion of the eyeball as much as the edge of the cornea as the bulbar conjunctiva. The folds shaped by the reflection of the conjunctiva from the lids onto the eyeball are known as the superior and inferior palpebral fornices. The conjunctiva contains numerous goblet cells secreting mucin into the tear movie. It additionally accommodates about 50 accent lacrimal glands and its substantia propria accommodates neural tissue, mast cells, lymphocytes and lymphoid follicles, that are essential in mediating local immunological reactions. The striated muscle of the levator palpebrae superioris opens the eye, and the striated orbicularis oculi muscle closes it. Two divisions of the trigeminal nerve provide sensation to the eyelids; the upper lid and medial canthus are provided by the ophthalmic division, and the rest of the decrease lid by the maxillary division.
To add to the confusion menstruation medicine buy evista 60 mg with visa, abortive forms of Buschke�Ollendorff syndrome have been described menstrual kotex generic 60 mg evista fast delivery, missing osteopoikilosis [5] women's health clinic gladstone evista 60 mg buy cheap on line. Clinically and histologically, the lesions resemble elastomas, however this uncommon condition has solely been reported in elderly Japanese males [1,2]. The painless or slightly tender swelling beneath the lower angle of the scapula, from 2 to 10 cm in diameter, is commonly found fortuitously. It could enlarge slowly, displacing neighbouring constructions, and it could be clinically confused with a sarcoma. The development is composed of mature fibrous tissue, containing fibres which stain as elastic fibres. Histologically, the lesion accommodates ample massive elastic fibres, some broken into irregular masses, and enormous quantities of comparatively acellular collagen. The elastic f]ibres are composed of true elastin surrounded by a great amount of hydrophilic material forming an orderly array of tubules [4]. It is mostly regarded either as a type of reactive hyperplasia, or as a hamartoma, arising both from dermis, subscapular connective tissue or periosteum [6]. There are some cases, however, that defy exact classification, and others by which histological criteria may be a poor guide to prognosis. Invasiveness and a high local recurrence rate may or is probably not related to an inclination Fibromatoses 96. The borderline between easy overgrowth and a benign tumour may be equally difficult to define. Abnormal fibrosis is a function of many debilitating systemic disorders, such as cirrhosis and pulmonary fibrosis. Fibromatoses Fibromatosis is a benign fibrous tissue proliferation, which is intermediate between benign fibroma and metastasizing fibrosarcoma. The lesions in fibromatosis may be single or a quantity of, and the probability of recurrence after surgical removing varies with the placement of the lesion and the age of the patient. The fibromatoses happen in two main groups: 1 Superficial fibromatoses (fascial fibromatoses): (a) palmar (Dupuytren); (b) plantar; (c) penile (Peyronie); (d) knuckle pads. These are rapidly rising tumours that usually involve the musculature or aponeuroses. Their tendonlike consistency accounts for their various name of desmoid tumours. It occurs extra commonly in patients with alcoholic cirrhosis, epilepsy [6] and diabetes [4,7], but the prevalence is decreased in rheumatoid arthritis [8]. Other conditions which have been much less convincingly claimed to be associated embrace periarthritis of the shoulder, persistent lung illness, gout, trauma and ulnar nerve injury [9]. There is one case report of a lady aged 14 years who developed Dupuytren contracture while receiving growth hormone remedy for hypopituitarism [12]. High alcohol consumption, smoking and trauma, notably the use of vibrating hand tools, have additionally been implicated [13]. Clinical features History Nodules could also be painful initially, though the situation sometimes develops insidiously over several months or years. Localized ischaemia has been thought to play an element, and in animal studies allopurinol (a aggressive inhibitor of xanthine oxidase) has been proven to limit the injury associated with acute ischaemia [15]. High concentrations of free radicals are toxic, however in low concentration they stimulate fibroblast proliferation [14]. The contractures, which are a late complication, seem to follow the conversion of the fibroblasts to contractile myofibroblasts [16]. Presentation the earliest sign is the development of a palmar nodule, normally within the ulnar half of the hand. Insidious progression of the fibrosis over a number of years causes flexion contractures of the affected fingers. Clinical variants Plantar and penile fibromatosis are closely associated situations (see later). There may be a histological resemblance to fibrosarcoma, but the latter is more pleomorphic, with bigger nuclei and more mitoses. Pathology Fibroblasts in affected fascia seem to be similar to those in normal palmar fascia however their density is elevated and they tend to be clustered round narrowed small vessels [18,19]. Later levels are characterised by the presence of myofibroblasts, which have a fibrillary cytoplasmic ultrastructure and seem to have some other properties of easy muscle. The nuclei are deeply indented, probably because of the contractile properties of the cell. The cells even have altered surface membrane properties which allow attachment to neighbouring cells and stroma. Myofibroblasts have additionally been identified in the normal aorta and in granulation tissue, hypertrophic scars, keloids, liver fibrosis, dermatofibromata, and so forth. The superior phases of palmar fascial fibromatosis are characterized by dense fibrous connective tissue with a few elongated cells. This could additionally be because of decreased degradation ensuing from increased levels of tissue metalloproteinase inhibitors within the lesions [21]. Structural abnormalities of glycosaminoglycans, notably dermatan sulphate, might predispose to abnormal fibrillogenesis [22]. Disease course and prognosis the situation tends to progress extra slowly in ladies [9]. Eventually, the perform of the hand is impaired due to fixed flexion of a quantity of digits. Traditionally full removing of the palmar aponeurosis has been recommended [26], although minimally invasive subtotal fasciectomy and direct closure is extra usually favoured [27,28]. Initial encouraging placebocontolled trials of collagenase injections [29] have been supported by subsequent experience, and the method is now extra widely practised [30]. Allopurinol could help by lowering free radical production [31], and it has been advised that vitamin C might forestall development of the disease by performing as a freeradical scavenger [2]. Many other nonsurgical approaches have been tried, together with steady slow skeletal traction, radiotherapy, dimethyl sulfoxide, vitamin E, steroid injections and interferon, although none has been confirmed to be clinically useful [32]. Highdose tamoxifen following minimally invasive surgical procedure reduces the chance of recurrent fibrosis within the short term, but the effect is misplaced on discontinuing the drug [33]. Intriguing outcomes have been reported from using relaxin gene remedy on Dupuytren myofibroblasts in vitro, with the potential for use in vivo [34]. Genetics Palmar fascial fibromatosis is usually familial, and could additionally be inherited as an autosomal dominant trait [23], by which case the onset tends to happen at an earlier age [24]. Genomewide research show elevated expression ranges of metalloproteinases 1, 3 and 16, fibroblast growth factor and a variety of other collagen genes [25]. Environmental elements Occupational publicity to handtransmitted vibration could also be an exacerbating issue [13]. Total excision of the lesion and the entire plantar fascia seems to give the best outcomes, with the bottom incidence of recurrence. Synonyms and inclusions � Peyronie disease � Plastic induration of the penis � Fibrous sclerosis of the penis Plantar fascial fibromatosis [1,2] Definition and nomenclature this can be a rarer condition than palmar fascial fibromatosis, though typically associated; a survey from Reykjavik found that 15% of men with the latter had plantar fibromatosis [3]. The fibromatosis not often ends in contractures however tends to be regionally invasive and to recur. Synonyms and inclusions � Ledderhose disease pathophysiology Penile fibromatosis might happen as an isolated abnormality, or as one component of polyfibromatosis in association with palmoplantar fibromatosis, keloids and knuckle pads. There may be a genetic issue, however reliable studies of the mode of inheritance are lacking. The condition is uncommon beneath the age of 20 years, and the best incidence is between forty and 60 years. Differential analysis the differential diagnosis consists of keloid and fibrosarcoma. Magnetic resonance imaging may confusingly reveal the cerebriform pattern typically seen in fibromyxoid sarcoma [4]. In youthful patients, aggressive childish fibromatosis and aponeurotic fibroma should also be considered [5]. Complications are rare, although squamous carcinoma has been reported occurring within a lesion of plantar fibromatosis [6].






