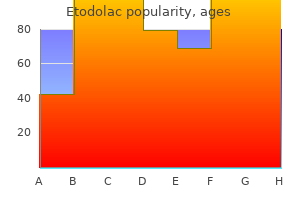
Etodolac
Etodolac
Etodolac dosages: 400 mg, 300 mg, 200 mg
Etodolac packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
Renal insufficiency is a significant complication of surgical procedures requiring cross-clamping of the thoracic or suprarenal aorta rheumatoid arthritis without rheumatoid factor 300 mg etodolac discount visa. The data regarding renal safety in vascular surgery sufferers are conflicting and have been extrapolated primarily from sufferers present process cardiac surgery procedures rheumatoid arthritis cure etodolac 300 mg discount with mastercard. Whether the renal dysfunction after renal vein ligation is solely a consequence of the resultant increased venous strain or develops from a mix of venous hypertension and transient ischemia from intraoperative suprarenal clamp placement arthritis symptoms in back or spine 200 mg etodolac cheap with visa, which is required more frequently than with infrarenal clamp placement (11% vs. The quality of the renal pulses must be evaluated and the blood circulate assessed by Doppler color-flow imaging after restoration of circulation through the aorta in any affected person who has had important juxtarenal aortic manipulation. Postoperatively the continued retroperitoneal and intraperitoneal sequestration of, extracellular fluid requires replacement with lactated Ringer resolution, throughout the limits imposed by left-heart filling pressures, to guarantee adequate renal output. The urinary output is monitored constantly and ought to be maintained at or above 0. Several biomarkers are at present being investigated in patients present process cardiac surgical procedure to enhance the detection of early renal dysfunction. Dialysis is used aggressively to control extra quantity and relieve azotemia and hyperkalemia. Often, renal revascularization could be accomplished by balloon angioplasty and stenting, along with operative or endovascular correction of the aortic disease. In this setting, patients typically have impaired renal function, and the big volume of contrast brokers used for imaging studies or intervention could lead to additional nephrotoxicity the preoperative administration of. Welten and associates, in a research of 2170 sufferers undergoing decrease extremity bypass or belly aortic surgical procedure, demonstrated that early statin use increased the chances of recovery if renal perform deteriorated postoperatively 154,one hundred fifty five In addition, statin use was also associated with. Intestinal Ischemia Intestinal ischemia may complicate aortic bypass or endarterectomy for occlusive disease, but the majority of instances involve the colon and observe aneurysmectomy 156,157. Almost all reported cases of intestinal ischemia following aortic surgery are a results of arterial obstruction or hypotension; venous ischemia is extremely uncommon. The total mortality rate for sufferers with colon ischemia is roughly 50% and approaches 90% for transmural colon involvement. Occlusion of the orifice of the inferior mesenteric artery is regularly associated with aneurysmal disease and obstructive aortic atherosclerosis, thus inserting the burden of bowel circulation on collaterals from the superior mesenteric artery and the hypogastric vessels. Severe obstruction or occlusion of the superior mesenteric artery is compensated for by branches from the celiac artery and retrograde flow from the inferior mesenteric artery by way of the left colic and middle colic arteries. Hypogastric obstruction requires collateral move from branches of the inferior mesenteric artery When this supply is also impaired, colon circulation must. Failure to ensure perfusion via no less than one hypogastric might promote colon ischemia if that is the primary provide within the absence of the inferior mesenteric artery or efficient collateral flow from the meandering artery Loss of the inferior mesenteric artery or the meandering artery. The massive hematoma related to a ruptured aneurysm could compress significant collateral vessels, which can clarify the excessive incidence of colon ischemia on this circumstance. Prolonged hypotension and the usage of vasopressors could exacerbate the effects of preexisting occlusive disease. Abdominal issues after coronary artery bypass occur in lower than 1% of patients. Acute mesenteric ischemia accounts for 10% to 67% of those issues, with mortality rates of 70% to 100%. Meandering mesenteric sacrifice under these circumstances predisposes to small bowel and colon ischemia. Findings that suggest the presence of intestinal ischemia and progressing infarction of the colon include progressive distention, sepsis, rising peritoneal signs, and unexplained metabolic acidosis. The commonest medical presentation is diarrhea- both brown liquid or bloody-which happens in 65% to 76% of patients with intestinal ischemia. Therefore, in critically sick sufferers who develop fever, abdominal distension, diarrhea, and leukocytosis after emergency aortic procedures, stool specimens for culture and for C. Appropriate oral antibiotic remedy (metronidazole or vancomycin) ought to be instituted if the analysis of C. The diagnosis depends on a high index of suspicion and the immediate efficiency of endoscopy with the versatile sigmoidoscope or colonoscope. Adjunctive procedures were used in 12% of these patients, compared with 4% in earlier research from their establishment. Sigmoid colon pH monitoring begun earlier than surgical procedure and continued postoperatively has been used with some success by Bj�rck and Hedberg to establish sufferers at risk for ischemic colitis. Further evaluation of sigmoid colon pH monitoring seems warranted earlier than its widespread software. The incidence of ischemic colitis without left colon involvement is uncommon sufficient that endoscopy to 40cm is often sufficient to set up the analysis. In a current report, Acosta and colleagues demonstrated elevated D-dimer concentrations in patients with acute mesenteric ischemia. Wider application of this test to different causes of acute mesenteric ischemia awaits validation. Patients beneath remark for intestinal ischemia are managed by frequent reexamination; serial endoscopy; sigmoid colon and gastric intramucosal pH monitoring; monitoring of blood gases and serum lactate ranges, white blood cells and D-dimers, urine output, and fluid requirements; institution of broad-spectrum antibiotic coverage; and bowel rest with nasogastric suction. Plain radiographs might reveal a nonspecific ileus, dilated loops of bowel, or thumb printing; intramural or portal vein gasoline are rarely seen and normally indicate late-stage illness. If the colon appears distended, both clinically or radiographically it should be decompressed by the gentle insertion of, a rectal tube because elevated intraluminal strain could further compromise colon blood flow. Improvement of the patient, as evidenced by diminishing diarrhea, improvement in vital indicators, scientific examination, laboratory values, and resolution of the ischemia documented by endoscopy permits continuation of nonoperative administration. Prevention of intestinal ischemia depends on an appreciation of the potential for this complication and the institution of applicable steps to either avoid harm to the collateral circulation of the colon or augment circulation to the bowel as a half of the aortic reconstructive process. This technique permits a number of views of advanced aortic lesions, displays the true diameter of aortic aneurysms, and should alleviate the necessity for angiography 178,179 Identification of a patent inferior mesenteric. Intraoperative duplex ultrasonography in patients present process visceral artery repair permits prompt correction of underlying technical defects. When inferior mesenteric ligation is required, this ought to be carried out by suture ligature within the aortic lumen or immediately adjoining to the aortic wall to keep away from damage to its ascending and descending branches. The affiliation of severe visceral and aortic occlusive disease in youthful female patients is accompanied by excessive mortality and morbidity charges. The extreme weight loss resulting from celiac and superior mesenteric artery occlusive lesions makes full revascularization a hazardous undertaking. In these individuals, a mixture of endovascular remedy of the visceral occlusive disease before aortic revascularization might decrease the early morbidity and mortality rates, and improve long-term survival. This dialogue might be restricted to paralytic ileus and mechanical small bowel and duodenal obstruction, the commonest issues encountered. The enhance in intraoperative blood loss and postoperative fluid requirements associated with these issues accounts for the extended requirement for mechanical ventilation and the occurrence of renal failure. The presentation is commonly delayed, with symptoms occurring eight to 60 days (mean, 13. Symptoms include increased nasogastric tube output, nausea, bilious vomiting, stomach ache, distension, hematemesis, hematochezia, diarrhea, fever, leukocytosis, and a decrease in hematocrit level. Therefore, a 1- to 2-week trial of conservative therapy in these sufferers is reasonable. Patients with obstruction lasting longer than 2 weeks nearly always require operative relief of the obstruction. Fluid and electrolytes should be replaced, a nasogastric tube reinserted, and diet supplied. Operative aid of the obstruction is indicated in sufferers with obstruction lasting longer than 2 weeks or if problems ensue. There had been no bowel infarctions, small bowel fistulas, or late graft infections in the aortic patients present process laparotomy for bowel obstruction. The associated decrease in venous return, compounded by hypotension, reduces cardiac output and will increase peripheral resistance, resulting in impaired renal, hepatic, and mesenteric perfusion; a rise in bacterial translocation from the intestine; and raised intracranial stress, which, if uncorrected, ends in the elevated morbidity and mortality in these sufferers. The indirect technique requires emptying the bladder and instilling 50 to 150mL of saline; the drainage tubing is clamped and a needle connected to the strain transducer is inserted above the clamp and the stress determined. If the bladder stress exceeds 20mm Hg, the pressure must be monitored hourly A bladder stress of larger than 30mm Hg is. A short course of a neuromuscular blocking agent may decrease fascial edge retraction and be a helpful adjunct to negative strain devices and conservative measures. Mass suturing of the musculoaponeurotic layers of the belly wall using monofilament or braided suture is the most frequently used approach to close midline incisions. Also, a suture length�to�wound length ratio greater than 4 reduces the incidence of incision lesions. Primary restore using monofilament nonabsorbable suture is acceptable for closure of small periumbilical defects. Surgical or laparoscopic repair utilizing prosthetic mesh is often essential to repair massive defects in the higher abdomen.
Correction of abnormalities within the graft or within the vessels adjacent to a failing graft ought to be carried out as soon as reduced perfusion has been recognized rheumatoid arthritis liver generic etodolac 300 mg visa. Anticoagulants may prevent thrombosis in the presence of progressing stenosis if surgical procedure must be delayed rheumatoid arthritis gwas etodolac 300 mg cheap free shipping. However arthritis in my neck what can i do buy generic etodolac 400 mg on-line, once occlusion has occurred, the longer the thrombus has been present, the less effective recanalization attempts might be. Areas of isolated stenosis throughout the graft, at an anastomosis, or in the influx or outflow arteries may be successfully managed by percutaneous balloon angioplasty 297. These fibrous vein graft lesions are sometimes troublesome to dilate and will require using chopping balloons and high-pressure balloons typically inflated from 10 to 20atm. Primary, primary assisted, and secondary patency rates of 38%, 58%, and 84%, respectively at 24, months after balloon angioplasty have just lately been reported by Eisenberg and colleagues. Progressive disease in the inflow vessels requires a leap graft from the decrease end of the unique graft to a patent distal popliteal or infrapopliteal artery to bypass the obstruction. Prosthetic graft declotting can typically be achieved by way of a single distal graft opening if the thrombosis is current. Operative angiography under fluoroscopic guidance is required after declotting of either venous or prosthetic grafts to affirm the thrombus has been extracted completely to view both, anastomoses, to evaluate the complete size of the intervening graft to identify areas of stenosis that have to be repaired, and to reevaluate the inflow and the runoff bed. The endothelial lining of vein grafts and of small runoff vessels is spared the trauma of mechanical thrombectomy which can be an necessary, factor in restored vein graft function long term. Although effective lysis may be completed several weeks after an occlusion has occurred,79,338 greatest outcomes with this form of remedy are normally achieved inside hours or days of thrombosis. As quickly because the clot has been successfully cleared from the graft by lytic therapy, angiographic investigation of the entire length of the graft, both anastomoses, the influx, and the runoff bed is required to establish the trigger of graft failure, which should be corrected to keep away from reocclusion. In the interim between lytic recanalization and correction of the causes of graft thrombosis, patients should be effectively anticoagulated to forestall rethrombosis. Graft stenoses or deterioration of influx or runoff vessels must be recognized and corrected to obtain long-term patency and limb salvage. Autogenous vein is preferable to prosthetic materials, particularly for bypasses to the infrapopliteal arteries. The long-term outcomes with prosthetic materials are poor when used for secondary bypass, whereas arm veins have been shown to have long-term patency charges almost equal to those of saphenous vein. Curi and associates reported a 13% incidence of numerous hypercoagulable states in this patient inhabitants. Failure to identify and proper the reason for graft occlusion usually suggests a poor prognosis, as a result of the underlying trigger has not been removed. For this cause, antiplatelet therapy in the immediate postoperative period is indicated. Reoperation to maintain extremity circulation is worthwhile because prolonged limb salvage may be achieved in 40% to 60% of sufferers undergoing four or more reoperative procedures. Warfarin in the therapeutic vary augmented the patency of low-flow grafts, which occluded extra frequently than higher-flow grafts (46% vs. The reported incidence of serious wound issues after autogenous and prosthetic infrainguinal bypass grafting ranges from 7. Independent predictors for wound an infection have been infrainguinal surgical procedure weight problems and an angiography injection website, within the operative space. Predisposing factors embody age, feminine gender, weight problems, diabetes mellitus, renal failure, anemia, postoperative anticoagulation, steroid therapy, ipsilateral limb ulceration or infection, and severity of ischemia. Technical elements, together with the size and placement of the incision, prolonged retraction, location of the distal anastomosis, and strategy of wound closure, might all influence the ultimate therapeutic of these incisions. The two parallel incisions required to mobilize the artery and vein for in situ grafting to the dorsalis pedis artery risk necrosis of the intervening skin bridge. Wound complications vary from erythema, hematoma/hemorrhage, and superficial necrosis of the margins, to an infection of the deeper layers with publicity of the graft. Gram-positive cocci and blended bacterial flora are frequently cultured from these wounds. Several steps assist to forestall wound complications after infrainguinal bypass procedures. Preoperative mapping of the course of the saphenous vein with duplex ultrasound minimizes the chance of creating a big posterior flap. The use of skip incisions and leaving skin bridges may be of value in some patients. Isolation of necrotic or ulcerative pores and skin lesions of the foot earlier than preparation of the pores and skin limits contamination of the operative subject. In patients present process in situ vein bypasses, valve incision with the LeMaitre valvulotome and detection of side branches with Doppler ultrasound, angiography or angioscopic steerage (when available) and ligation of aspect branches, by way of small incisions, could obviate the necessity for long continuous incisions and, as a consequence, scale back the incidence of wound problems. If a continuous incision is used, careful placement of the incision, meticulous hemostasis, and cautious pores and skin closure also scale back the incidence of wound problems. Once a wound complication has occurred, however, the remedy ought to be tailor-made to the severity of an infection. Wound erythema with minimal necrosis of the wound margins normally responds to appropriate antibiotics and local wound care. More intensive wound an infection and necrosis require intensive d�bridement and, usually, pores and skin grafting, muscle transfers, or myocutaneous-free flaps. Rarely an uncovered vein graft, ruptures, requiring removal of the graft and placement of a new conduit routed via uninvolved sites. Graft Surveillance Vein Grafts When implanted in the arterial system, vein grafts endure a sequence of morphologic adaptive adjustments that embody thickening of the wall, anastomotic intimal hyperplasia, valvular stenosis, dilatation, aneurysm formation, and atherosclerosis as a response to arterial blood stress. In actuality the in situ, technique might entail more manipulation and injury to the intima from using valvulotomes. Platelet thrombi happen on the sites of valve incision or splits in the intima along the size of the vein. Exploration of those websites, with careful removing of any thrombotic material and restore by patch angioplasty or substitute of the damaged vein phase, is often essential. Intraoperative duplex scanning of infrainguinal vein bypass grafts has been shown to establish problems that require revision in 10% to 27% of procedures (arm or spliced vein, 27%; in situ saphenous vein, 16%, nonreversed saphenous vein, 13%; reversed saphenous vein, 10%). Testing is begun in the quick postoperative interval and repeated at 6-month intervals for no much less than 2 years. Davies and coauthors found no variations in major main assisted, and, secondary patency rates between scientific (69%, 76%, and 80%) and duplex (67%, 76%, and 79%) surveillance of vein grafts regardless of a better incidence of stenosis in the clinical group (19% vs. The majority of lesions detected by duplex surveillance by Tinder and Bandyk367 have been asymptomatic, progressed in severity on subsequent scans, and amenable to therapy with endovascular techniques. The finding of low graft circulate throughout intraoperative evaluation or at a scheduled surveillance examine predicts failure, and if associated with an occlusive lesion, a graft revision can delay patency The. A peak systolic velocity 300cm/s and peak systolic velocity ratio across the stenosis greater than 3. Recently Shrikhande and colleagues questioned the validity of the aforementioned criteria for tibial bypasses and advised a velocity ratio of larger than 2. However, tibial graft stenoses accounted for under a small number of the lesions evaluated and validation of these findings await the outcomes of research with bigger numbers of sufferers undergoing tibial bypasses. Johnson and coauthors,371 using intraoperative duplex scanning, detected lesions requiring revision in 15% (96/626) of infrainguinal bypasses. The lesions detected included eighty two vein/anastomotic stenoses, 17 vein segments with platelet thrombus, and 5 low-flow grafts. The revision fee was highest for arm and lesser saphenous vein bypass grafts (27%) in contrast with reversed saphenous vein bypass grafts (10%); nonreversed translocated saphenous vein (13%) and in situ saphenous vein bypass grafts (16%). Ferris and associates372 found that despite normal completion angiography early graft velocity abnormalities could possibly be, detected in 26% of 224 grafts. Fifty-two percent of these lesions required correction, 38% resolved, and the remaining lesions have been revised at a later date. When conducted appropriately a graft surveillance program should reduce the incidence of sudden, graft failure to lower than 3% per 12 months. Reoperation to correct such defects before graft occlusion permits salvage of the grafts and prevents recurrent ischemia. Unfortunately between 20% and 40% of grafts occlude with out warning or with, recently recorded normal ankle strain indexes.
Complementary distal arteriovenous fistula and deep vein interposition: a five-year experience with a brand new approach to enhance infrapopliteal prosthetic bypass patency J Vasc Surg arthritis center of north georgia buy 400 mg etodolac visa. Alterations in wall shear stress predict sites of neointimal hyperplasia after stent implantation in rabbit iliac arteries arthritis back neck pain buy generic etodolac 400 mg on line. Mis-sizing of stent promotes intimal hyperplasia: influence of endothelial shear and intramural stress arthritis hand gloves 400 mg etodolac order otc. Influence of residual stenosis after percutaneous coronary intervention with stent implantation on improvement of restenosis and stent thrombosis. The position of low endothelial shear stress in the conversion of atherosclerotic lesions from secure to unstable plaque. Platelet-derived progress factor gene expression in human atherosclerotic plaques and normal artery wall. Production of platelet-derived progress factor-like mitogen by smooth-muscle cells from human atheroma. Sunitinib, a small-molecule receptor tyrosine kinase inhibitor, suppresses neointimal hyperplasia in balloon-injured rat carotid artery J Cardiovasc Pharmacol Ther. Promoting endothelial restoration and decreasing neointimal hyperplasia utilizing sequential-like release of acetylsalicylic acid and paclitaxel-loaded biodegradable stents. Acceleration of re-endothelialization and inhibition of neointimal formation utilizing hybrid biodegradable nanofibrous rosuvastatin-loaded stents. Association of polymorphonuclear leukocytes with sites of aortic catheter-induced harm in rabbits. Cells, cytokines and mobile immunity within the pathogenesis of fibroproliferative vasculopathies. Novel mannequin of inflammatory neointima formation reveals a possible function of myeloperoxidase in neointimal hyperplasia. Leukocyte stimulation of intimal lesion formation is inhibited by therapy with diclofenac sodium and dexamethasone. Localization of T lymphocytes and macrophages in fibrous and sophisticated human atherosclerotic plaques. The lamina adventitia is the main website of immune cell accumulation in commonplace chow-fed apolipoprotein E-deficient mice. Macrophages, myofibroblasts and neointimal hyperplasia after coronary artery damage and repair. Systemic supply of proresolving lipid mediators resolvin D2 and maresin 1 attenuates intimal hyperplasia in mice. Extracellular Vesicles Derived from Adipose Mesenchymal Stem Cells Regulate the Phenotype of Smooth Muscle Cells to Limit Intimal Hyperplasia. Vascular response to basic fibroblast growth factor when infused onto the traditional adventitia or into the injured media of the rat carotid artery Circ Res. Syndecan-4 deficiency limits neointimal formation after vascular injury by regulating vascular smooth muscle cell proliferation and vascular progenitor cell mobilization. Overexpression of reworking progress issue beta1 in arterial endothelium causes hyperplasia, apoptosis, and cartilaginous metaplasia. Antibodies against transforming growth factor-beta 1 suppress intimal hyperplasia in a rat mannequin. Ribozyme oligonucleotides in opposition to reworking growth factor-beta inhibited neointimal formation after vascular injury in rat model: potential utility of ribozyme strategy to treat cardiovascular disease. A morphologic and permeability examine of luminal smooth muscle cells after arterial harm in the rat. Studies on plasminogen activator and different proteases in subcultured human vascular cells. Nitric oxide-generating vasodilators and 8-bromo-cyclic guanosine monophosphate inhibit mitogenesis and proliferation of cultured rat vascular clean muscle cells. Transfection of inducible nitric oxide synthase gene causes apoptosis in vascular clean muscle cells. Adenoviral transfer of the inducible nitric oxide synthase gene blocks endothelial cell apoptosis. Endothelium-derived stress-free issue produced and launched from artery and vein is nitric oxide. Nitric oxide launch accounts for the biological exercise of endothelium-derived stress-free issue. Direct evidence for the significance of endothelium-derived nitric oxide in vascular transforming. Pharmacologic inhibition of nitric oxide synthases and cyclooxygenases enhances intimal hyperplasia in balloon-injured rat carotid arteries. Essential position of endothelial nitric oxide synthase for mobilization of stem and progenitor cells. Estrogen-mediated, endothelial nitric oxide synthase-dependent mobilization of bone marrow-derived endothelial progenitor cells contributes to reendothelialization after arterial damage. Nitric oxide-dependent bone marrow progenitor mobilization by carbon monoxide enhances endothelial restore after vascular damage Circulation. Control of accelerated vein graft atheroma with the nitric oxide precursor: L-arginine. Inhibition of neointimal proliferation in rabbits after vascular harm by a single treatment with a protein adduct of nitric oxide. Chronic inhalation of nitric oxide inhibits neointimal formation after balloon-induced arterial harm Circ Res. Polymeric-based perivascular supply of a nitric oxide donor inhibits intimal thickening after balloon denudation arterial harm: position of nuclear factor-kappaB. Adenovirus-mediated gene switch of human inducible nitric oxide synthase in porcine vein grafts inhibits intimal hyperplasia. Nitric oxide-generating polymers cut back platelet adhesion and smooth muscle cell proliferation. Perivascular supply of a nitric oxide donor inhibits neointimal hyperplasia in vein grafts implanted in the arterial circulation. Nitric oxide-releasing biopolymers inhibit thrombus formation in a sheep mannequin of arteriovenous bridge grafts. Efficacy of native molsidomine supply from a hydrogel-coated angioplasty balloon catheter within the atherosclerotic porcine model. Local effects of nitric oxide supplementation and suppression within the improvement of intimal hyperplasia in experimental vein grafts. Local supply of gene vectors from baremetal stents by use of a biodegradable synthetic complicated inhibits in-stent restenosis in rat carotid arteries. Efficient inhibition of intimal hyperplasia by adenovirus-mediated inducible nitric oxide synthase gene transfer to rats and pigs in vivo. Gene remedy inhibiting neointimal vascular lesion: in vivo transfer of endothelial cell nitric oxide synthase gene. Insights into the effect of nitric oxide and its metabolites nitrite and nitrate at inhibiting neointimal hyperplasia. Nitric oxide and nanotechnology: a novel approach to inhibit neointimal hyperplasia. Nitric oxide delivery through a permeable balloon catheter inhibits neointimal growth after arterial harm J Surg. Targeted Nitric Oxide Delivery by Supramolecular Nanofibers for the Prevention of Restenosis after Arterial Injury. Ephrin type-B receptor four activation reduces neointimal hyperplasia in human saphenous vein in vitro. Basic mechanisms of oxidative stress and reactive oxygen species in cardiovascular harm Trends Cardiovasc Med. Regulation of reactive oxygen species by p53: implications for nitric oxide-mediated apoptosis. Adventitial fibroblast reactive oxygen species as autacrine and paracrine mediators of reworking: bellwether for vascular disease Correlation of modifications in nitric oxide synthase, superoxide dismutase and nitrotyrosine with endothelial regeneration and neointimal hyperplasia in the balloon-injured rabbit subclavian artery Coron Artery Dis.
In all cases rheumatoid arthritis specialist new zealand purchase 200 mg etodolac with visa, the risks and advantages of using lytic remedy within the therapy of patients with graft limb occlusions must be evaluated fastidiously rheumatoid arthritis diet recipes free 400 mg etodolac generic otc. The relatively low incidence of issues arthritis joint deformity etodolac 200 mg order line, improved technique of administration, and efficacy of thrombolytic brokers have reduced the necessity for urgent surgical thrombectomy in sufferers with noncritical limb ischemia. Successful lytic therapy readily identifies the reason for the graft limb occlusion and should enable a less in depth repair. In addition, lytic remedy could cut back the risk of wound and graft problems and scale back the incidence of reperfusion edema and compartment syndrome related to extensive redo procedures. Mechanical Thrombectomy Mechanical thrombectomy units that theoretically permit speedy revascularization of an ischemic extremity utilizing minimally invasive techniques are gaining in reputation The. These units may be categorized broadly into (1) aspiration thrombectomy catheters that remove the thrombus by steady handbook suction through a large-lumen aspiration catheter; (2) pull-back thrombectomy catheters that withdraw the thrombus with a balloon catheter or basket into a trapping device, allowing the clot to be removed; (3) recirculation thrombectomy gadgets that ablate the thrombus by hydrodynamic vortices, which pulverize the thrombus into microscopic fragments; (4) nonrecirculation thrombectomy units, which macerate the thrombus mechanically into fragments that are larger than those produced by recirculation catheters; and (5) energyassisted devices that use ultrasound, laser, or radiofrequency to lyse the thrombus or enhance the results of pharmacologic agents. The most extensively studied gadget is the AngioJet rheolytic thrombectomy system, which is accredited for peripheral arterial and coronary functions. The major remedy limitation of those gadgets is their lack of efficacy in opposition to organized thrombotic or embolic material. Protruding atheromas of the aortic arch and descending aorta have assumed increasing significance as potential websites for embolization throughout catheter manipulation within the aorta for cardiac catheterization, carotid stenting placement of thoracic endografts, or bypass surgery a hundred and ten Embolization may also occur spontaneously. Evidence of spontaneous embolization has also been demonstrated at autopsy studies, but the incidence seems to be low (0. Intraoperative Embolism Variable amounts of atherothrombotic materials may be dislodged and carried to a downstream territory as a consequence of manipulation throughout arterial dissection and clamp placement. Larger emboli lodging in major vessels can normally be retrieved with a balloon thrombectomy catheter. This could also be a minor and self-limited drawback, or it could produce extensive gangrene of all of the digits and the forefoot, leg, buttocks, and barely the abdominal wall. Careful evaluate of preoperative imaging studies will determine the location of clamp placement. A number of technical maneuvers has been used to forestall or minimize operative embolization. The proximal clamp could need to be placed at the degree of the diaphragm if the pararenal phase of the aorta appears to be concerned. The lumen of the aortic prosthesis must be totally aspirated to take away blood and debris after testing the proximal suture line, and efforts ought to be made to stop the accumulation of blood inside the prosthesis while distal iliac or femoral anastomoses are being carried out. Vigorous antegrade flushing of the proximal vessel and retrograde flushing from the distal arteries as the earlier few stitches are being positioned in an anastomosis, earlier than the restoration of circulation, is the most reliable maneuver to be certain that retained debris and clot are effectively removed. Minor patchy areas of cyanosis or necrosis can be observed, with spontaneous recovery anticipated. Whether intensive lipid-lowering statin remedy for 3 to 6 months before surgery in sufferers at recognized threat of embolization will show helpful is presently unknown. The major consequences are important reduction in coronary perfusion, which can promote myocardial injury especially in sufferers with significant coronary artery disease, and, temporary renal ischemia, which can contribute to renal failure. Prevention is preferable to remedy after a hypotensive insult has already occurred and depends on sufficient hydration and efficient restoration of intravascular quantity through the process, and especially earlier than clamp release. The extent of intravascular depletion is directly related to the length of intraperitoneal and retroperitoneal exposure during surgery. The most dependable information to making certain adequate quantity replacement without circulatory overload is using a Swan-Ganz catheter to monitor left-heart filling pressures and myocardial efficiency. The arterial pressure have to be constantly observed whereas blood move is slowly restored to the extremities by gradual release of the clamps until full flow could be tolerated without hypotension. Acute renal harm manifested by the incidence of, albuminuria (93%) and proteinuria (22%) in sufferers undergoing aortic surgery is the, mildest type of impairment. Albuminuria usually happens earlier than cross-clamping and peaks between zero and 6 hours after declamping. A contributing issue is renal cortical vasospasm produced by infrarenal application of the aortic clamp, which stimulates the renin-angiotensin mechanism. Renal artery obstruction may be produced by displacement of huge atherosclerotic plaques, thrombus, or dissection on the orifices of the renal arteries when an aortic clamp is applied. Myoglobinemia can occur after restoration of circulation to limbs which have been severely ischemic for an prolonged interval. Although the implications of ischemic damage to the kidney are complex, harm to the tubules, particularly the S3 segment of the proximal tubule and the thick ascending limb of the loop of Henle, is central to the event of oliguria. Central filling pressures must be monitored perioperatively to be positive that volume alternative is optimal in relation to cardiac output and myocardial performance. Chylous Ascites Chylous ascites, issuing from a broken cisterna chyli and its tributaries on the root of the mesentery is a rare complication of aortic reconstruction and efficiency of a, Warren shunt. Chylous ascites may find yourself in nutritional imbalance, immunologic deficit, and respiratory dysfunction. Abdominal paracentesis reveals a milky, fluid, with a high lymphocyte rely and lipid content material, which is bacteriologically sterile. Leakage of ascites to the outside via a defect in the incision increases the fluid and protein loss and heightens the chance of infection. Such a leak must be repaired surgically or laparoscopically under sterile situations and prophylactic antibiotic protection. The reliability of these checks in identifying the location of the leak or fistula remains unestablished. Whether the use of octreotide or fibrin glue accelerates the decision of ascites remains unclear. When the neurologic deficit was complete initially, involving each sensory and motor function, 76% of the patients died; there were solely two full neurologic recoveries and one partial recovery By contrast, when the initial. The major explanation for spinal twine ischemia is interruption of move by way of the great radicular artery of Adamkiewicz, which is the main source of supply to the anterior spinal artery at the decrease finish of the cord. The anterior spinal artery itself is long and has quite poor collateral contributions from the posterior spinal arteries or from the radicular arteries derived from more proximal intercostal vessels. Because the spinal cord is just tenuously supplied in its decrease portion by vessels other than the good radicular artery embolization or harm to this vessel, during aortic reconstruction might lead to some extent of twine infarction. The effectiveness of collateral pathways could additionally be additional compromised by hypotension, especially in patients with ruptured aneurysms; prolonged clamp placement; ligation or occlusion of the hypogastric, lumbar, or sacral arteries; and retrograde dissection from the aortic anastomosis occluding intercostal arteries. Monitoring of somatosensory evoked potentials during thoracic surgery has been proven to correlate with wire ischemia. Practical software of this system to belly aortic surgery is undergoing continued investigation. Suturing a patch of posterior aortic wall with its intercostal vessel orifices right into a window cut out of the graft has been really helpful for thoracoabdominal aneurysms. When ischemic injury to the spinal wire is clinically evident postoperatively therapy, 216 is supportive. Several drugs, including steroids, rosuvastatin, cilostozol, angiotensin ll receptor blockade, and oxygen-free radical scavengers, are being investigated to restrict the extent of, or stop neurologic injury after, aneurysm repair. Thorough data of the anatomic relationships of the ureters at the stage of the iliac bifurcation is essential. Sometimes, a quantity of ureters may be current or they could be in an aberrant place, owing to congenital anomalies. Direct damage to the ureter can finest be averted by preserving the dissection close to the iliac artery on the level the place the ureter normally crosses the widespread iliac bifurcation in transit to the bladder. This is especially important through the blind improvement of the retroperitoneal tunnel for aortofemoral bypass. The ureter must be elevated away from the iliac vessels so that the graft will lie dorsal to it. Inadvertent passage of the graft ventral to the ureter could trigger it to be compressed between the graft limb and the underlying iliac artery producing hydroureter and hydronephrosis. The incidence of, ureteral obstruction after aortic grafting in a single prospective research was 2%. The right ureter must be carefully protected throughout retroperitoneal closure because this construction can easily be caught up in the suture line. Iatrogenic ureteral injuries sustained throughout placement or revision of a vascular graft should be repaired primarily Although renal. Once acknowledged, placement of a percutaneous nephrostomy tube may be associated with a shorter hospital keep and decrease an infection rate than with open repair. Ureteral obstruction is believed to be extra widespread when the limb of the graft is tunneled anterior to the ureter. However, hydronephrosis secondary to anterior graft placement occurs in only 30% of cases. The majority of sufferers have a clinical presentation inside 1 year of the procedure, however delayed presentation as a lot as 14 years has been reported.
A special case is that of children with acute lymphoblastic leukemia involving the testis arthritis in knee and fluid purchase etodolac 200 mg on line. Radiation therapy with doses of 20 to 25 Gy arthritis knee muscle pain purchase etodolac 300 mg mastercard, either alone or with chemotherapy does arthritis in dogs come on suddenly 300 mg etodolac purchase free shipping, causes irreversible harm to Leydig cells and induces hyalinization of seminiferous tubules. Patients expertise azoospermia and hypogonadotropic hypogonadism with low serum testosterone level. In addition, radiation induces dense interstitial fibrosis and lack of peritubular cells, thus obscuring the border between the interstitium and tubules. This makes the tubules tough to identify in hematoxylin and eosin�stained sections. Ischemia secondary to radiation-induced vascular injury additionally contributes to hyalinization. Tumors of the central nervous system are the most typical strong malignancy in the pediatric population. Cranial irradiation is frequently used as a therapeutic modality in these youngsters. Complete restoration requires 9 to 18 months after irradiation of 1 Gy, 30 months after publicity of 2 to three Gy, and 5 years or extra after exposure of! Similarly, irradiation of iliac or inguinal lymph nodes for Hodgkin disease or other forms of lymphoma exposes the testes to approximately 5 Gy. Use of cytotoxic chemotherapy is associated with a broad variety of opposed unwanted effects, together with gonadotoxicity. The prepubertal testis is very vulnerable, probably due to the steady turnover of early germ cells that undergo spontaneous degeneration earlier than the haploid stage is reached. Chemotherapeutic agents kill rapidly proliferating cells, differentiating spermatogonia, and stem cells. In addition, stem spermatogonia that do survive fail to differentiate, resulting in permanent infertility. Combination chemotherapy makes it difficult to confirm which specific agent is liable for azoospermia and Leydig cell dysfunction. Comparative research of chemotherapy for acute lymphoblastic leukemia, extragonadal solid tumors, Hodgkin disease, Ewing sarcoma, and other gentle tissue sarcomas in children and pubertal boys have shown that alkylating agents (chlorambucil, cyclophosphamide, and melphalan) trigger essentially the most severe testicular injury. Seminiferous epithelium is essentially the most susceptible cell sort to the detrimental results of this chemotherapy. This agent acts directly on the spermatogenic stem cells, and restoration is determined by the variety of surviving cells. Puberty might progress, even throughout therapy, and the adult testis might show a Sertoli cell�only pattern. Combinations of chemotherapy medication heighten the unfavorable effects on testicular perform. Procarbazine, used alone to treat Hodgkin disease, causes permanent azoospermia in 30% of sufferers; however, when combined with mustine, vincristine, and prednisolone, it causes 97% of male sufferers to turned permanently sterile. Newer protocols with totally different drugs and doses are constantly introduced to cut back gonadotoxicity. Studies of young adults add negative data about fertility restoration in sufferers with cancer. Approximately 17% those that received chemotherapy are azoospermic on the preliminary analysis. The causes of this harm could also be more advanced than increased catabolic state, malnutrition, or increase in stress hormones and decrease in gonadotropic levels. Advances in assisted reproductive methods improve the probability of profitable pregnancy using cryopreserved spermatozoa. Opioids used for pain administration inhibit gonadal function and cause hyperprolactinemia. Risk for subfertility may be categorized in accordance with the kind of malignancy and the associated therapy (Table 12. High risk for growth of subfertility is associated with total physique irradiation, localized radiation remedy both within the pelvic or testicular area, chemotherapy conditioning for bone marrow transplant, alkylating agent�based remedy in Hodgkin disease, and treatment of metastatic sarcoma. In the latter group, cross-sex hormone treatment is a prerequisite for sex reassignment surgery. The testicular parenchyma reveals combined atrophy with one seminiferous tubule with Sertoli cell�only pattern and Sertoli cells of adult sort and the opposite two tubules with spermatogenesis. In patients with gender dysphoria changing from male to female, testicular adjustments have been studied in bilateral orchiectomy specimens after sex reassignment surgery. Tubules turn out to be hyalinized and peritubular cells enhance, whereas Leydig cells might disappear,3335,3338 decline or increase in number, or stay unchanged. The seminiferous tubules comprise isolated spermatogonia and dedifferentiated Sertoli cells with spherical nuclei, small nucleoli, and pseudostratified infantile distribution. In 72% of instances, spermatogenesis is pubertal-like, with seminiferous tubules containing Sertoli cells and spermatogonia only, or spermatogonia and primary spermatocytes, as the only germ cells. Sertoli cell�only tubules in sufferers handled with estrogens contain dedifferentiated Sertoli cells. A correlation exists between the degree of Sertoli cell dedifferentiation and the dose and timing of remedy with estrogens or antiandrogens. Brief treatment induces germ cell loss and inconspicuous Sertoli cell modifications, and as a lot as Surgery Sexual perform is commonly adversely affected in patients who bear bilateral retroperitoneal lymph node dissection for nonseminomatous testicular most cancers. Up to 90% lose antegrade ejaculation, although libido, erection, and orgasm are regular. Loss of antegrade ejaculation outcomes from elimination of or damage to sympathetic ganglia and the hypogastric nervous plexus throughout surgical procedure. Unilateral surgery, particularly if limited to the right side, and trendy nervesparing techniques reduce this complication by preserving antegrade ejaculation and fertility. Infertility in Patients With Spinal Cord Injury Spinal wire harm is frequent, with more than 10,000 new circumstances yearly in the United States, predominantly involving young adults. Major sexual dysfunctions in these sufferers embody lack of erection and ejaculation and poor semen quality. Most of those males reveal faulty seminal emission as properly (entrance of semen into the posterior urethra). Semen could additionally be obtained via vibratory stimulation of the penis or electroejaculation in more than 90% of instances, but high quality is low, with increased variety of useless spermatozoa, markedly low motility, and decreased fertilization rate. Compared with controls, semen in these sufferers has considerably increased numbers of neutrophils and macrophages, and markedly greater ranges of reactive oxygen species. Possible etiologies embody increase in testicular temperature resulting from vascular dilation or alteration in scrotal thermoregulation secondary to impaired sympathetic innervation from extended wheelchair restraint; alteration in sperm transport secondary to nerve injury that results in sperm stagnation in seminal vesicles, a hostile environment that normally is devoid of spermatozoa; and abnormal composition of seminal fluid with consequent deterioration of spermatozoa that, within the epididymis and ductus deferens, had good motility. The inflammatory infiltrate of the testicular interstitium has two characteristic intranuclear inclusions. Inflammation and Infection Infectious agents could attain the testis and epididymis through blood vessels, lymphatics, sperm excretory ducts, or directly from a superficial wound. Infection transmitted through the blood mainly affects the testis and causes orchitis, whereas infection ascending via sperm excretory ducts normally causes epididymitis. The tunica albuginea is covered by a fibrinous exudate, and the testicular parenchyma is yellow or brown. In some cases the infection heals with deposition of granulation tissue and fibrosis; in others, infection might persist as an lively process, resulting in chronic orchiepididymitis. The tubular lining is destroyed, leaving behind solely hyalinized tubules and clusters of Leydig cells. A group of tubules with complete spermatogenesis surrounded by completely hyalinized tubules could also be observed. If an infection is bilateral, the patient normally becomes infertile, with extreme oligozoospermia or azoospermia, though biopsy could reveal the presence of mature spermatids in some tubules, thus allowing sperm extraction for paternity. Occasionally, testicular harm is so severe that testicular endocrine operate is impaired, inflicting hypergonadotropic hypogonadism, with low testosterone level and regression of secondary intercourse characteristics. Gross image of the testis displaying congestion and separation of lobules by intense edema. Inflammatory infiltrate as microabscesses instantly associated to seminiferous tubules. Seminiferous tubules and interstitium with histiocytes displaying microvacuolated cytoplasm. Small fragments of testicular parenchyma could also be eradicated by way of the scrotal skin, a situation identified clinically as fungus testis. Specific causes might require particular stains, cultures, or serologic exams and include tuberculosis, syphilis, leprosy, brucellosis, mycoses, and parasitic diseases.
Pokeberry (Pokeweed). Etodolac.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96251
Nodular hyperplasia usually includes the transition zone arthritis medication for dogs metacam 300 mg etodolac purchase, however sometimes nodules arise from the periurethral tissue on the bladder neck lemons arthritis relief generic etodolac 400 mg on line. Microscopically arthritis knee lung cancer etodolac 300 mg discount overnight delivery, nodular hyperplasia consists of various proportions of epithelium and stroma (fibrous connective tissue and easy muscle). It accommodates small, thick-walled blood vessels embedded in spindle cell proliferation. There are four kinds of pure stromal nodules: (1) immature mesenchymal (5% of stromal nodules); (2) fibroblastic (50%); (3) fibromuscular (36%); and (4) easy muscular (10%) varieties. A focus of adenocarcinoma varieties an ill-defined mass within the peripheral zone on the decrease proper of the specimen. Note the dilated peripheral sinus that types the boundary of the nodule with the transition zone stroma. This sinus usually goes in and out of the airplane of section and should seem incomplete. The transition zone is sometimes sampled by needle biopsies until the urologist specifically targets this area or large hyperplasia compresses the peripheral zone. We require the presence of no much less than part of a nodule for the diagnosis of nodular hyperplasia in needle biopsies, a very unusual discovering. Narrow 18-gauge needle biopsies nearly by no means comprise the entire nodule unless it is rather small and fortuitously sampled. Vascular insufficiency most likely accounts for infarction of hyperplastic nodules, seen in up to 20% of resected circumstances. The heart of the nodule undergoes hemorrhagic necrosis, usually with reactive adjustments within the residual epithelium on the periphery, together with squamous metaplasia and urothelial metaplasia. Both require androgens for development and development, and both could respond to androgen deprivation treatment. Inflammation is usually present in both, thus suggesting a possible causative link. Nodular hyperplasia could also be associated to most cancers arising within the transition zone, maybe in association with certain forms of hyperplasia. It is possible that nodular hyperplasia has no single mechanism, however somewhat represents a synergistic effect of a quantity of occasions inside biologic communication systems (neural, endocrine, and immune systems) during getting older. There is an elevated variety of neuroendocrine cells in small adenomas, and the number of cells decreases as nodules enlarge, suggesting a job at inception of nodular hyperplasia. One or more bigger dilated acini are normally current inside round to oval clusters. The small acini seem to bud off from the dilated acinus and impart a lobular look to the lesion. The small acini are lined by a layer of cuboidal secretory cells with mildly enlarged nuclei with an increased nuclear-to-cytoplasmic ratio compared with adjoining benign epithelial cells. Nuclei comprise evenly distributed and finely granular chromatin, and nucleoli are normally small, although mildly enlarged basophilic nucleoli are focally present in 39% of circumstances. The cytoplasm is commonly basophilic or finely granular to clear, and luminal cytoplasmic apocrine-like blebs are present in 33% of instances. In cases with sclerosis the acinar lumina are compressed and present marked distortion. The separation from carcinoma is most tough in needle biopsy specimens during which solely a portion of the lesion is sampled, and consciousness of this entity assists on this distinction. Part of the epithelium is flattened, indicating atrophy, however different areas present low cuboidal epithelium and luminal secretory blebs. Prostatic Stromal Hyperplasia With Atypia Prostatic stromal hyperplasia with atypia consists of one or more illdefined, uncircumscribed, hyperplastic stromal proliferations, generally nodular, with variable numbers of atypical, weird giant cells, with vacuolated nuclei, smudged chromatin, and frequent multinucleation infiltrating around benign acini. Most cells comprise a reasonable amount of eosinophilic cytoplasm with indistinct cellular borders. Prostatic stromal hyperplasia with atypia is a uncommon lesion that has been referred to by quite a lot of terms, together with atypical stromal hyperplasia, stromal hyperplasia with weird nuclei, pseudosarcomatous lesion, and pseudoneoplastic lesion of the prostate gland. These findings suggest that this lesion outcomes from native hypersensitivity to androgen, with upregulation of androgen receptors in these cells. Stromal hyperplasia with atypia has no malignant potential, and the atypical cells are degenerative myofibroblasts. Architecture, low energy Lobular small acinar proliferation, often with central massive dilated acini or acinus Irregular, "atrophic" Basal Cell Hyperplasia and Basal Cell Proliferations There are three patterns of basal cell hyperplasia: typical basal cell hyperplasia, atypical basal cell hyperplasia, and basal cell adenoma (Table eight. Multinucleated big cells punctuate the stroma, with average cytologic atypia with out mitotic figures. The nests could additionally be strong or cystically dilated, and occasionally are punctuated by irregular spherical luminal spaces, making a cribriform sample. The proliferation might protrude into the acinar lumen and retain the overlying secretory luminal epithelium. Basal cell hyperplasia resembles prostatic acini in the fetus, and this characteristic accounts for the synonyms fetalization and embryonal hyperplasia. Basal cell hyperplasia could also be composed of basal cell nests with areas of luminal differentiation resembling comparable lesions of the salivary gland (so-called adenoid basal form of basal cell hyperplasia). The basal cells in basal cell hyperplasia are enlarged, ovoid or round, and plump (epithelioid), with giant, pale, ovoid nuclei, finely reticular chromatin, and a average amount of cytoplasm. Nucleoli are normally inconspicuous (<1 m in diameter) besides in atypical basal cell hyperplasia (discussed later). Sclerosing basal cell hyperplasia is identical to typical basal cell hyperplasia except for the presence of delicate lacy fibrosis or dense irregular sclerotic fibrosis and hyperplastic easy muscle surrounding and distorting hyperplastic mobile aggregates. Clear cell change is frequent in basal cell hyperplasia, often with a cribriform pattern; a cribriform pattern with out clear cell change is rare. Focal calcification is evident in some circumstances and may be present throughout the basal cell nests (Table 8. No mitotic figures were noticed in both of these cases regardless of exhaustive sectioning. The proliferation of basal cells involves more than a hundred small crowded acini (per section) forming a nodule. The nucleoli are round to oval and flippantly eosinophilic, like these seen in acinar adenocarcinoma of the prostate (mean diameter is 2 m). Chronic inflammation occurs in most cases, a finding suggesting that nucleolomegaly reflects reactive changes. A morphologic spectrum of nucleolar size is noticed in basal cell proliferations, and only these with greater than 10% of cells exhibiting prominent nucleoli are thought of atypical. Basal cell adenoma consists of one or more large, round, normally solitary circumscribed nodules of acini with basal cell hyperplasia in the setting of nodular hyperplasia. Condensed stroma is seen on the periphery, often traverses the adenomatous nodules, and creates incomplete lobulation in some cases. Stroma is regular or barely increased in density and may be basophilic without myxoid change adjacent to cell nests. The basal cells in adenoma are plump, with massive nuclei, scant cytoplasm, and inconspicuous nucleoli, although massive distinguished nucleoli are not often observed. Compare with (F) "strong" pattern of basal cell hyperplasia, with absence of lumen. Atypical basal cell hyperplasia of the prostate: immunophenotypic profile and proposed classification of basal cell proliferations. Basal cell adenoma invariably arises in association with nodular hyperplasia and seems to be a variant with no malignant potential. In distinction with basal cell carcinoma, adenoma is well circumscribed, lacks necrosis, and the stroma between the basal cell nests is like that of the encompassing benign stroma. Immunohistochemical Findings Basal cell hyperplasia (typical and atypical forms) displays intense cytoplasmic immunoreactivity in virtually all cells with keratin 34E12 and p63 (Table eight. Differential Diagnosis the differential diagnosis of basal cell proliferations includes all kinds of benign and malignant lesions (Table 8. The proliferation and stratification of lining cells with cytologic atypia might resemble small foci of stable basal cell hyperplasia. Seminal vesicle epithelium is distinguished by the presence of secretory luminal cells, vital cytologic atypia (particularly within the senile seminal vesicle), and distinctive abundant yellow to golden-brown lipochrome pigment.
There are three patterns of seminal vesicle invasion: (1) direct spread along the ejaculatory duct complicated into the seminal vesicles; (2) prostatic capsular perforation adopted by extension into the periprostatic delicate tissues and unfold into the seminal vesicles; and (3) isolated deposits of most cancers in the seminal vesicles (see Chapter 9) arthritis diet help 400 mg etodolac cheap fast delivery. Mucosal involvement by in situ urothelial carcinoma is uncommon arthritis with dogs discount etodolac 300 mg amex, present in solely 1% of instances coping with arthritis in back discount 200 mg etodolac with mastercard. The cysts are grossly multiloculated, ranging in size from 5 to 15 cm in diameter. The density and cytologic options of the stroma determine whether the tumor is a fibroadenoma, low-grade phyllodes tumor, or high-grade phyllodes tumor (cystosarcoma phyllodes). Heterologous differentiation was not apparent histologically or ultrastructurally, although desmin reactivity was observed in 30% of the stromal cells, significantly within the looser myxoid regions, suggesting muscular differentiation. At excessive magnification (B), the stromal cells display various levels of cytologic atypia. These tumors develop locally and compress adjoining pelvic organs such as the prostate, bladder, and rectum. Other malignant delicate tissue tumors of the seminal vesicle include angiosarcoma, fibrosarcoma, and rhabdomyosarcoma. Primary choriocarcinoma was reported in a 28-year-old, forming a hemorrhagic 12-cm diameter mass; at post-mortem the testes had been normal on serial sectioning, and no different main website was found. Immunohistochemical identification of practical relationships within the accessory sex glands. The affiliation between seminal vesicle size and period of abstinence from ejaculation. Seminal vesicle epithelium as a potential pitfall within the cytodiagnosis of presacral plenty. A potential research to consider sexual dysfunction and enlargement of seminal vesicles in sexually lively males handled for benign prostatic hyperplasia by alpha blockers. Normal human ejaculatory duct anatomy: a research of cadaveric and surgical specimens. Prostate-specific antigen expression and lipochrome pigment granules within the differential diagnosis of prostatic adenocarcinoma versus seminal vesicle-ejaculatory duct epithelium. Seminal vesicle parameters at 10year intervals measured by transrectal ultrasonography. Relationship between volume of the seminal vesicles and sexual exercise in middle-aged males. Aneuploidy in benign seminal vesicle epithelium: an instance of the paradox of ploidy research. Cytologic options of seminal vesicle epithelium in aspiration biopsy smears of the prostate. Seminal vesicle epithelium in fine-needle aspiration biopsies of the prostate as a pitfall within the cytologic analysis of carcinoma. Cells from ejaculatory ducts and seminal vesicles and diagnostic difficulties in prostatic aspirates. Analysis of the prostatic central zone in patients with unilateral absence of wolffian duct structures: further proof of the mesodermal origin of the prostatic central zone. Ureteral ectopia into cystic seminal vesicle with ipsilateral renal dysgenesis and monorchia. Hydrospermatocyst with ectopic junction of the ureter and ipsilateral renal agenesis. Renal dysplasia related to ureteral ectopia and ipsilateral seminal vesicle cyst. Seminal vesicle cyst associated with renal agenesis and ipsilateral ectopic ureter. Seminal vesicle cyst related to ipsilateral renal agenesis: case report and evaluate of literature. Cyst of seminal vesicle with ipsilateral renal agenesis and ectopic ureter: case report. Right renal agenesis and ureter ectopic abouchement in cystic dilation of seminal vesicle. Multicystic seminal vesicle with ipsilateral renal agenesis: two instances of Zinner syndrome. Unusual variant of inverted Y ureteral duplication with an ipsilateral seminal vesicle cyst and renal dysgenesis. Magnetic resonance imaging of seminal vesicle cyst related to ipsilateral urinary anomalies. Congenial seminal vesicle cyst with an intracystic papillary adenoma associated with ipsilateral renal agenesis. Complete resolution of a big seminal vesicle cyst-evidence for an obstructive aetiology. A uncommon retrovesical hydatid cyst and value of transrectal ultrasonography in diagnosis: a case report and evaluation of the literature. Benign ectopic prostatic tissue involving the seminal vesicle in a patient with prostate cancer: recognition and implications for staging. A seminal vesicle cyst sophisticated with a tumor like nodular mass of benign proliferating prostatic tissue: a case report with ultrastructural and immunohistochemical research. Ectopic prostate: case report of a presacral mass presenting with obstructive signs. Prostate most cancers arising in ectopic prostatic tissue inside the left seminal vesicle: a rare case identified with multi-parametric magnetic resonance imaging and magnetic resonance imaging-transrectal ultrasound fusion biopsy. Prostatic glands and urothelial epithelium in a seminal vesicle cyst: report of a case and evaluation of pathologic features and prostatic ectopy. Seminal tract amyloidosis: synchronous amyloidosis of the seminal vesicles, deferent ducts and ejaculatory ducts. Beitrag zur kenntis der para-amyloidose in urogenitalen system unter besonderer berucksichtigung der sog senilen amyloidose in den samem blaschen und ihres verhaltnisses zum samenblaschen-pigment. Characterization of localized seminal vesicle amyloidosis inflicting hemospermia: an evaluation utilizing immunohistochemistry and magnetic resonance imaging. Immunohistochemical detection of lactoferrin and amyloid of the prealbumin-transthyretin type. Seminal vesicle amyloidosis: morphological, histochemical and immunohistochemical observations. Seminal vesicle amyloid: the first example of exocrine cell origin of an amyloid fibril precursor. Localized amyloidosis of seminal vesicles: report of three instances in surgically obtained material. A case of multifocal fibrosclerosis involving posterior mediastinal fibrosis, retroperitoneal fibrosis, and a left seminal vesicle with elevated serum IgG4. Primary seminal vesicle abscess: prognosis and therapy by transrectal ultrasound. Seminal vesicle abscess: the use of computerized coaxial tomography for diagnosis and therapy. Sanchez Chapado M, Angulo Cuesta J, Guil Cid M, Lera Fernandez R, Dehaini A, Prieto Chaparro L. Cytomegaloviral inclusions detected in the seminal vesicle, ductus deferens and lungs in an post-mortem case of lung most cancers. Calcification of the vas deferens: its relation to diabetes mellitus and arteriosclerosis. Case report: endoscopic management of seminal vesicle stones with cutaneous fistula. The usefulness of Pax8 immunohistochemical expression for the differential analysis. Papillary adenocarcinoma in a seminal vesicle cyst associated with ipsilateral renal agenesis: a case report. Carcinosarcoma of the prostate in combination with adenocarcinoma of the prostate and adenocarcinoma of the seminal vesicles. Primary squamous cell carcinoma of seminal vesicle: a particularly uncommon case report with literature evaluation. Histogenesis of induced prostate and seminal vesicle carcinoma in Lobund-Wistar rats: a system for histological scoring and grading. Seminal vesicle intraepithelial neoplasia versus basal cell hyperplasia in a seminal vesicle.
Globular Mallory-like our bodies in renal cell carcinoma: report of a case and evaluate of cytoplasmic eosinophilic globules rheumatoid arthritis natural treatment etodolac 300 mg trusted. Myelinoid lamellated cytoplasmic inclusions in human renal adenocarcinomas: an ultrastructural examine arthritis in back from car accident generic etodolac 400 mg amex. Utility of cytokeratin 7 for distinguishing chromophobe renal cell carcinoma from renal oncocytoma arthritis neck va disability etodolac 200 mg low price. Cytokeratin 7: a helpful adjunct in the prognosis of chromophobe renal cell carcinoma. Cytokeratins 7 and 20 immunoreactivity in chromophobe renal cell carcinomas and renal oncocytomas. The diagnostic utility of immunohistochemistry in distinguishing between mesothelioma and renal cell carcinoma: a comparative examine. Keratin immunohistochemistry in renal cell carcinoma subtypes and renal oncocytomas: a systematic analysis of 233 tumors. Expression profiling of renal epithelial neoplasms: a method for tumor classification and discovery of diagnostic molecular markers. The usefulness of immunohistochemical markers in the differential prognosis of renal neoplasms. Immunohistochemistry within the evaluation of renal cell carcinoma: a crucial appraisal. Renal cell carcinomas with papillary structure and clear cell parts: the utility of immunohistochemical and cytogenetical analyses in differential analysis. Renal cell carcinoma with rhabdoid features: an aggressive neoplasm with overexpression of p53. Extensively cystic renal neoplasms: cystic nephroma, cystic partially differentiated nephroblastoma, multilocular cystic renal cell carcinoma, and cystic hamartoma of renal pelvis. Multilocular cystic renal cell carcinoma: a collection of 12 cases and evaluate of the literature. Multilocular cystic renal cell carcinoma: a clinicopathological, immuno- and lectin histochemical research of 9 cases. Multilocular cystic renal cell carcinoma: a report of forty five circumstances of a kidney tumor of low malignant potential. Cystic partially regressed clear cell renal cell carcinoma: a possible mimic of multilocular cystic renal cell carcinoma. Multilocular cystic renal cell carcinoma is a subtype of clear cell renal cell carcinoma. Multilocular cystic renal cell carcinoma: similarities and variations in immunoprofile in contrast with clear cell renal cell carcinoma. Prognostic impact of histologic subtyping of grownup renal epithelial neoplasms: an experience of 405 circumstances. Prevalence of microscopic tumors in regular appearing renal parenchyma of sufferers with hereditary papillary renal cancer. Hereditary and sporadic papillary renal carcinomas with c-met mutations share a distinct morphological phenotype. Allelic loss at the D9S171 locus on chromosome 9p13 is associated with development of papillary renal cell carcinoma. Molecular genetic proof for the unbiased origin of multifocal papillary tumors in patients with papillary renal cell carcinomas. Bilateral multicentric papillary renal tumors with heteroclonal origin primarily based on tissue-specific karyotype instability. Papillary renal cell carcinoma: a clinicopathologic and immunohistochemical research of 105 tumors. Papillary renal cell carcinoma with low-grade spindle cell foci: a mimic of mucinous tubular and spindle cell carcinoma. Solid variant of papillary renal cell carcinoma with spindle cell and tubular parts. Morphologic typing of papillary renal cell carcinoma: comparison of development kinetics and patient survival in sixty six cases. Prognostic worth of morphological subtypes in a clinicopathologic examine of forty three instances. Gains of chromosomes 7, 17, 12, sixteen, and 20 and loss of Y happen early within the evolution of papillary renal cell neoplasia: a fluorescent in situ hybridization examine. The morphologic and immunohistochemical spectrum of papillary renal cell carcinoma: examine including 132 circumstances with pure type 1 and kind 2 morphology in addition to tumors with overlapping options. Cytogenetic and molecular tumor profiling for sort 1 and kind 2 papillary renal cell carcinoma. Dismantling papillary renal cell carcinoma classification: the heterogeneity of genetic profiles suggests a quantity of unbiased diseases. Prognostic factors for the survival of patients with papillary renal cell carcinoma: meaning of histological typing and multifocality. Toward biological subtyping of papillary renal cell carcinoma with medical implications through histologic, immunohistochemical, and molecular analysis. Clinical and pathological options associated with prognosis in patients with papillary renal cell carcinoma. Adult papillary renal tumor with oncocytic cells: clinicopathologic, immunohistochemical, and cytogenetic features of 10 circumstances. Integrated phenotypic/ genotypic evaluation of papillary renal cell carcinoma subtypes: identification of prognostic markers, cancer-related pathways, and implications for therapy. Papillary renal cell carcinoma with oncocytic cells and nonoverlapping low grade nuclei: increasing the morphologic spectrum with emphasis on clinicopathologic, immunohistochemical and molecular options. Oncocytic papillary renal cell carcinoma with inverted nuclear pattern: distinct subtype with an indolent clinical course. Histological subtype is an impartial predictor of outcome for patients with renal cell carcinoma. Reappraisal of morphologic differences between renal medullary carcinoma, collecting duct carcinoma, and fumarate hydratase-deficient renal cell carcinoma. Molecular pathways: Fumarate hydratase-deficient kidney cancer-targeting the Warburg impact in most cancers. Hereditary leiomyomatosis and renal cell carcinoma syndrome-associated renal cancer: recognition of the syndrome by pathologic features and the utility of detecting aberrant succination by immunohistochemistry. Familial cutaneous leiomyomatosis is a two-hit situation associated with renal cell cancer of characteristic histopathology. Hereditary leiomyomatosis and renal cell cancer: a syndrome associated with an aggressive form of inherited renal cancer. Fumarate hydratase-deficient renal cell carcinoma is strongly correlated with fumarate hydratase mutation and hereditary leiomyomatosis and renal cell carcinoma syndrome. Tubulocystic carcinoma of the kidney with poorly differentiated foci: a frequent morphologic pattern of fumarate hydratase-deficient renal cell carcinoma. Risk of renal and colonic neoplasms and spontaneous pneumothorax in the Birt-Hogg-Dube syndrome. Prognostic implications of histological options in patients with chromophobe cell renal carcinoma. Chromophobe renal cell carcinoma: an immunohistochemical research of 21 Japanese cases. Chromophobe renal cell carcinoma: a comparative examine of histological, immunohistochemical and ultrastructural options using high throughput tissue microarray. Sarcomatoid renal cell carcinoma: an examination of underlying histologic subtype and an analysis of associations with patient outcome. Renal cell neoplasms of oncocytosis have distinct morphologic, immunohistochemical, and cytogenetic profiles. Sporadic hybrid oncocytic/chromophobe tumor of the kidney: a clinicopathologic, histomorphologic, immunohistochemical, ultrastructural, and molecular cytogenetic research of 14 instances. Birt-Hogg-Dube renal tumors are genetically distinct from different renal neoplasias and are associated with up-regulation of mitochondrial gene expression. Subtypes of chromophobe cell renal carcinoma: an ultrastructural and histochemical examine of thirteen instances. A case of chromophobe renal cell carcinoma associated with low chromosome quantity and microsatellite instability. Polyploidization and losses of chromosomes 1, 2, 6, 10, thirteen, and 17 in three circumstances of chromophobe renal cell carcinomas. Specific lack of chromosomes 1, 2, 6, 10, 13, 17, and 21 in chromophobe renal cell carcinomas revealed by comparative genomic hybridization.






