Nexium
Nexium
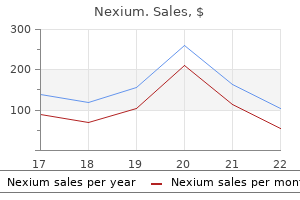
Nexium dosages: 40 mg, 20 mg
Nexium packs: 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Laparoscopic pyloromyotomy for hypertrophic pyloric stenosis: a potential gastritis diet ���2 buy nexium 20 mg cheap, randomized controlled trial gastritis diet emedicine nexium 20 mg buy mastercard. Open versus laparoscopic pyloromyotomy for pyloric stenosis: a potential gastritis diet kits nexium 40 mg order on-line, randomized trial. The long-term aim is to preserve a level of weight discount which improves or eliminates obesityrelated comorbidities and reduces the danger of future obesity-related medical issues and dying. This convention concluded that there was insufficient data to make recommendations about bariatric surgery for patients <18 years of age. For this cause, present opinion holds that bariatric surgery must also be an choice for extremely chosen adolescents with excessive weight problems. Recent greatest follow tips have been developed for pediatric/adolescent weight reduction surgical procedure. These new tips more intently mimic those for grownup surgical procedure than in earlier years. Physical maturity should be documented by either history and bodily examination or radiographic study, thus generally limiting surgery to these over the age of 12 years. Minimally invasive bariatric surgical procedure is probably one of the most technically troublesome operations to carry out. Expertise in minimally invasive surgical procedure could not confer the same level of expertise in performing minimally invasive bariatric surgical procedure. Surgeons performing bariatric procedures have to be properly skilled as instructed by the American Society for Bariatric Surgery, American College of Surgeons, and the Society of American Gastrointestinal Endoscopic Surgeons. Prior to performing laparoscopic bariatric operations, surgeons must meet all native credentialing requirements for the performance of open bariatric procedures and advanced laparoscopic operations. Given the controversy centered on adolescent bariatric surgical procedure, the aspiring adolescent bariatric surgeon, at a minimal, ought to take a course in bariatric surgical procedure and perform his or her first five to ten procedures proctored by an skilled laparoscopic bariatric surgeon. Various producers supply the gear required and the choice of 1 over one other is basically a matter of surgeon desire. Information in regards to the surgical process, various operations and the rationale for the operation to be performed, postoperative care, and the considerable life-style modifications required afterwards have to be conveyed verbally and in writing to the patient and caregivers. The adolescent and parents should show understanding of the details of the process, its identified and potential dangers, and predictable consequences, and that understanding must be reflected in the archived responses to a written check. The referring pediatrician might want to turn into conversant in the anatomic and physiologic changes that occur after operation and develop an understanding of frequent postoperative issues to effectively partner with the surgeon in the care of the affected person for years following the operation. Thus, the experienced laparoscopic bariatric surgeon can perform this operation with out another educated bariatric surgeon as an assistant. The two different 12-mm and as much as two 5-mm trocar placement websites and the 5-mm subzyphoid site for liver retraction are proven. Exposure of the small bowel is optimized if the desk is positioned into slight Trendelenburg position and the omentum is tucked rigorously beneath the liver edge. The transverse mesocolon is grasped with a locking grasper just anterior to the duodenojejunal flexure and elevated anteriorly. The Roux limb is generally introduced as a lot as the pouch within the antecolic fashion, this requires a minimum of 50 cm to comfortably attain the pouch in the epigastrium. The mesentery is minimally divided at this level utilizing either half the length of a second stapler load or the Harmonic scalpel. Next, a single keep suture is positioned to approximate the antemesenteric borders of the distal end of the biliopancreatic segment (the proximal jejunum) and the purpose one hundred fifty cm distal to the top of the roux limb. The Harmonic scalpel is used to make opposing enterotomies which are spread extensive sufficient with a grasper to settle for the stapler jaw. A side-to-side jejunojejunostomy is created using the 60-mm Echelon stapler with white load. The mesenteric defect is next closed with a operating 2-0 silk suture to avoid an internal hernial orifice. In the antecolic technique, the omentum must be draped back inferiorly, and often bivalved up to the transverse colon, to reduce the bulk of tissue that the roux limb will traverse. This omental division additionally reduces the tension (and thus risk of stricture) transmitted from the Roux limb to the anastomosis when the patient assumes an erect posture postoperatively. This dissection is continued posteriorly in close proximity to the gastric wall till the aircraft practically reaches the lesser sac behind the stomach. The higher curvature of the stomach is next elevated and a skinny space of the gastrocolic ligament is chosen for entry into the lesser sac, utilizing the Harmonic scalpel. Numerous posterior attachments between the lesser curve and retroperitoneum are divided to obtain continuity between the lesser curve dissection, which was performed anteriorly. A tubular lesser curve pouch is next created utilizing the Echelon 60-mm stapler with multiple blue masses. Once in place across the lesser curve, the stapler is fired creating the inferior most margin of the pouch. Next, light dissection is carried out at the apex of the staple line to fully break into the retrogastric lesser sac from above. This easy maneuver is important since the procedure is far more easy if the lesser sac is identified and entered from the anterior aspect at this point. Counter-traction is important to ensure that the complete stapler head is within the lumen. Gentle traction is utilized below the proposed anastomosis to be sure that no stray tissue is within the last anastomosis. The stapler is then closed, fired, then faraway from the port site with the anvil intact. One should check to make certain that two separate donuts of tissue are contained within the stapler complicated at its inspection. The integrity and patency of the anastomosis is assessed laparoscopically with intraluminal air insufflation under saline. Two 12-mm and three 5-mm trocars are utilized for the procedure and positioned via a similar manner as previously described. A 34 Fr orogastric tube is positioned by anesthesia at the beginning of the case and placed on suction to aid within the dissection. The higher omentum is then carefully dissected away from the larger curvature of the abdomen at this level till the lesser sac is entered. The 34 Fr orogastric tube aids in the identification of the esophagus and the left crus throughout this portion of the procedure. The assistant is invaluable during this dissection, offering traction and counter-traction, given the often massive measurement of the stomach in these cases. The 34 Fr orogastric tube is then positioned into the antrum and along the lesser curvature of the abdomen to act as a information for the rest of the procedure. The remainder of the stapler fires are carried out sequentially alongside the 34 Fr orogastric tube (adjacent to the lesser curvature of the stomach) with the Echelon 60-mm stapler, blue hundreds with Gore Seamguard Bioabsorbable Staple Line Reinforcement. This does go away a small triangular portion of stomach on the superior aspect of the resection margin, but ensures that the esophagus remains free from the staple line. This maneuver might probably decrease the incidence of leaks at this website given the relative proximity of the skinny esophageal tissue. One 15-mm, one 12-mm, and two 5-mm trocars are used to carry out this process and are placed as beforehand described within the arrangement illustrated. A 5-mm blunt endoscopic dissector (supplied within the Realize pack) is used, by way of the pars flaccida approach by way of the lesser omentum, to create a tunnel behind the superior portion of the abdomen near the esophagogastric junction. Blunt dissection continues gently alongside the best crus to enable passage utterly beneath the abdomen. The band is then rotated so that the buckle will eventually lie alongside the lesser curvature of the abdomen. Rarely, a portion of the anterior paraesophageal fats pad (generally by the Harmonic scalpel) needs to be taken all the method down to permit for proper placement. This not solely permits for adequate visualization of the fascia for port placement, but in addition locations the port in the identical position each time to permit for easier identification for access within the clinic. The injector port is then attached to the tubing and transfixed to the fascia by an intrinsic staple gadget or by non-absorbable suture. They are cared for in a monitored, non-intensive care unit setting, and maintenance fluids are administered based upon lean physique weight (typically 40�50 % of precise weight).
The mixture of aortic and mitral disease normally takes the form of predominant mitral stenosis and predominant aortic regurgitation but some aortic stenosis gastritis drugs cheap nexium 40 mg on-line. In trivalvular rheumatic disease gastritis diet ������ best nexium 20 mg, the lesions of the aortic and mitral valves are typically similar to gastritis symptoms night sweats 40 mg nexium those observed when only the left-sided heart valves are affected. Involvement of the tricuspid valve is universally related to enlargement of the proper atrium. In the compensated heart with mitral valve illness and a traditional tricuspid valve, the best ventricle could also be of normal dimension. In patients with multivalvular disease in whom the aortic valve additionally participates with the mitral valve, the left ventricle is hypertrophied, but significantly less than noticed in sufferers with isolated aortic valvular illness. Of 99 sufferers with main amyloidosis, 92 confirmed severe involvement of the heart. The clinician ought to contemplate the analysis of amyloidosis of the guts when persistent, intractable heart failure develops in a affected person age 50 or older, significantly if the guts failure remains unexplained, even in the presence of the usual signs and signs. Murmurs typical of valvular illness could be detected only if the valves are affected by depositions of amyloid. Cardiac ultrasound with Doppler imaging typically reveals a restrictive cardiomyopathy. Cardiac biopsy and staining with Congo red confirm the analysis of amyloidosis of the guts by demonstrating apple-green birefringence beneath polarized gentle. Electron microscopic research of homogeneous amyloid reveal delicate fibers thought to be liable for the impact of the green birefringence. On cardiac biopsy, microscopic homogeneous deposits of amyloid are translucent and refract the sunshine strongly (see Plate 6-60). The myocardial fibers are compressed and often are atrophied to very flat fibers with pinlike nuclei. The pseudomyocardial hypertrophy explains the insufficiency of each coronary heart chambers. Rarely, as a end result of obstruction of a coronary artery by nodular deposits of amyloid, infarction or disseminated necroses of the myocardium could occur. Secondary typical or systemic amyloidosis happens in ailments with chronic irritation and extreme tissue necrosis, especially chronic tuberculosis of the lungs or different organs. Other main underlying ailments are bronchiectasis, empyema of the pleural cavities, continual osteomyelitis, and tumors, as properly as leprosy, syphilis, and echinococcosis (hydatid disease). Deposits of amyloid may be discovered within the blood vessels and in relation to myocardial fibers of the myocardium of elderly persons with out underlying illness. Newborns, nursing mothers, and patients with previous viral infection are predisposed, as are diabetic and severely burned sufferers. Diagnosis and treatment of septic myocarditis rely upon tradition of the myocardial strains. Dense colonies of bacteria throughout the dilated capillaries and veins are the earliest detectable finding in microscopic sections of the myocardium (see Plate 6-61). The surrounding myocardial fibers can reveal homogeneous cytoplasm with unstained or pyknotic nuclei. When the heart is sectioned at post-mortem, myocardial abscesses are sometimes visible as small yellow factors or stripes, measuring 1 or 2 mm, beneath the thin endocardium of the best ventricle (see Plate 6-61). The irregular and bizarre formation of the abscesses is usually decided by the anatomic course of the Mastoiditis Tonsillitis, septic sore throat Carbuncle Cardiac catheterization Staphylococcal enteritis Omphalitis Appendicitis Peritonitis Septic endometritis Surgical wound infection Hand an infection Osteomyelitis Major foci of origin Abscess in coronary heart muscle. Subendocardially located abscesses can perforate into the ventricular lumen and cause bacterial endocarditis. Frequently, the major focus often could be detected simply, such as after perforation into the pericardial sac, however in a couple of circumstances it may be impossible to discover. Microorganisms (viruses, rickettsiae, micro organism, protozoa) or their toxins can produce myocarditis. Decreasing blood strain, arrhythmias, and complete heart block could precede acute heart failure. Microscopically, the myocardial fibers are swollen and show a dustlike fatty degeneration. The secondary inflammatory reactions are frequently arranged focally but also could also be diffuse. In the encompassing areas of toxic necrosis, circulatory disturbances also might develop, leading to further necrosis. The protracted shock finally affects the coronary blood supply in such a way that additional disseminated hypoxic necrosis happens. Myocarditis could be preceded by meningitis, encephalitis, pleurisy, hepatitis, and pericarditis, in addition to gastrointestinal symptoms. Except for dilatation of both ventricles, the myocardium appears macroscopically unchanged. In the third stage, interstitial accumulations of lymphocytes, plasma cells, and histiocytes are the predominant options. These third-stage changes are noticed most regularly in sections of the myocardium and the conduction system at autopsy. In sarcoidosis the lungs, liver, spleen, and lymph nodes are involved far more incessantly and extensively than the center (see Plate 6-63). At first the myocarditic foci include perivascular accumulations of histiocytes. The recurrent course of the disease could result in diffuse fibrosis of the myocardium. Some consultants hypothesize that cardiac sarcoid is expounded to an abnormal immune response to environmental components. More than one case of sarcoidosis can be observed in families or in siblings, for reasons nonetheless undetermined. The focal myocardial lesions consist primarily of lymphocytes and histiocytes (see Plate 6-63). In later phases, perivascular interstitial fibrosis progresses, and scarring extends diffusely all through the myocardium. Initially, the disease is characterized by edema and erythema of the pores and skin, followed by hardening and atrophy. As remnants of myocardial fibers, large cells with numerous nuclei may also be current. However, as lengthy as the etiology of granulomatous myocarditis with big cells stays unclear, ultimate classification is still unresolved, although the illness is believed to be brought on by T lymphocytes. The prognosis of big cell myocarditis often could be made at cardiac biopsy and at post-mortem. Clinical examination reveals an enlarged coronary heart, with passive congestion of the lungs and belly organs. A prognosis of large cell myocarditis is justified only if different causes of cardiac failure. Idiopathic myocarditis often takes a fast, deadly course and sometimes is called pernicious myocarditis. A raised firm ridge marks the junction of the inflow and outflow areas, greatest seen in the left ventricle. The unscarred part of the endocardium might show a gentle opacification from elastomyofibrosis. Lesions could also be focally distributed in the inflow space, and the areas of preference are the apex and the site behind the posterior cusp of the A-V valve; the cusp adheres to the mural endocardium. The A-V valves exhibit no particular lesions, and the semilunar valves are entirely unaffected. On the best side, the ventricular configuration leads to filling and obliterating the ventricular cavity with a mass of thrombus and organizing fibrous tissue. Beneath the thickened endocardium, there are small blood lagoons-dilated thebesian veins-and from these and the endocardial scar tissue, tongues of fibrous tissue extend into the internal third or half of the myocardium, but never involve its full thickness. The main coronary vessels are regular; no changes are seen within the minor vessels aside from an occasional small focus of inflammatory cells and, in late levels when fibrosis is severe, an obliterative arteritis. Severe calcification may develop in the valve or mural endocardium, which is important radiologically, indicating that the constriction is endocardial, not pericardial, although a big pericardial effusion may be present. The heart weight could additionally be elevated but is usually lowered, and despite the voluminous atria, the ventricles often are small and shrunken. The disease could also be biventricular, and the clinical manifestations could change depending on which ventricle is most diseased. Patients have high Characteristic recession of right apex, forming bizarre notch: enlargement of right atrium Dense collagen layer lining left ventricle, involving posterior papillary muscle and chordae tendineae, demarcated by a ridge, sparing outflow tract; posterior mitral cusp adherent to wall; mural thrombi central venous strain and may show exophthalmos.
In the unoxygenated myocardium gastritis diet management nexium 20 mg line, and when the fibrillations are of poor quality gastritis for dogs order nexium 40 mg free shipping, defibrillation will not be attainable gastritis chronic nausea nexium 40 mg purchase line. Once spontaneous cardiac motion has been resumed, cardiac function is supported by vasopressor medicine, as needed. Wide-spectrum antibiotics are left within the pleural house, and the patient is given massive doses of intravenous antibiotics for 1 week. Electrodes lubricated with electrode paste; one placed over base of coronary heart at first proper intercostal area, and one over apex just below left nipple; each pressed firmly against chest wall. After 10 minutes of mind anoxia, with out defibrillation, about 10% of sufferers will survive and go away the hospital, many with residual cognitive impairment. Prompt defibrillation in any affected person with cardiac arrest from ventricular fibrillation is the remedy of alternative. In a affected person who has been defibrillated and is unconscious, prompt defibrillation followed by hypothermia might assist protect brain operate by reducing ischemic damage related to decreased blood flow to the brain. Current resuscitation suggestions support the utilization of hypothermia protocols after defibrillation, and proof supports its benefit in sufferers with ventricular fibrillation because the preliminary rhythm. To accomplish hypothermia in these patients requires an organized method by emergency department physicians and the cardiologists liable for care of those critically compromised patients on hospital admission. Protocols to decrease body temperature must be rapidly implemented and maintained for roughly 24 hours. Patient temperature must be lowered to a goal 32� to 34� C (~90� F) and drugs to control shivering administered. After 24 hours the affected person must be rewarmed slowly, to avoid complications such as hypotension and hyperkalemia. Central space of fibrinoid necrosis surrounded by zone of palisading mesenchymal cells and peripheral fibrous tissue capsule containing chronic inflammatory cells. Low-dose methotrexate is being tested with ischemic heart illness patients to assess the efficacy and safety of utilizing an antiinflammatory agent to lower main antagonistic cardiovascular occasions. Distinctive features at post-mortem embody thickening of the aortic wall caused by adventitial scarring, as well as intimal proliferation limited to the aortic root (ascending aorta) however extending into the membranous ventricular septum. In some, ultrasonic detection of aortic regurgitation could precede development of joint manifestations. Confirmation by cardiac ultrasound is troublesome, and the aortic root dilatation could outcome from aortic regurgitation. First-degree atrioventricular block is the most typical conduction system disease, though extra serious A-V blocks as well as right and left bundle-branch blocks can occur as well. Treatment of patients with ankylosing spondylitis is mostly received poorly, although tumor necrosis factor- antagonists may have a task. The inflammatory cellular infiltrates are sometimes composed of T cells and macrophages. More than half of myositis patients died of disease issues inside 5 years earlier than steroids were out there; since then, a large percentage of patients survive past 5 years. Conduction abnormalities could lead to symptomatic bradycardia brought on by complete coronary heart block. Coronary artery manifestations extra usually contain the microcirculation rather than the epicardial arteries. Difficulty in moving into bus or in climbing stairs Edema and heliotrope discoloration around eyes a classic signal. The most specific autoantibodies found in sufferers with systemic sclerosis are antinuclear antibodies. Scleroderma is a symmetric thickening, tightening, and induration of the pores and skin of the fingers and the pores and skin proximal to the metacarpophalangeal or metatarsophalangeal joints; (sclerodactyly). Digital pitting scars, lack of substance within the finger pad, and pulmonary fibrosis of the lung bases are part of the medical picture (see Plate 6-94). Myocardial disease in systemic sclerosis could additionally be multifactorial, associated to related pulmonary or renal involvement or hypertension. These findings doubtless had been related to the development of congestive coronary heart failure, conduction abnormalities, ventricular arrhythmias, and cardiovascular demise. Thus, left ventricular regional wall motion abnormalities and impaired coronary move reserve in sufferers without epicardial coronary stenoses can happen. Fibrosis with formation of microcysts, a lot of which symbolize dilated bronchioles Grossly sectioned lung. Inflammation and microvascular disease end in stiffening of the conduit arteries. Prognosis in systemic sclerosis is worsened by the presence of cardiac involvement. Therapy typically is poorly acquired in sufferers limited by cardiovascular problems of systemic sclerosis. The mitral and tricuspid valves are most incessantly affected by single or mulberry-shaped excrescences 1 to 4 millimicrons in measurement and happen randomly, both on and away from the road of closure and on each surfaces of the valve as properly as on the chordae tendineae, papillary muscle tissue, and mural endocardium, often on the base of the ventricles. Microscopically, the excrescences have a superficial layer of partially hyalinized platelet and fibrin thrombi. Endothelial proliferative and granular plugs of fibrin occlude the lumen of small vessels, displaying necrosis of the wall. Infiltrations of neutrophils in the acute stage and mononuclear cells within the older lesions are outstanding. Fluorescent antibody assay demonstrates deposits of gamma globulin and the C3 complement within the acute vascular lesion (Plate 6-95, B). In the late levels of vessel involvement, endothelial proliferation, thickening, and partial occlusion could additionally be found. Foci of myocardial irritation related to interstitial edema and eosinophilic degeneration of collagen could additionally be prominent (Plate 6-95, C). The cardiac manifestations of acromegaly include hypertension, concentric left ventricular hypertrophy, valve dysfunction, and systolic/diastolic ventricular dysfunction (see Plate 6-97). Coronary artery disease is probably associated with the high incidence of hypertension and diabetes in acromegalic patients and could also be unrelated to hormonal abnormalities. As the pituitary adenoma expands, acromegalic patients typically experience headache and abnormalities related to cranial nerve defects, such as strain on the optic chiasm leading to a bitemporal hemianopsia or different visible subject defects. Ventricular hypertrophy may lead to diastolic dysfunction, leading to coronary heart failure symptoms with preserved ejection fraction. Patients with acromegaly could have an elevated potential for arrhythmias, together with ectopic beats, paroxysmal atrial fibrillation, paroxysmal supraventricular tachycardia, sick sinus syndrome, ventricular tachycardia, and bundle branch blocks. Systolic blood pressure usually rises, diastolic pressure drops and pulse pressure will increase. Atrial fibrillation, typically paroxysmal, is particularly common in sufferers older than 40 (see Plate 6-97). Chest radiographs could present average cardiac enlargement and a prominent pulmonary artery. The hemodynamic adjustments in thyrotoxic sufferers outcome from the general enhance in metabolic price, higher sensitivity to catecholamines, and direct impact of thyroid hormones on the guts. The enhanced cardiac index outcomes from accelerated coronary heart price and elevated stroke volume. The hemodynamic modifications occur and not utilizing a vital variation in stress in the right atrium or the pulmonary artery. Flow to the pores and skin and muscle tissue improves, but with no improve in cerebral or splanchnic move. The additional renal blood move parallels the final increase in oxygen consumption. The affected person with earlier coronary artery illness may develop angina pectoris underneath the burden of this cardiac workload. Similarly, with rheumatic valvular deformity, congestive heart failure might supervene. The normal coronary heart may eventually fail as the results of elevated cardiac work of lengthy duration (tachycardiainduced cardiomyopathy). The stroke index falls, the response to train is poor, and proper atrial and pulmonary artery pressures are elevated.
The perineal body is reconstructed gastritis symptoms child nexium 40 mg with mastercard, bringing together the anterior limit of the sphincter chronic gastritis x ray buy discount nexium 40 mg on-line. A lengthy widespread wall between the vagina and the bladder exists gastritis and nausea quality 40 mg nexium, and both the ureters run through this frequent wall. The surgeon have to be conversant in the totally different techniques of ureteral reimplantation as a outcome of these sufferers may require this operation during the procedure. Once in the abdomen, the patency of the M�llerian buildings may be confirmed by passing a No. When both M�llerian constructions are atretic, we suggest leaving them in place, and following the patient intently so that a call may be made about them when she reaches puberty. The process continues with the location of traction sutures within the single uterus or in each hemiuteri. This dissection is continued all the way in which down to meet the earlier dissection initiated from below. Vaginal substitute the vagina may be augmented or completely changed with bowel when it is extremely small and is located very high, or in circumstances of absent vagina. The blood supply of the rectum might be provided transmurally from branches of the inferior mesenteric vessels. Colon 18 Ped51-18 19a Ped51-19a 19a,b When small bowel is chosen for reconstruction, probably the most mobile portion is utilized. The mesentery of the small bowel is longer in an space approximately 15 cm proximal to the ileocecal valve. A phase of this portion of the small intestine is selected, preserving its mesentery. The blood supply of the hemivagina of that facet is sacrificed, that of the contralateral hemivagina is preserved and is adequate for both hemivaginas. The vaginal septum is resected, and both hemivaginas are tubularized right into a single vagina, benefiting from their combined lengthy lateral dimension. This is a superb maneuver, but it could solely be performed when the anatomic traits fulfill the requirements described. At that time, the surgeon should have enough experience to decide about whether to reconstruct the bladderneck or to shut it permanently. In the second situation (permanent closure of the bladderneck), a vesicostomy is created, and the affected person will require a continent diversion-type of procedure at the age of urinary continence (between three and four years of age). Ped 51-23 23 comPlIcatIons urethrovaginal fistula Urethrovaginal fistula used to be the most common and feared complication in cases of persistent cloaca, however with the appearance of the total urogenital mobilization maneuver, this complication has essentially been eliminated. Patients with common channels longer than 3 cm will require intermittent catheterization 70�80 p.c of the time. Prophylactic antibiotics are administered orally to avoid urinary tract infections whereas the catheter is in. Most sufferers go residence after 2 days, or after 3�4 days for many who required a laparotomy. The mixture of an excellent bladderneck and a floppy, flaccid bladder makes these sufferers best candidates for intermittent catheterization, which keeps them fully dry. The initial method consists of the restore of the omphalocele, closure of the bladder (primarily or staged) with or with out osteotomies, and the creation of an end colostomy utilizing all out there colon. Only after determining the potential for bowel control should a urological reconstruction be deliberate. Laparoscopy has also been utilized by several authors for chosen forms of cloacal malformations, in order to consider the intraabdominal anatomy and to carry out mobilization of pelvic constructions. Some authors advocate the laparoscopic approach for all excessive anorectal malformations, and imagine that outcomes are better with this strategy. In children with high anorectal malformation without a fistula, the choice ought to be made based on the extent of the rectal atresia. The umbilicus is everted and a 5-mm longitudinal incision is performed through the skin. It is important to determine the ureters and the vas deferens bilaterally to keep away from harm to these constructions in the course of the rectal dissection. Opening the rectal fistula to establish the place of the urethra can generally be helpful. The area from the apex of the pubococcygeus muscle extending posteriorly is identified and developed. The 12-mm perineal port, grasper, and rectum are gently pulled caudally, delivering the rectum by way of the sphincter advanced to the perineal skin. Pull via tract 7 Pubococcygeus Postoperative care 543 the belly cavity and pelvis are inspected laparoscopically for hemostasis, the pneumoperitoneum is launched, and all the ports are removed. The linea alba on the stage of the umbilical port is reapproximated with 2/0 Vicryl figure-of-eight suture and all the abdominal skin incisions are closed with a single horizontal mattress 5/0 chromic dermal suture. Steristrips are applied as a dressing to the abdominal incisions and polysporin to perineal incision. If it becomes necessary to substitute the catheter, this ought to be accomplished beneath radiological steering. The affected person is maintained with intravenous fluids and bowel relaxation and is initiated on an oral diet once bowel operate resumes. Once the patient has resumed a full oral food plan and is having bowel movements, or ostomy output, with out difficulty, the patient is discharged to the community and is seen once more in 2 weeks the place the neo-anus is calibrated. Once the specified neo-anus size and compliance is achieved, the dilatations are weaned. The two-stage process involves neonatal restore and creation of neo-anus as described above, adopted by the creation of a defending descending colostomy. First, the colon is commonly very dilated and stuffed with meconium, which makes it difficult to dissect. The colostomy could also be carried out in the sigmoid, descending, or transverse colon, and is normally a loop or a divided stoma. The colostomy could be done within the left lower quadrant, left upper quadrant, or through the umbilicus, and could be accomplished utilizing a small incision or with a laparoscopic method. This can be achieved most simply by acquiring a biopsy of the mucosa and, most importantly, the submucosa of the rectum. The lubricated instrument is inserted into the anus and the side hole positioned at 3 cm from the anal verge. This is the minimal distance and avoids the traditional hypoganglionic zone and diagnostic confusion. It is suggested to apply a delicate strain on to the rectal wall to be able to obtain an enough pattern. This is normally about three � 1 mm, and the crucial submucosa can be acknowledged as a particular whitish layer. The method of processing suction biopsies have to be ascertained earlier than the process, as dictated by particular laboratory requirements. However, numerous different techniques have been extensively reported within the literature and may nicely exchange its use. Postoperative care A rectal examination ought to be carried out after finishing the biopsy to exclude lively bleeding. Observations ought to be continued for no less than 2 hours, to ensure complete hemostasis. This has an prevalence rate of between 10 and 20 p.c and is largely operator dependent, although newer single-use gadgets have improved this. Although these perforations can usually be treated conservatively with antibiotics, nasogastric suction, and intravenous fluid, a laparotomy may be needed. Position the toddler is held in the lithotomy position while an older youngster might want to be placed in stirrups within the lithotomy position. Applying traction on this stay suture, the operator places an additional keep suture 2 cm higher, which is tied and the needle left intact. Technical modifications which are illustrated on this chapter have been introduced through the years. A inflexible, time-consuming routine is required postoperatively and this is a lifelong commitment.
Ramipril increases mean ache free walking time by over 200 yards in sufferers with uncomplicated diabetic gastritis diet discount nexium 20 mg without prescription, steady claudication not already taking an angiotensin-converting enzyme inhibitor or angiotensin receptor blocker gastritis diet juice 20 mg nexium discount. Exercise gastritis symptoms and home remedies order 20 mg nexium amex, especially a supervised exercise program, can improve strolling by up to 150% over 3�12 months. Revascularization, both surgical or percutaneous transluminal angioplasty, is indicated for the next: 1. After attending physical therapy for presumed spinal stenosis for 8 weeks, he reports some enchancment in his train tolerance, though he still has daily ache. An epidural corticosteroid injection supplies extra pain relief, and he is ready to proceed a strolling program. Spinal abnormality or intervention (degenerative joint disease, trauma, surgical procedure, drug injection) c. Potential local or systemic supply of infection (skin or soft tissue an infection, endocarditis, osteomyelitis, urinary tract infection, injection drug use, epidural anesthesia, indwelling vascular access) 2. Infection occurs by contiguous spread in 33% of circumstances and by hematogenous spread in 50%. Other organisms embrace Staphylococcus epidermidis, Escherichia coli, Pseudomonas aeruginosa. More widespread in posterior than anterior epidural space, and extra frequent within the thoracolumbar than cervical areas. The most essential predictor of the final neurologic consequence is the neurologic standing before surgical procedure, with the postoperative neurologic standing being as good as or better than the preoperative status. Antibiotics Vertebral Osteomyelitis Textbook Presentation the basic presentation is unremitting again ache often, but not at all times, with fever. Urinary tract, pores and skin, gentle tissue, vascular entry site, endocarditis, septic arthritis most commonly discovered sources, with endocarditis found in one-third of sufferers with vertebral osteomyelitis b. Can additionally happen because of contiguous spread from an adjoining gentle tissue infection or direct infection from trauma or surgical procedure. Generally causes bony destruction of two adjoining vertebral bodies and collapse of the intervertebral house. Found within the lumbar backbone in 58% of instances, thoracic spine in 30%, and cervical backbone in 11% b. Complicated by epidural abscess in 17% of circumstances, by paravertebral abscess in 26%, and disk area abscess in 5% B. C-reactive protein additionally elevated in nearly all sufferers, and could also be a better marker of response to therapy. Culture of a biopsy specimen is positive in about 77% of patients (range in research 47�100%). Surgery is critical provided that neurologic symptoms counsel onset of vertebral collapse causing twine compression or growth of spinal epidural abscess; surgery is at all times essential for osteomyelitis related to a spinal implant. Endocarditis should be thought-about in sufferers with both vertebral osteomyelitis or a spinal epidural abscess. Chou R, Qaseem A, Snow V et al; Clinical Efficacy Assessment Subcommittee of the American College of Physicians; American College of Physicians; American Pain Society Low Back Pain Guidelines Panel. Diagnosis and therapy of low again pain: a joint scientific follow guideline from the American College of Physicians, and the American Pain Society. Predictive value of clinical characteristics in sufferers with suspected cauda equina syndrome. Does the clinical examination predict lower extremity peripheral arterial illness Does this older adult with lower extremity pain have the scientific syndrome of lumbar spinal stenosis Office analysis of spine and limb ache: spondylotic radiculopathy and other nonstructural mimickers. A is a 24-year-old girl who involves see you because her gums are bleeding when she brushes her teeth. Bleeding because of platelet abnormalities, whether or not due to decreased quantity or abnormal operate of platelets, is usually small vessel bleeding, and produces such findings as petechiae, bruising, gum bleeding, or nosebleeds. Platelet-related bleeding is mostly not quantitatively significant (ie, platelet-related bleeding tends not to trigger severe blood loss requiring purple cell transfusions). Nonetheless, platelet-related bleeding can nonetheless be clinically essential if a patient bleeds a small amount into the brain (unusual until the platelet depend is < 10,000/mcL) or induces an belly hematoma from vigorous coughing, for instance. Bleeding because of coagulation factor abnormalities is extra prone to be quantitatively vital, generally occurring in joints, the gastrointestinal tract, mind, retroperitoneum, or at websites of recent injury or medical or surgical intervention. Abnormality of the tissue such that minor trauma causes bleeding, similar to a toothbrush causing gum bleeding from inflammatory gingival disease B. Decreased production of platelets (1) Medications (examples include valproic acid, linezolid, thiazide diuretics, gold compounds, antineoplastic chemotherapy drugs) (2) Bone marrow replacement by malignancy, fibrosis, granulomas (3) Bone marrow aplasia (4) Alcohol (5) B12 deficiency b. She notes that her final menstrual interval was considerably heavier than ordinary, and he or she has had an intermittent headache over the last 2 days, partially relieved by acetaminophen. Her oral examination shows evidence of recent gingival bleeding, and there are a couple of palatal petechiae. The second pivotal level is that her historical past further means that her platelet dysfunction is acquired. If she had a congenital platelet dysfunction, similar to von Willebrand disease, she may need had life-long heavy menses and different manifestations of bleeding. A platelet count will verify that her bleeding is said to thrombocytopenia, quite than platelet dysfunction, which is much less generally seen. A key step, then, is to determine if the thrombocytopenia is isolated or part of a pancytopenia picture, corresponding to one might encounter with acute leukemia. The platelet depend is low, with massive platelets seen on peripheral blood smear; other cell strains are normal. This is the demographic group that generally suffers from different autoimmune issues. If carried out, it might likely show regular or elevated megakaryocytes, indicating adequate platelet manufacturing and suggesting the thrombocytopenia is as a outcome of of peripheral destruction of platelets in the reticuloendothelial system. A bone marrow examination should be accomplished when the presentation is atypical: patient has splenomegaly or significant lymphadenopathy or other cytopenias or the affected person is older. In refractory instances, different immunosuppressants could additionally be used, similar to rituximab, azathioprine, or cyclophosphamide. The 5 basic manifestations are thrombocytopenia; microangiopathic hemolytic anemia; neurologic abnormalities similar to confusion, headache, lethargy, or seizures; fever; and acute kidney harm. Neurologic abnormalities are present in about two-thirds of sufferers, acute kidney harm or renal failure in about half, and fever in about one-quarter. The lack of the enzyme results in the ultra-large multimers inflicting platelet aggregation and clumping in the microcirculation, leading to thrombocytopenia. These clumps trigger red blood cells passing over them to be physically broken, resulting in the characteristic finding on the blood smear of schistocytes, or fragmented red blood cells. If neurologic signs or acute kidney injury is current, the analysis turns into even more likely. She has no different symptoms or indicators of bone marrow dysfunction, no historical past of current medicine use, and no underlying different circumstances. After 1 week, her platelet rely rises to 40,000/mcL, and after 2 weeks, to one hundred thirty,000/mcL. She then begins a prednisone taper over many weeks, and her platelet rely stays above 100,000/mcL. J is a 62-year-old man who underwent a coronary bypass graft operation 1 week in the past for extreme coronary artery illness. He has remained within the hospital for administration of a postoperative sternal wound an infection, has been doing nicely, and is scheduled for discharge later in the day. His past history is notable for an autoimmune hemolytic anemia a quantity of years in the past, successfully treated with prednisone. Therefore, the first steps in diagnosing thrombocytopenia in a hospitalized affected person are to evaluate previous platelet counts to decide whether the thrombocytopenia is new, evaluation the treatment record, and look for important signs suggestive of sepsis. Finally, he could have cirrhosis because of his intensive alcohol intake over time, with hypersplenism causing mild-to-moderate thrombocytopenia. If hypersplenism is the trigger, his platelet count at admission would most likely have been somewhat low, sometimes between 40,000/mcL and 120,000/mcL. He is receiving antibiotics for the wound infection and subcutaneous heparin each 8 hours for prophylaxis against deep venous thrombosis. There may be related thrombosis, more commonly venous (deep venous thrombosis, pulmonary embolism, venous limb gangrene) than arterial (cold digits or extremity). Caused by the development of an antibody directed towards a heparinplatelet factor four complex; the antibody occurs extra commonly with unfractionated heparin than with low-molecular-weight heparin.
Syndromes
A number of drugs diet plan for gastritis sufferers nexium 40 mg discount with mastercard, food dyes gastritis vs gerd nexium 40 mg buy generic online, and metabolites may cause heme-negative purple urine gastritis cystica profunda definition purchase 20 mg nexium with visa, or pigmenturia (Table 21-1). Spurious causes embrace urinary contamination from menstruation and sexual activity in ladies. All patients with hematuria should have a urine culture carried out, regardless of the chance of infection. The differential analysis of hematuria is usually divided into microscopic hematuria or macroscopic hematuria. Visible blood clots, that are by no means because of a glomerular trigger, are one other pivotal level, indicating a lower urinary tract supply of the hematuria. Tubulointerstitial (1) Nephrolithiasis (2) Polycystic kidney illness or medullary sponge kidney (3) Pyelonephritis (4) Acute interstitial nephritis (5) Papillary necrosis c. Vascular (1) Arterial embolus or thrombosis (2) Arteriovenous malformation or arteriovenous fistula (3) Renal vein thrombosis (4) Nutcracker syndrome (compression of left renal vein) (5) Malignant hypertension d. A reviews a quantity of episodes of painless visible hematuria over the past several days, along with occasional gentle lower stomach discomfort. He has no household history of kidney stones, however his father did have prostate cancer. External genitalia are regular, and digital rectal exam exhibits a symmetric, nontender prostate without nodules. Leading Hypothesis: Bladder Cancer Textbook Presentation Bladder most cancers classically presents as painless visible hematuria in an older male smoker. Male sex and white race: white males are 3�4 times extra prone to develop bladder most cancers than African American males or white females 2. Kidneys filter and focus metabolic toxins into the urine which pool within the bladder, promoting oncogenesis b. Compounds associated with bladder most cancers include fragrant amines, aniline dyes, nitrates, nitrites, coal, and arsenic. Occupations associated with the next danger of bladder cancer embrace miners, bus drivers, rubber workers, motor mechanics, leather-based workers, blacksmiths, machine setters, hairdressers, and mechanics. Prognosis: 10-year survival for muscle-invasive most cancers nonetheless confined to the bladder is 65�72%. Malignancy was extremely uncommon in sufferers under the age of 40 with microscopic hematuria. Macroscopic hematuria: studies generally included older patients who offered to "hematuria clinics" a. White gentle flexible cystoscopy with biopsies is the gold normal for diagnosing bladder most cancers; random biopsies of bladder tissue are taken to detect carcinoma in situ not visible to the bare eye. Hexaminolevulinate fluorescence cystoscopy is also useful for detection of carcinoma in situ. Comparatively greater sensitivity (92�100%) and specificity (94�97%) for the detection of renal lots, urinary tract stones, and genitourinary transitional cell carcinomas three. Delivers a relatively excessive radiation dose; subsequently, some guidelines advocate avoiding in low-risk patients F. Urine cytology sensitivity is 7�17% for low-grade and 53�90% for high-grade cancers; specificity is 90�98%. Patients 40 years old, or with visible urinary blood clots, require cystoscopy even if the bleeding is glomerular. Superficial or minimally invasive tumors are treated with transurethral resection for both diagnostic confirmation and remedy. Muscle-invasive tumors are handled with radical cystectomy and cisplatinbased chemotherapy. It reveals a 1 mm stone in the best renal pelvis, and a 2 cm cyst within the left kidney. Have you crossed a diagnostic threshold for the leading speculation, bladder most cancers Alternative Diagnosis: Prostate Cancer See Chapter 2, Screening & Health Maintenance. Arises from the renal epithelium and accounts for over 80% of renal cancers, with a 1. About 2% of circumstances are associated with inherited syndromes like von Hippel-Lindau illness 3. The most common histologic kind is evident cell, which accounts for 75� 85% of circumstances. Hematuria occurs with tumor invasion of the renal accumulating system, ranging from microscopic to seen blood clots. An abdominal or flank mass, generally solely palpable in skinny individuals, is often agency, homogenous, and nontender, shifting with respiration. Deciding whether or not to perform a partial or complete (radical) nephrectomy is determined by 1. A affordable alternative for individuals at excessive threat for complications from surgery is thermal ablation (eg, cryotherapy or radiofrequency ablation) D. His exam is totally normal with a notable absence of stomach ache, costovertebral angle tenderness, urethral discharge or testicular ache, and lower extremity edema. In younger sufferers (under age 40) with out threat components, cancer is an unusual explanation for asymptomatic nonvisible hematuria; in the absence of decrease urinary signs, a urologic cause is uncommon. The patient reviews no prior medical or surgical history; he has not seen a physician since his final pediatrician go to at age 18. On more detailed questioning, he does recall "three or four" earlier episodes of his urine altering color for a few days, which he associated with colds or minor respiratory infections. It can be found upon detection of asymptomatic, nonvisible hematuria with or without proteinuria throughout routine medical screening. No evidence of a job for any specific antigen despite the relation between mucosal infections and episodes of visible hematuria. One or extra episodes of seen hematuria, normally related to higher respiratory an infection (often referred to as synpharyngitic hematuria) and sometimes accompanied by flank pain and low-grade fever (present in 40�50% of patients). Nonvisible hematuria and typically mild proteinuria, detected by the way on routine screening (present in 30�40% of patients). Urine dipstick with microscopy and culture ought to be used to rule out an infection, confirm the findings of hematuria, and consider for proteinuria. A definitive diagnosis can solely be made by renal biopsy with immunofluorescence or immunoperoxidase research for IgA deposits. Proteinuria (> 500�1000 mg/day), elevated serum creatinine, or hypertension suggests extra severe or progressive illness and are indications for renal biopsy to set up the analysis. Have you crossed a diagnostic threshold for the main speculation, IgA nephropathy Characteristically presents with persistent or intermittent hematuria by the way found on routine urinalysis. Most patients have isolated hematuria, which can current at just about any age, without proteinuria or renal impairment. Renal biopsy is often not performed in sufferers with isolated hematuria, normal renal function, and no or minimal proteinuria. Historically, most circumstances have been attributed to group A streptococci, specifically Streptococcus pyogenes. Presents with hematuria, proteinuria, and edema, typically accompanied by hypertension and delicate acute kidney damage b. Characterized by low-grade proteinuria (< 1 g/day), pyuria, and nonvisible (microscopic) hematuria; typically goes undetected Evidence-Based Diagnosis A. In youngsters, nephritis typically follows pharyngitis by 1�2 weeks and pores and skin an infection by 2�4 weeks. During this time asymptomatic nonvisible (microscopic) hematuria and proteinuria is often present. The streptozyme take a look at measures all 5 of these streptococcal antibodies and performs higher than any individual antibody measurement alone. It has a sensitivity of 95% in patients with latest group A streptococcal pharyngitis and 80% in those with streptococcal skin infections. Adults current with gross hematuria and diffuse edema; proteinuria can lead to foamy urine and hypertension may cause headaches. Exam may reveal signs of an infection, corresponding to pharyngitis, pneumonia, cellulitis/abscess, endocarditis, or urethral/vaginal discharge. Older adults (25%) might have additional signs of volume overload (increased jugular venous strain, S3 gallop, pulmonary crackles, decrease extremity edema) stemming from acute volume overload precipitated by the acute kidney injury.
Usually a complication of irritation or an infection inside or adjoining to the pleural space gastritis diet gastritis symptoms buy nexium 40 mg amex, empyema hardly ever resolves spontaneously because host defenses are restricted by the anatomy and physiology of the pleural area symptoms of gastritis back pain purchase nexium 20 mg overnight delivery. However gastritis gerd diet nexium 20 mg discount on-line, infection of the chest wall or a subphrenic abscess can even result in empyema. Initially, sterile pleural fluid accumulates in the pleural space as an inflammatory response to neighboring an infection. At the end stage of illness, the pleural fluid has a pH of lower than 7 and a glucose degree of lower than forty mg/dL. Today, the preliminary treatment stays largely governed by personal expertise and coaching, hospital historical norms, and information from retrospective case collection. Instillation of fibrinolytic brokers into the pleural house for administration of a parapneumonic effusion is really helpful when the white blood cell rely within the pleural fluid is greater than 10 000/L. Illustrations 1a and 1b reveal pre- and post-therapy (one month post-therapy) plain radiographs of a patient handled successfully with fibrinolysis alone. It should be noted that radiographic improvement usually lags behind physiologic recovery. For the uncommon pediatric affected person with a hospital-acquired pneumonia, gram-negative coverage ought to be added. The skin and soft tissues about the fifth intercostal area in the mid-axillary are infiltrated with both � percent marcaine or 1 p.c lidocaine (1 cc/kg maximum). A transverse skin incision is made within the intercostal space under which the tube will move. Blunt dissection is then carried subcutaneously over the rib and into the pleural space cephalad to the rib. The tube is secured to the pores and skin with a nonabsorbable suture, and a sterile occlusive dressing with hydrophobic gauze is utilized. To this end, we make use of either double lumen endotracheal intubation or tracheal intubation with bronchial blockade. Usually, placement of the cannula in the fifth intercostal house at the mid-axillary line is an effective start line. Pleural debridement is then undertaken using a hoop forceps or Yankauer suction to remove the pleural peel and debris. Once all pockets of fluid have been drained and the majority of the pleural particles is removed, a single chest drain/tube (preferably a 19 Fr round Blake drain, if available) is inserted into the pleural space underneath direct imaginative and prescient. In addition, thoracoscopic debridement in young children may be accomplished via mini-thoracotomy with equal results. A small (3 cm) incision is situated in the mid-axillary line on the level of the fifth intercostal space. A suction device can be inserted via the mini-thoracotomy whereby loculations and debris are bluntly removed and lysed. An appropriate sized chest drain is tunneled over the ribs caudal to the incision. This tedious and meticulous dissection is facilitated by incising the peel in its thickest portion, and teasing the peel away from the lung with a Kitner or peanut type of instrument. Small areas could be lined with either fibrin sealant or observed as most will resolve spontaneously. Complicated empyema cavities in critically unwell sufferers who may not tolerate thoracoscopy or a lengthy open debridement could also be drained by rib excision and tube drainage of the cavity. This is accomplished by excising a small section of 1 to three ribs on the most dependent portion of the cavity, and inserting a large bore thoracostomy tube which is secured to the pores and skin and linked to suction initially. A postoperative chest radiograph is obtained within the recovery room to be certain that the lung has expanded utterly, and the chest drain/tube is within the appropriate position. Antibiotics are continued postoperatively for 10�14 days, and tailor-made to the microbiologic analysis of the cultured pleural fluid. A follow-up go to and chest radiograph is really helpful 3�4 weeks following discharge. Therapy of parapneumonic effusions in kids: videoassisted thoracoscopic surgery versus standard thoracostomy drainage. Randomized controlled trial of intrapleural streptokinase in empyema thoracis in youngsters. However, these conclusions are typically primarily based on comparison to historic controls, at best. In children, the commonest etiology is iatrogenic following an operation within the posterior mediastinum. Procedures on the esophagus and thoracic aorta, such as ligation of a patent ductus arteriosus, coarctation repair, and Fontan procedure, are at highest risk for this complication. Other essential causes of chylothoraces in youngsters embody superior vena cava obstruction, blunt and penetrating trauma, lymphatic malformations, malignancy, and following diaphragmatic hernia repair, particularly in the setting of right heart failure. The duct extends into the thorax by way of the aortic hiatus after which passes upward into the posterior mediastinum on the proper earlier than shifting toward the left at the degree of the fourth or fifth thoracic vertebra. It then ascends behind the aortic arch and into the posterior neck to the junction of the left subclavian and internal jugular veins. Therefore, disruption of the thoracic duct under the fifth thoracic vertebra produces a proper chylothorax. Azygos vein Diaphragm Cisterna chyli 1 226 chylothorax Any child with the suspicion of getting a chylothorax mandates an evaluation of the pleural fluid obtained by thoracentesis or tube thoracostomy. A pleural fluid cell depend larger than a thousand cells per microliter with greater than 70�90 percent lymphocytes is diagnostic for a chylothorax. Apart from the obvious respiratory embarrassment from the buildup of chyle in the pleural house, a chylothorax, even in infants, can produce a quantity of hundred milliliters of fluid per day, leading to hyponatremia, hypoalbuminemia, and immunologic derangements secondary to the lack of lymphocytes. A major cornerstone in the initial remedy of any chylothorax is full restriction of enteral consumption with the administration of intravenous alimentation. If no medical impact is seen after several days, continuous intravenous somatostatin therapy may also be helpful as an adjunct to facilitate closure of the leak. Preoperative lymphoangiograms or nuclear scintigraphy could be performed, however these studies are technically difficult to get hold of and are seldom helpful in operative planning. Lung isolation is good in thoracoscopy and thoracotomy because of the need to clearly visualize the medial facet of the posterior mediastinum. This can often be achieved by selective intubation of the contralateral mainstem bronchus. Each of those procedures may be carried out as a standalone procedure or together, depending on surgeon desire and the clinical scenario. The thoracic duct ought to be approached from the ipsilateral aspect, whereas in instances of bilateral effusion, the proper chest must be chosen initially. However, some youngsters, similar to those with vital pulmonary adhesions or extreme congenital diaphragmatic hernia, ought to be approached via a posterolateral thoracotomy, typically via the sixth or seventh interspace. This orientation of the ports allows for optimal visualization of the posterior mediastinum at the level of the diaphragm. The inferior pulmonary ligament can be divided with diathermy, if needed, to optimize exposure. On the best aspect, the thoracic duct is positioned between the azygous vein and the aorta. This must be performed no matter whether a particular space of leakage is recognized. The duct can equally be ligated cephalad to the world of leak site if one is recognized. At the conclusion of the process, a chest tube is positioned through the inferior port web site. An various strategy to pleurodesis is to instill a chemical agent, such as bleomycin, doxycycline, or talc, all of that are recognized to facilitate vital pleural inflammation. Parietal pleurectomy Pleurectomy, which involves handbook stripping of full thickness parietal pleural, is a preferred first-line method in the setting of chylothorax secondary to central venous obstruction or diffuse lymphatic leak. Pleurectomy could additionally be significantly helpful in instances the place the leak is diffuse, or is poorly identified. These shunts are much less invasive, making them perfect for top operative danger patients. The one-way pumping chamber can be positioned either externally or internally within the subcutaneous tissues depending on the size of the affected person. A lengthy atraumatic clamp is then passed from the decrease incision to the upper incision by way of the subcutaneous pocket. The peritoneal catheter is trimmed to the suitable length and inserted into the belly cavity. In these circumstances, one could consider drainage into the central venous system, by way of the interior jugular vein.
If the affected person is simply too compromised to give consent erythematous gastritis diet 20 mg nexium buy free shipping, a surrogate must be recognized based on a living will or a durable power of attorney gastritis vinegar nexium 20 mg without prescription. Cause and prognosis of cardiac arrest and the success price of resuscitation are markedly totally different when the arrest occurs in the operating room than when it occurs outside it gastritis treatment home purchase nexium 40 mg amex. However, informed consent for (or knowledgeable refusal of) medical intervention is guided by the identical ethical ideas during endof-life care, regardless of location. Just beneath the sternoclavicular joints, the cartilages of the primary ribs are attached to the sternum. The junction between the manubrium and the physique of the sternum usually varieties a prominent ridge, accentuated by the 2 elements of the sternum forming a slight angle with each other, the sternal angle of Louis. Along the inferior and inner floor of the posterior a half of each rib, a groove-the sulcus costae-affords protection to the intercostal vessels and nerve. The first rib (see Plate 1-2) may be very brief and comparatively heavier than the other ribs. On the superior floor of the first rib, two grooves are divided by a tubercle-the tuberculum scaleni-that types the purpose of insertion of the anterior scalene muscle. The groove in entrance of the muscle is occupied by the subclavian vein, whereas the subclavian artery follows the groove behind the tubercle. Each internal intercostal muscle arises from the decrease border of the rib above and runs downward and outward to insert on the higher border of the rib below. The sternohyoid and sternothyroid (see Plate 1-1) are skinny, straplike muscles that arise from the superior border and posterior surface of the sternum and insert into the hyoid bone and the thyroid cartilage, respectively. Of the deeper neck muscle tissue, the three scalene muscle tissue originate from the transverse processes of the cervical vertebrae. The parts of the cervical nerve plexus emerge from the groove between the anterior and middle scalene muscles. In this house the widespread carotid artery, inner jugular vein, and vagus nerve are enclosed in a common connective-tissue sheath; the jugular vein runs most superficially and the vagus nerve lies beneath, between the common carotid artery and internal jugular veins. On the left side the thoracic duct (see Plate 1-1) crosses over the subclavian artery and runs anteriorly to empty into the proximal subclavian vein. The inside thoracic arteries originate from the inferior surface of the subclavian arteries and run downward, lateral to , and (for a short distance) with the phrenic nerve, reaching the posterior surface of the anterior chest wall. Along their course the internal thoracic arteries give rise to branches to the thymus, mediastinum, and pericardium posteriorly; to the perforating branches to the pores and skin and subcutaneous tissues anteriorly; and finally to the lateral branches that move along the rib cartilages and anastomose with the posterior intercostal arteries. The 10 decrease intercostal veins on the proper enter the azygos vein, and the higher two intercostal veins enter either the azygos or the brachiocephalic (innominate) vein. The decrease intercostal veins on the left aspect enter the hemiazygos or accessory hemiazygos vein. The three left superior intercostal veins enter the left brachiocephalic vein by a standard stem, the left superior intercostal vein. Most of the thoracic cavity is occupied by the 2 lungs, each of which is enclosed by its pleura. That a part of the mediastinal pleura that covers the pericardium known as the pericardial pleura; the remainder (visceral pleura) covers the lung. The digital house between the visceral and parietal pleurae incorporates a tiny amount of clear fluid. The right lung consists of three lobes-the superior, middle, and inferior lobes-and is somewhat larger than the left lung, which has two-the superior and inferior lobes (see Plate 1-1). The smaller dimension of the left lung results from the eccentric place of the center, which encroaches on the left pleural cavity. Originating from the convexity of the arch, from the proximal to the distal position, are the brachiocephalic, left frequent carotid, and subclavian arteries. The left vagus nerve runs between the subclavian vein and the aortic arch, giving rise to the left recurrent nerve (see Plate 1-5), which equally loops around the arch to ascend along the trachea. Behind the trachea runs the usually collapsed esophagus (see Plate 1-4), joined by the vagus nerves simply beyond the branching off of the recurrent nerves from the vagi. Behind the esophagus, between the azygos vein and the descending aorta, the thoracic duct (see Plate 1-2) ascends, coursing behind the aortic arch to enter the neck, where it empties into the left subclavian vein. The posterior mediastinum is a shallow space containing the lower parts of the esophagus, vagus nerves, descending aorta, azygos and hemiazygos veins, thoracic duct, and sympathetic nerve chains. The remaining and largest part of the mediastinum, the middle mediastinum, accommodates the pericardium, coronary heart, lung roots, and phrenic nerves. The pericardial cavity is the third serous cavity contained within the chest, with the two pleural cavities. The pericardial cavity is conical in shape, with the base of the cone mendacity posteriorly to the proper and the apex anteriorly to the left. As with the pleura, a visceral portion of the pericardium is distinguished overlying the guts and proximal nice vessels, usually called the epicardium, as is a parietal portion. Most of the lateral and anterior portions are contiguous but not normally adherent to the pleura. Posteriorly, a blind recess of the pericardial cavity is bordered by the pericardial reflection between the pulmonary veins and inferior vena cava, known as the oblique pericardial sinus. Small recesses exist between the superior and inferior pulmonary veins on all sides and behind the fold of the left vena cava (ligament of Marshall), a small crease of pericardium working from the left facet of the pulmonary trunk to the left atrium, between the neck of the left auricle and the left pulmonary veins. The left vena cava fold incorporates the vestigial remains of the left widespread cardinal vein. In situ the center occupies an uneven place, with its apex pointing anteriorly, inferiorly, and about 60 degrees toward the left. Its 4 chambers are organized in two functionally related pairs, separated from one another by the cardiac septum (see Plate 1-5). The anatomic nomenclature of the guts removes it from the body and places it on its apex, and thus the cardiac septum is in a sagittal plane. This follow has led to misconceptions and difficulties in orientation amongst cardiologists and surgeons. On a chest radiograph, for instance, the left cardiac border is fashioned by the left ventricle, however the right border is shaped by the right atrium, not the proper ventricle, which lies anterior. The main and necessary part of the left atrium lies immediately posterior and within the midline in front of the backbone and esophagus, allowing the pulmonary veins to be as short as possible. To the left of the best ventricle, a small section of the left ventricle is seen, separated from it by the anterior interventricular sulcus (groove). The anterior interventricular (descending) department of the left coronary artery (see Plate 1-5) lies in this groove, once more embedded in fat. To the right of the pulmonary trunk lies the intrapericardial portion of the ascending aorta, the base of which is essentially covered by the right auricle (right atrial appendage). As this groove descends alongside the posterior aspect of the best atrium, it turns into less distinct. The posterior wall of the left atrium types the anterior wall of the oblique pericardial sinus. The aortic arch crosses the pulmonary artery bifurcation after giving off its three major branches: the brachiocephalic (innominate), left common carotid, and left subclavian arteries. However, its wall consists of cardiac muscle, and because of its embryonic origin, the coronary sinus should be thought of a real cardiac construction. The diaphragmatic surfaces of the best ventricle and the left ventricle are separated by the posterior interventricular sulcus (groove). Its position corresponds to that of the sulcus terminalis externally (see Plate 1-6). From the lateral side of the crista terminalis, a large quantity of pectinate muscle tissue run laterally and usually parallel to one another along the free wall of the atrium. The triangular-shaped superior portion of the best atrium-the right auricle-is also crammed with pectinate muscles. One pectinate muscle originating from the crista terminalis is normally bigger than the others and is recognized as the taenia sagittalis. The interatrial septum types a shallow despair within the septum known as the fossa ovalis. The remainder of the septum is muscular and usually types a ridge across the fossa ovalis, the limbus fossae ovalis. A probe may be passed beneath the anterosuperior part of the limbus into the left atrium in some instances, and the foramen (fossa) ovalis is then "probe patent. These bands kind a large, nearly circular orifice with no obstacle to move within the normal coronary heart.
As the trough approaches the bottom of the appendix gastritis diet juice discount nexium 20 mg free shipping, a V-shaped incision is created round roughly 60 % of its circumference; this allows the bottom of the appendix to be folded into the cecum with out kinking gastritis symptoms relief generic nexium 40 mg online. Creation of ColoniC submuCosal tunnel 8 9 A small hole is punched within the mucosa of the colon utilizing artery forceps gastritis diet 5 bites nexium 20 mg generic with amex. The tube is fixed externally to the abdominal wall and washouts can be commenced the following day. Artist Date 60 12c E Evans 21 12 12 12d Date 12e operation 557 fashioning the stoma 13a�g Two skin flaps (V and rectangular) are created at the site of the stoma. The cecum or colon is sutured to the anterior belly wall to forestall pressure on the stoma or volvulus of the bowel on the conduit. The rectangular flap is then sutured over the anterior circumference of the conduit till the anastomosis is full. This is sutured into the conduit as described above, and the rest of the anastomosis is completed by suturing the conduit to the umbilical rim. The affected person ought to be given some eight Fr and 10 Fr catheters, as a end result of if catheterization turns into difficult, the smaller catheters can be used initially to assist dilate the stoma. If severe stomal stenosis develops, dilatation under common anesthesia is recommended, following which a stopper could be left in situ for a period to scale back the risk of a further stenosis. The bag is crammed with the required phosphate and infused over a 10-minute period. Uncommon complications include leakage of fecal fluid via the stoma, and if this occurs, the valve mechanism will want to be revised or a valve created, if this had not been done in the first instance. A day by day enema is given for the primary few months, but after that about half the patients use the washouts on alternate days or, hardly ever, even much less frequently than that. Initially, many sufferers expertise colicky belly pain, and this can be helped by lowering the concentration of the phosphate and the rate of enema infusion. Most sufferers continue to use a washout, but if fecal leakage occurs between enemas, the volume could be lowered or increased and this often resolves the issue. Further washouts with faucet water often assist, but sometimes retrograde washouts are required. The in situ appendix in the Malone antegrade continence enema procedure for faecal incontinence. The classic strategy to the neonate diagnosed with Hirschsprung disease had been to perform a leveling colostomy and to wait till 6�12 months of age to perform the definitive pull-through. This method has modified dramatically over the past three a long time, and transition to major pull-through is now predominant. The transanal approach is now used by a large proportion of pediatric surgeons, and is discussed on this chapter. Perhaps the commonest indication for a full-thickness biopsy is the kid who has undergone multiple indeterminate suction rectal biopsy. Retain the needle on probably the most cephalad of those sutures, as it may be used to start the closure of the defect after the biopsy is obtained. Using sharp curved scissors, a full-thickness incision is made along the decrease half of the rectal wall, between the dentate line and the center suture. Once that is carried out, the scissors can be placed in the presacral space and gently unfold. A colostomy can be required in these patients with a delayed diagnosis of Hirschsprung disease, the place the colon has turn into overly distended and not amenable to a major pull-through. In addition, placement of a leveling colostomy allows the proximal bowel to develop, which can stretch the mesentery and simplify the following pull-through procedure. Finally, this colostomy may be closed during the pull-through, thus avoiding a 3rd operation. The infant ought to obtain rectal washouts and be placed on broad-spectrum, intravenous antibiotics just prior to the incision, but no formal bowel preparation is required or effective. If that is the case, a good place to begin is just above the peritoneal reflection. A pair of fine, sharp scissors is used to make an incision solely via the seromuscular layers. The muscular layer, which is fairly thick, even within the aganglionic section, makes this dissection pretty straightforward. Hypertrophied nerve bundles, despite the presence of ganglia, indicate that one is still within the transition zone. Importantly, the transition zone varies from the anti-mesenteric and mesenteric sides of the bowel. Thus, the surgeon must confirm this appropriate stage by sending a frozen section on the mesenteric side of the colon as nicely. Because of the comparatively large caliber of the bowel, stomal prolapse and peristomal hernias are common problems. A sew is positioned between the proximal and distal loops of bowel, starting at the fascia, then to each limb of bowel, and at last again to the fascia. A portion of the fascia could additionally be closed within the mid-portion of the defect between intestinal segments. These dilatations will forestall narrowing of the opening and allow the dilated proximal colon to return to regular size. As with different pull-through procedures, ganglionic bowel is introduced down to less than 1 cm proximal to the dentate line. To protect the autonomic nerve plexus to the genitourinary system, little or no manipulation of the rectum is carried out anteriorly. The procedure has undergone a quantity of modifications, the most important of which was by Martin and included the utilization of an automatic stapling gadget. The child is admitted the day before the surgery for a mechanical bowel preparation in addition to oral antibiotics. More just lately, primarily based on lack of proof supporting its use, our group and others have deferred from the use of a bowel prep. Care should be taken to give adequate rectal and colonic washouts, as stool is usually inspissated in the distal rectum. The baby is placed in a supine position and prepared circumferentially from the stomach to the ft. Excellent publicity is obtained by assistants supporting and flexing the decrease extremities on the hips through the anal anastomosis. By preserving the remainder of the arcades, the bowel should maintain its viability. The ureter is rigorously recognized and the peritoneal reflection between the rectum and bladder is incised. Dissection may be facilitated by a blunt clamp, however can also be very simply carried out with the index finger. Tacking sutures are placed on both left and proper sides of the bowel in order that it can be retracted anteriorly through the pull-through procedure. Care is taken to keep this distance by curving the incision as one strikes laterally in every path. Needles are positioned into the defect created by the incision and are retained for the initiation of the anastomosis. In the past, a proximal spur left between the bowel segments brought on the eventual formation of big fecalomas. The process was modified by Boley by performing a primary anastomosis on the anus, and then additional modified by Coran. As with the Duhamel approach, this procedure avoids injury to the pelvic nerves and, by remaining inside the muscular wall of the aganglionic segment, necessary sensory fibers and the integrity of the internal sphincter are preserved. Although one imagines that leaving aganglionic muscle surrounding regular bowel might result in a high incidence of constipation, that is typically not the case. The legs are carefully padded and positioned on wood skis extending off the end of the desk. A hockey-stick incision is made incorporating the leveling colostomy (if present). The similar kind of incision is made, however, for infants undergoing a main pull-through operation. The endorectal dissection is then began about 2 cm beneath the peritoneal reflection. The authors have progressively shortened the size of the endorectal dissection, because longer lengths of muscular cuff might lead to elevated bouts of constipation and enterocolitis. Once the submucosal layer is reached, the seromuscular layer is divided circumferentially using blunt dissection with hemostat or a Kitner dissector.
Some youngsters with massive tonsils and adenoids show few or no signs of sleepdisordered respiration gastritis yogurt buy nexium 20 mg online, whereas others with severe obstructive symptoms are discovered to have relatively normal-sized tonsils and adenoids atrophic gastritis symptoms uk buy nexium 20 mg mastercard. It is evident from these instances that obstruction to airflow additionally depends on the tone and volume of surrounding tissues gastritis beer buy nexium 20 mg low price. Thus, the presence of comorbid circumstances such as obesity, craniofacial anomalies, and neuromuscular issues should be considered in understanding the pathophysiology in every child. Whether the obstruction outcomes from adenotonsillar hypertrophy alone or from additive collapse of surrounding tissues, the child must increase respiratory effort to maintain airflow. Increased intraluminal adverse stress towards compliant pediatric airway buildings results in airway collapse and cessation of airflow via the Bernoulli effect. Abnormal peripheral and central neuromuscular regulation of respiratory operate also contributes to the development of sleep-disordered breathing and obstructive symptoms. Whereas daytime sleepiness is regularly reported in adults with obstructive sleep apnea, kids extra often have nonspecific behavioral difficulties corresponding to hyperactivity and studying incapacity. Parents may report a history of continual rhinorrhea, allergic rhinitis, and poor urge for food. Examination of the kid may reveal audible mouth breathing, dry lips, hyponasal speech, and the so-called adenoid face, an elongated or oblong face with the mouth open and an expression of being misplaced or apathetic. The lowest grade denotes normally sized tonsils that fit throughout the tonsillar fauces and the best indicates hypertrophic tonsils that obstruct at least 75% of the lateral oropharyngeal dimension. Flexible endoscopy and lateral radiography are helpful in diagnosing adenoid hypertrophy, though most cases are diagnosed clinically with examination of the adenoids carried out on the time of surgery. Adenoids are located midline within the nasopharynx in close proximity to the opening of the eustachian tubes. For this cause, adenoid hypertrophy is frequently associated with chronic center ear effusion, otitis media, and sinusitis. History and bodily examination alone are poor at differentiating easy loud night breathing from obstructive sleep apnea. Snoring, as estimated from history, and adenotonsillar size on examination have comparatively low optimistic and unfavorable predictive values within the analysis of youngsters with sleep-disordered breathing. Breathing parameters which might be usually monitored in pediatric patients embody airflow, respiratory effort, and oxygen saturation by way of pulse oximetry. End-tidal carbon dioxide focus, mind electrical potentials (via electroencephalography), chin muscle electrical potentials (vis electromyography), and leg actions may also be monitored. Obstructive sleep apnea is normally defined as cessation of airflow with continued respiratory effort for a minimum of two breaths or 10 seconds. Hypopnea is outlined as no much less than 50% reduction in airflow with associated respiratory effort for no much less than two breaths or more than 3% decrease in oxygen saturation. Apnea and apnea-hypopnea indices (number of events divided by variety of hours of sleep) are calculated for the whole length of sleep. Ideally, all children suspected of getting sleep apnea ought to bear polysomnography, but young age is a limiting factor. Bleeding, laryngospasm, vomiting, ache, and dehydration are among the commonest postoperative issues. As in all instances, the kid ought to be carefully monitored after pharmacologic intervention. Unless an intravenous catheter is already in place, induction of common anesthesia is normally completed with inhalation of sevoflurane and oxygen with or without nitrous oxide. Rapid airway obstruction may be anticipated, and oral airways of several sizes should always be readily available. Moderate continuous positive pressure is often wanted to counteract the results of a reduced upper airway muscle tone. Cuffed endotracheal tubes may be preferable to uncuffed tubes to reduce the chance of aspiration of blood. Air leak at or beneath a pressure of 25 cm H2O should be confirmed and cuff stress monitored. The use of nonsteroidal antiinflammatory medication remains controversial and varies broadly from center to heart. High-dose intravenous dexamethasone (up to 1 mg/kg, maximum of 25 mg) has been shown to cut back postoperative swelling as nicely as nausea and vomiting. Rarely, huge hemorrhage can happen when the carotid vessels are torn through the procedure. Adenotonsillectomy has been the remedy of choice, sometimes even in the absence of great adenotonsillar hypertrophy when there are concomitant predisposing conditions to obstructive sleep apnea. In common, elective surgical procedures must be postponed if the kid has excessive fever, croupy cough, common malaise, or evidence of decrease respiratory tract infection. General anesthesia by way of masks or laryngeal mask airway is preferable to endotracheal intubation and has been proven to be associated with a decrease incidence of intraoperative and postoperative respiratory complications. If intubation is required, the trachea ought to be instrumented only underneath a deep plane of anesthesia. There is delicate dilation of the ureter and renal pelvis and calyces are mildly blunted. The pelvis is severely dilated, ureters are tortuous, and the calyces are severely blunted. It does involve urethral catheterization for contrast injection, and a few children could require sedation and even basic anesthesia for catheter placement. Untreated reflux will increase the dangers of pyelonephritis and renal scarring with subsequent reflux nephropathy. The affected ureter is repositioned and retunneled into the bladder wall to create a model new ureterovesical junction with the proper length/diameter ratio. A mild method in conjunction with applicable preoperative anxiolysis is helpful in most cases. Cystoscopic procedures are usually short, however a comparatively deep aircraft of anesthesia have to be established to reduce risk of laryngospasm during urethral stimulation. Care should even be taken to safe the airway device, because the youngster is normally moved to the far end of the operating table for cystoscopy. Posterior Urethral Valve Posterior urethral valve is a standard cause of bladder outlet obstruction in male kids. Malformation of the posterior urethra within the type an obstructive membrane results in varying levels of urethral obstruction. Nonpalpable testes account for just one fifth of all cases of cryptorchidism; in 40% of instances the testis has an intraabdominal location, in one other 40% a high inguinal location, and within the the rest reveals atrophy or congenital absence. Most palpable undescended testes will spontaneously descend throughout infancy, but this hardly ever continues after 9 months of age. Occasionally, the primary presenting drawback is renal failure with related uremic symptoms. Approximately one third of patients with posterior urethral valve progress to end-stage renal disease, requiring lifelong renal substitute therapy or renal transplantation. Bladder outlet obstruction is usually addressed instantly at birth by placement of a urethral catheter. If the urethra is too small to accommodate the required surgical devices, direct vesicocutaneous or ureterocutaneous urinary diversion procedures may be required. Orchiopexy could be performed through an inguinal, suprainguinal, or laparoscopic method. In instances in which the testis is in a high intraabdominal position and spermatic vessels are short, a two-stage process could also be required to permit time for collateral vessel formation after initial vessel clipping, followed by mobilization and scrotal fixation of the testis. An intense vagal response could be seen with surgical traction and manipulation of the spermatic wire and testicle; this will additionally occur with pneumoperitoneum as in all laparoscopic procedures. A high incidence of postoperative nausea and vomiting is observed, and thus prophylactic antiemetic treatment ought to be routinely given. Hypospadias Hypospadias is congenital malpositioning of the urethral meatus on the ventral side (underside) of the penis. The irregular opening can occur anyplace from the glans penis to the penile shaft and even right down to the scrotum and perineum. Hypospadias involving the glans penis, also identified as coronal hypospadias, is the commonest (50% of cases). Chordee, an irregular ventral curvature of the penis, is commonly seen with hypospadias.






