Diflucan
Diflucan
Diflucan dosages: 400 mg, 200 mg, 150 mg, 100 mg, 50 mg
Diflucan packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

From a developmental perspective antifungal roof shingles cheap diflucan 100 mg without prescription, renal operate is very depending on gestational age and postnatal adaptations definition of fungus cheap diflucan 50 mg fast delivery. Developmental adjustments that occur in renal operate are higher characterized than another organ system (Table 79 antifungal powder for jock itch order diflucan 100 mg fast delivery. Failure to account for the ontogeny of renal operate and regulate dosing regimens accordingly may end up in a degree of systemic publicity that may improve the chance of drug-associated antagonistic events. Failure to modify the dose and dosing interval for digoxin to compensate for developmentally associated differences in its plasma clearance can produce important toxicity, particularly given the low therapeutic index for this drug (25). Finally, it is essential to acknowledge that perceived developmental variations in each pharmacokinetics and pharmacodynamics can be influenced by the concomitant expression of illness whereby observations made in the course of the "properly" state could be very totally different from these during each acute. As recently reviewed by Mulla (28), development can influence pharmacodynamics by way of consequences of maturational changes in drug receptor number, receptor affinity, receptor density, signal transduction, or alterations within the intracellular milieu essential for the creation of a pharmacologic effect. Similarly, ontogenic profiles seem to be operative for valproic acid-associated hepatotoxicity (31), midazolam-associated sedation (32), and warfarin sensitivity (33,34), all of that are examples the place age-associated variations in drug response appear independent of pharmacokinetic alterations. As also reviewed by Mulla (28), much of the data concerning developmental pharmacodynamics are derived from animal studies. In healthy adults, the interpretation of genotype-phenotype relationships is largely two dimensional provided that the genotype is "mounted" (with the exception of epigenetic events) and absent exterior modifiers. Food and Drug Administration has included pharmacogenetic data (predominantly derived from grownup studies) within the permitted product labels for approximately 10% of medication offered within the United States (38), the medical utility of these knowledge in pediatric therapeutic determination making can be fairly restricted. Specifically, understanding the developmental trajectory for the practical exercise of genes as nicely as the developmental context during which the gene(s) of curiosity is/ are working is of paramount significance when considering the predictive nature of genotype associated to either drug disposition or action, both therapeutic and opposed (39). The potential scientific utility involved with the utilization of genotype-derived activity scores for a specific drug metabolism is when the score could be demonstrated to be a reliable predictive biomarker of drug clearance. As denoted beforehand, maturation of metabolic capability for a given drug-metabolizing enzyme or transporter has a particular developmental trajectory with practical maturity. However, as just lately denoted by Holford (41), predictive accuracy of allometric scaling is compromised during periods of growth the place the actions of pathways answerable for drug clearance. The extension of this precept to the sector of developmental pharmacogenomics is exemplified by intervals of life where the maturation of drug clearance pathways/mechanisms demonstrates genotype-phenotype discordance. Instead, we offer an outline of the overall classifications and mechanisms of motion of essentially the most generally used cardiovascular medication within the pediatric population. More disease-specific drug information and additional particulars can be found in accompanying chapters dealing with cardiac transplantation, arrhythmias, coronary heart failure, myocarditis, hypertension, and hyperlipidemias. This change in sodium focus affects sodium-calcium a thousand � o 331 (neonates/preterms) 333(1-11 months) " 334(1-11 yrs). However, the rise in contractility is modest and may be imperceptible within the nonfailing heart. Digoxin is readily absorbed from the gastrointestinal tract, and peak serum ranges occur approximately 30 to 90 minutes after an oral dose. The loading dose (digitalization dose) is generally divided over 12 to 24 hours (half whole loading dose initially, one-fourth 6 to 12 hours later, and one-fourth 12 to 24 hours after the preliminary dose). Administration of a loading dose is related to a higher incidence of toxic results, especially in newborns. The half-life is approximately 20 hours in infants and 40 hours in older youngsters, adjustments related to developmental increases in renal operate. Consequent to its lengthy elimination half-life, digoxin could also be given once day by day in infants and youngsters. Because of the lack of relationship between larger serum levels and a greater therapeutic impact, the goal serum digoxin levels ought to range between 1 and 2 ng/mL. The main indication for acquiring a serum digoxin concentration is in cases of known or suspected digoxin toxicity. This occurs mostly in circumstances of accidental overdose and in complicated patients with renal failure and/or those taking medicines which will interfere with digoxin clearance. However, some sufferers might profit from the reduction in heart rate mediated by digoxin. Digoxin exerts important neurohormonal modulating results in adult sufferers with congestive coronary heart failure which can be of benefit, even in the absence of measurable objective modifications in cardiac function. Drugs that will predispose to digoxin toxicity include diuretics (hypokalemia) 1673 and amiodarone (reduced elimination of digoxin). Cardiac toxicity in infants usually leads to second- or third-degree atrioventricular block with resulting bradycardia, however nearly any kind of arrhythmia can be produced by digoxin toxicity. In cases of life-threatening arrhythmias, specific Fab antibody fragments should be administered intravenously. Stimulation of /31-adrenergic receptors within the mature heart increases price, contractility, relaxation, and conduction. Stimulation of /32-adrenergic receptors in the lungs produces bronchodilation and modest pulmonary vasodilation. In contrast to a lot of the vascular mattress, skeletal muscle vasculature contains /32-adrenergic receptors that promote vasodilation when activated. Dopaminergic receptors within the splanchnic and renal vascular beds produce vasodilation in response to dopaminergic agonists, Maturational adjustments in the receptor-effector and signal transduction pathways lead to age-related variability in responsiveness to adrenergic agonists (49-51). Loading circumstances, volume status, and responsiveness of the peripheral vasculature also can affect the responses to these brokers, especially in critically ill infants and kids. Adrenergic agonists bear speedy biotransformation and consequent to their very quick elimination half-life, are administered by steady intravenous infusion. Comparison of the relative results on /3-, a-, and dopaminergic receptor subtypes for varied drugs is offered in Table 79. However, it appears to be much less arrhythmogenic than the opposite sympathomimetic arrunes. Dopamine Dopamine is an endogenous precursor of norepinephrine with direct cardiac,8]-adrenergic agonist results. In addition dopamine indirectly stimulates,8]-receptors by promoting the release of norepinephrine from presynaptic sympathetic nerve terminals inside the myocardium. Dopamine has little or no effect on,82-adrenergic receptors, but at greater concentrations, It stimulates ai-adrenergic receptors. At greater rates of infusion, ai-receptor stimulation (vasoconstriction) becomes more pronounced and the renal vasodilating effect is overcome. Dopamine has gained considerable popularity for use within the acutely sick toddler or baby with cardiac dysfunction from any etiology (52-54). Low to reasonable doses are thought to incur an extra advantage by rising renal blood move and sustaining urine output, though this has not been conclusively confirmed. At conventional doses, dopamine has little effect on pulmonary vascular resistance. High rates of infusion could increase systemic vascular resistance, induce sinus tachycardia, and provoke arrhythmias and, in critically unwell patients with circulatory insufficiency, can outcome in peripheral gangrene. Epinephrine Epinephrine is produced by the adrenal medulla and has extremely potent effects on a- and,8-adrenergic receptors. At low concentrations, the predominant effects embody increased coronary heart fee, contractility, and systolic blood pressure because of,8]-adrenergic stimulation. As the dose increases, diastolic blood stress might decline barely as a result of,8radrenergic results m the penpheral vasculature. At larger doses, a-adrenergic effects turn out to be distinguished and pronounced vasoconstriction occurs. The initial infusion price should be at the decrease finish of the beneficial dosage and then progressively increased as wanted. Epinephrine increases myocardial oxygen requirements due to its distinguished inotropic and chronotropic results. Tissue ischemia can occur due to peripheral vasoconstriction, especially with excessive rates of infusion. This pharmacologic profile ends in dilation of the renal and splanchnic beds, elevated renal blood flow and glomerular filtration rate, and diuresis. Fenoldopam is used primarily for treating hypertension in adults, however some facilities have used intravenous fenoldopam in infants and youngsters in an effort to promote diuresis (55,56). Potential benefits of fenoldopam include fast titration and few unwanted side effects past excessive hypotension. Additional prospective research are wanted to decide the position of fenoldopam within the administration of acutely ill infants and kids with coronary heart disease. Infusion of norepinephrine will increase systolic and diastolic blood stress, systemic vascular resistance, and contractility.
Huluci Behcets a Turkish dermatologist fungus on neck effective diflucan 400 mg, first described the illness in three sufferers (224) fungus on tree trunk 400 mg diflucan buy with amex. Initially it was thought to be more prevalent close to the old silk buying and selling routes in the Middle East and in Central Asia and was known as the Silk Road Disease antifungal antibacterial soap diflucan 50 mg best. It is more widespread in Japan, Turkey, and Middle East in comparability with rest of the world (227). There is excessive frequency of familial instances particularly in pediatric patients (228,229). It includes several organs such as central nervous system, gastrointestinal, pores and skin, mucous membranes, eyes, and musculoskeletal system. Anecdotal reviews have described other cardiac issues similar to endomyocardial fibrosis, noninfective endocarditis, aneurysms of the ascending aorta, intracardiac thrombus formation, coronary artery aneurysm, and pulmonary artery aneurysms (243-246). All of these sufferers responded to immunosuppressive remedy and recovered without residua. Recurrence of the aneurysmal illness, hypercoagulable state, thrombosis, and the tendency for an exaggerated inflammatory response (pathergy) have been major drawbacks reported with the procedure. Severe conduction abnormalities are uncommon, for instance, complete heart block resulting in congestive cardiac failure (250). In some instances, this vasculitis seems to cause myocardial harm as a end result of the mixture of small vessel vasculitis of myocardial vessels, coronary artery involvement, and/or cytokine-induced myocarditis (250). Myocardial involvement is extra commonly reported in adult dermatomyositis and in polymyositis (253-259). In adults, cardiac problems are the cause of demise in 10%-20% of patients with grownup dermatomyositis and polymyositis (250,260). A vital correlation was discovered between diploma of myonecrosis as measured by muscle enzymes and the degrees of antisignal recognition particle myositis-specific autoantibodies (261,262). It could be argued that if hypertension has a job in these cardiac findings, it might be in part because of corticosteroid therapy (265). Systemic scleroderma with inner organ involvement is a uncommon disease in childhood and happens less generally than local scleroderma illnesses such as linear scleroderma and morphea (268,269). The prognosis and mortality in juvenile onset systemic illness is, in general, better than grownup onset disease (270). Yet, in those youngsters with extreme or deadly scleroderma, disease progression and mortality may be harder to stop (268,271-273). The cardiac involvement in systemic scleroderma may be primarily as a outcome of the scleroderma disease process or secondary to severe lung involvement. Pulmonary involvement is the most typical systemic organ affected by scleroderma (75% patients) and cardiac involvement alone is rare (1 %) but a blended image of cardiopulmonary involvement is the commonest explanation for demise in systemic scleroderma (272,274,275). Most consider that patients who also had polymyositis with skeletal muscle involvement along with their scleroderma are more at risk for cardiac involvement and congestive cardiac failure (278-280). Some major autoimmune myocardial inflammation can also be thought of as a small factor contributing to myocardial harm and fibrosis. Myocardial fibrosis is reported to be the most typical autopsy discovering in deadly cases of juvenile systemic sclerosis (279) and myocardial fibrosis is taken into account as an indicator of cardiac involvement in systemic scleroderma. The myocardial fibrosis in scleroderma is histologically different from that as a end result of atherosclerotic coronary artery illness. Cardiac ischemic disease may outcome as a result of a quantity of causes corresponding to restrictive pulmonary illness, coronary artery involvement, myocardial microvasculitis inflicting perfusion defects, impaired restore mechanism, and sclerosis. Raynaud phenomenon is very common in patients with scleroderma, and Raynaud equivalent vascular phenomenon in cardiac vessels and coronary arteries of these sufferers leads to repeated cardiac ischemia and myocardial fibrosis (288,289). Systemic vascular disease leading to systemic hypertension and renal crisis can also have an effect on cardiac perfusion adversely and lead to left ventricular failure (280). Scleroderma can also present initially as pericardial illness or conduction abnormalities secondary to myocardial involvement. The most common symptom because of myocardial involvement in juvenile scleroderma is dyspnea and lowered train tolerance. The prevalence of the anti-Sci 70 antibody is rare in juvenile onset disease, with or with out extracutaneous manifestations (276). Endomyocardial biopsy is neither a risk-free process neither is it used very often in follow. The available info on cardiac involvement largely comes from autopsy results that only characterize the intense finish of the spectrum of the disease. Early and aggressive remedy with immunosuppressant medication, fibrinolytic medication, and supportive therapy might help to prevent cardiac disease and improve the result in sufferers with juvenile onset systemic scleroderma. It can also be important to monitor youngsters with local scleroderma for systemic disease. When it does occur, cardiac involvement in sarcoidosis remains to be typically ignored due to the lack of knowledge of its risk, its sluggish subclinical development, and the absence of any sturdy and dependable diagnostic software (297). In Japanese patients, 85% of deaths with sarcoidosis are because of cardiac involvement (298-300). They reported that medical options and shows of their cohort have been similar to that of adults but they found cardiac involvement to be more frequent in youthful sufferers and adolescents than in adults (302-306). One in 4 of the main criteria and two or extra of the 5 minor standards are happy. Abnormal echocardiography: regional abnormal wall motion or morphologic abnormality (ventricular aneurysm, wall thickening). Nuclear drugs: perfusion defect detected by 201thallium or ninety nine m technetium myocardial scintigraphy. Sarcoidosis can affect the pericardium, myocardium, or endocardium with equal frequency (296,313). These post-mortem findings support recent scientific findings that the true incidence of clinical cardiac involvement in sarcoidosis could additionally be between 5% and 50% (314). Sometimes cardiac involvement solely got consideration of physicians after the pulmonary illness resolved (315). Occasionally cardiac involvement could be the first presentation of the illness (306). Echocardiography is beneficial to diagnose the cardiac involvement in patients with sarcoidosis. Echocardiography could also be useful if it demonstrates a basic basal interventricular septal thinning or localized ventricular aneurysmal dilation, often with out coronary artery illness. Myocardial biopsies have a poor diagnostic yield �20% to 30%) because the sarcoidosis disease involvement is patchy and most biopsies are carried out on the best aspect of coronary heart (311,312,320). Less frequently, pericardial effusion, cardiac tamponade, and cardiac failure could also be seen (195,317,323). These problems typically happen in patients with widespread myocardial involvement (311,324). Other disease-modifying drugs and immunosuppressants such as methotrexate, azathioprine, hydroxychloroq uine, chloroquine, cyclophosphamide, cyclosporine A, thalidomide, pentoxyphylline, and infliximab have been used with varying success (306,308,312,325-327). A combination of steroids and another immunosuppressant may be used to limit steroid side effects. In sufferers with disseminated myocardial involvement, the utilization of antiarrhythmic medicine and automatic implantable cardiac defibrillator as bridge therapy while ready for cardiac transplant has been advocated to stop sudden death (312). Estimates of the prevalence of arthritis and different rheumatic circumstances within the United States: Part I. Determination of anti-citrullinated peptide antibodies in the sera of patients with juvenile idiopathic arthritis. Cardiac tamponade in juvenile chronic arthritis: report of two circumstances and evaluation of publications. Large pericardial effusion requiring pericardiocentesis as cardinal sign of macrophage activation syndrome in systemic onset-juvenile idiopathic arthritis. Prevalence of pericardia I effusion by echocardiography in juvenile rheumatoid arthritis. A patient recognized with pauciarticular juvenile rheumatoid arthritis after a mechanical prosthetic valve alternative because of aortic regurgitation. Cardiac operations for North American youngsters with rheumatic diseases: 1985-2005. The incidence of pediatric rheumatic illnesses: outcomes from the Canadian Pediatric Rheumatology Association Disease Registry. Description of 37 instances in children and a dialogue of endocrine remedy in 32 of the cases.
This process is presumed to occur by an autoimmune-like mechanism triggered by the initial viral insult fungus gnats human skin 400 mg diflucan order fast delivery. Several murine models have been studied that suggest that cytokine-mediated modulation of the immune response to viral infection might result in fungus ergot 100 mg diflucan discount overnight delivery induction of chronic autoimmune myocarditis (118-124) fungus covered scale tunic buy diflucan 100 mg cheap. Cytokines contribute to regulation of antibody manufacturing and maintenance of self-tolerance. In other strains, nonetheless, a second autoimmune section of myocarditis appears later, with findings of diffuse mononuclear cell infiltrates inside the heart. Both of those cytokines are identified to participate in leukocyte activation, which may be helpful in selling a specific lymphocyte response to viral infection. The function of cytokine exercise relative to the pathogenesis of viral myocarditis or subsequent development of chronic autoimmune myocarditis is beneath investigation. Furthermore, in patients with enterovirus an infection, this was more pronounced than in patients in whom no enterovirus was detected. Novel auto antigens also have been recognized in patients with myocarditis (115-117). In the rat mannequin, nitric oxide expression is crucial to the pathology of autoimmune myocarditis (124). It is troublesome to extrapolate the knowledge obtained in animal models of myocarditis to human disease. Apoptosis Apoptosis, or programmed cell demise, has an important role in embryogenesis, tissue homeostasis, and regulation of immunologic responses, among normal physiologic processes, and is related to the expansion and regression of tumors (108). Cells undergoing apoptosis exhibit attribute morphologic and biochemical options, together with chromatin aggregation, nuclear and cytoplasmic aggregation, and formation of apoptotic our bodies resulting from the partition of the cytoplasm and nucleus into membrane-bound vesicles. These apoptotic bodies are rapidly phagocytosed by adjacent macrophages or epithelial cells, with out resulting in an inflammatory response. Within such areas,::::1 of cells may stain posi% tive, together with myocytes, infiltrating inflammatory cells, and endothelial cells. In the tissue sections from control sufferers, either unstained cells or sporadically stained cells (one or two per section) could also be detected. Furthermore, a quantity of inflammatory cells could also be seen to be undergoing apoptosis. In tumors, infiltrating immune cells are destroyed by the induction of apoptosis by way of the expression of Fas ligand on the tumor cell that binds Fas on the lymphocyte. The 55-kDa protein of ElB binds to , and inhibits, p53, but the mechanism of suppression by the 19-kDa protein is unknown. It has been recognized for a quantity of years, nonetheless, that totally different variants induce completely different pathologic mechanisms and that completely different strains of mice are affected in a special way. It is more and more acknowledged that myocardial dysfunction and evidence of coronary heart failure can present at some point during their lifetimes (70,125-127). It remains unclear what the underlying cause of these long-term sequelae might be, however viral persistence and autoimmunity have been Widely speculated. Enteroviral protease 2A directly cleaves the cytoskeletal protein dystrophin, leading to dysfunction of this protein. Therefore, it appears that a fancy interaction between the viral genome and the heart occurs and ends in the short- and long-term consequence of affected sufferers. Enteroviral protease 2A cleaves dystrophin: proof of cytoskeletal disruption in an acquired cardiomyopathy. Newer approaches to genetic research, together with genome-wide affiliation research, may result in an enhanced understanding of genetic predispositions for buying viral myocarditis. Many physicians and scientists maintain onto the concept that myocarditis is a primary inflammatory dysfunction, however definitive information are limited to assist that speculation. Continual reassessment of sufferers with myocarditis is really helpful as their clinical image can change dramatically in a very short period of time. Many sufferers current with comparatively mild disease, with minimal or no respiratory compromise and solely gentle indicators and/or symptoms of congestive coronary heart failure. These patients require close hemodynamic and electrocardiographic monitoring to assess whether the disease will progress to worsening heart failure and the necessity for extra intensive medical care. Murine models of myocarditis suggest that exercise might end in elevated viral replication as nicely as myocardial irritation and necrosis (143). Thus, it seems prudent to place patients underneath this restriction at the time of prognosis. Normal arterial blood oxygen ranges must be maintained for any affected person with compromised hemodynamics leading to hypoxemia. Although no particular therapy aimed toward reversing myocardial damage is presently extensively really helpful, maintenance of cardiac output at ranges that provide adequate tissue perfusion and forestall metabolic disturbances and end-organ dysfunction is crucial to good outcome. N Engl] Med 2001;344:1498-1503, with permission from the Massachusetts Medical Society. This seems, at least partly, to do with the particular viruses identified in the myocardium. Medical Management the appropriate medical administration of sufferers with myocarditis relies on their medical presentation. Patients presenting with delicate symptoms of congestive coronary heart failure and preserved cardiac output should be frequently evaluated as they could progress to a more decompensated state. Diuretics could additionally be used judiciously to treat signs of shortness of breath or peripheral edema. There are growing information that help the utilization of nonselective beta blockade in patients with myocarditis. Human studies clearly report the shortage of beta blocker use as an unbiased predictor of poor prognosis (148). Additional potential therapeutic methods for heart failure may be discovered elsewhere (144). Patients with proof of decompensated heart failure may be greatest managed in an intensive care setting. Significant quantity overload must be treated with diuretic therapy accompanied by avoidance of great electrolyte disturbances as this will likely provoke arrhythmias. Patients who show signs of poor perfusion and low cardiac output should all be managed in an intensive care setting with careful choice of inotropic agents. A more intensive administration method to patients with decompensated coronary heart failure could also be found elsewhere in this textual content as nicely in current evidencebased guideline statements (144,149). Ventricular arrhythmias in the setting of systolic dysfunction could require intravenous amiodarone. Despite aggressive therapy of those arrhythmias, fast deterioration to ventricular fibrillation, particularly in the very young, could occur and must be handled instantly by direct-current cardioversion. Acute or persistent conduction system disease, including full heart block, may be seen and must be treated with temporary or permanent pacing primarily based on the medical scenario. Chronic arrhythmias could persist lengthy after the acute illness has handed, particularly within the setting of myocardial fibrosis. Thus, children who get well from myocarditis, regardless of cause, must be adopted indefinitely with appropriate arrhythmia surveillance. Our apply has been to perform ambulatory Holter monitoring annually at a minimum with extra frequent assessment or different methods corresponding to occasion recorders in patients with signs or concerns for ongoing arrhythmia. The use of immunosuppressive and immunomodulatory brokers in suspected cases or confirmed cases of viral myocarditis remains controversial. The Myocarditis Treatment Trial analyzed the use of immunosuppressive and steroid remedy (52). Although the examine was carried out in grownup patients, the results are potentially relevant to kids. There was no difference amongst sufferers handled with azathioprine and prednisone, cyclosporine and prednisone, and traditional remedy. Immunosuppressive therapy was not beneficial in most sufferers with histologically confirmed myocarditis. However, there could also be chosen populations with chronic myocarditis that profit from immunosuppression. The prognosis of acute myocarditis in newborns has been poor over time (157-159). The six infants who survived had no apparent sequelae, although long-term follow-up was not reported. It is most likely going that other viral causes of myocarditis similar to adenovirus have similar poor outcomes as infants. Older infants and youngsters have a greater prognosis, with a mortality price between 10% and 25% in clinically recognizable instances.
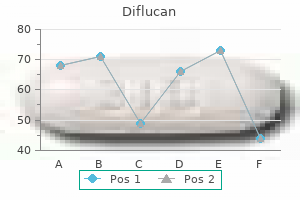
The quantity in every group (brackets) and the predicted survival out of a possible 5 years are proven fungus joint pain diflucan 150 mg buy without a prescription. The variety of patients handled with calcium channel blockers is steadily decreasing fungus gnats dunks generic diflucan 200 mg. Recently fungus dry rot generic 200 mg diflucan fast delivery, the use of particular closed hub systems has been described in kids to lower the danger of catheter-related infection (275). Some youngsters with an distinctive response to intravenous epoprostenol might wean from intravenous to oral therapy (47,276). Survival charges at 1, three, 5, and 10 years had been 94%,88%, 81%, and 61 %, respectively; treatment success rates at 1, 3, 5, and 10 years were 83%, 66%, 57%, and 37%, respectively. However, a recent examine of subcutaneous treprostinil in young children confirmed promise with tolerable unwanted aspect effects (280). Treprostinil has also been studied in an inhaled type (281) and studies are being carried out in kids. Iloprost requires patient cooperation with the therapy administration lasting 10 to 15 minutes, which is tough for younger children (256,282,283). Inhaled iloprost has additionally been studied together with bosentan and sildenafil, amongst others (285-287). While helpful results have been noted in short-term trials, these could also be attenuated with prolonged remedy (288,289). Elevated hepatic aminotransferase ranges occur in roughly 11% of adults and 3% of kids handled with bosentan. A retrospective research of 86 children on bosentan for a median publicity of 14 months with and without concomitant remedy found that bosentan supplied a sustained medical and hemodynamic improvement and was general properly tolerated, with 2-year survival estimates of ninety one % (8). Followup of those patients at four years revealed that the Kaplan-Meier estimate of illness development in sufferers while on bosentan was 54% with a survival estimate of 82%. There was a progressive decline within the helpful effect of bosentan after 1 12 months, with a more pronounced decline in the children, who tended to have extra extreme illness at baseline (167). In a Japanese cohort, bosentan pharmacokinetics was not altered by sildenafil (300). Bosentan has been studied in Eisenmenger syndrome in a placebo-controlled trial in patients (see Eisenmenger syndrome). Bosentan was well tolerated and improved exercise capacity and hemodynamics with out compromising peripheral oxygen saturation (164). However, sitaxsentan was removed from the market because of considerations of adverse results on the liver. The remaining 23 kids were handled with ambrisentan as an add-on remedy due to disease development. The estimated imply � commonplace error proportion change in p V02 for the low, medium and high doses mixed versus placebo was 7. Upper respiratory tract infections, pyrexia, and vomiting occurred extra usually with sildenafil than placebo (322). A long-term extension research included children continued on sildenafil monotherapy. At three years, a rise in mortality was famous in the highdose group and the data security monitoring board requested to decrease the dose of any child receiving excessive dose. Deaths in the extension research have been associated to etiology and baseline disease severity. In 14 of 29 children transitioned from sildenafil to tadalafil, repeat cardiac catheterization showed statistically significant improvements in mean pulmonary arterial strain (53. Although 5 patients (13%) discontinued ambrisentan as a end result of severe headache, lack of clinical efficacy, or close to syncope, no patients had aminotransferase abnormalities and there were no deaths after initiation of ambrisentan during follow-up (305). A research of sildenafil in Japanese youngsters has additionally instructed security and efficacy (321). A randomized, double-blind, placebo-controlled, dose-ranging examine of oral sildenafil citrate in treatment-naive youngsters with pulmonary arterial hypertension. Doppler echo cardiographic index for assessment of worldwide right ventricular perform. Use of myocardial efficiency index in pediatric patients with idiopathic pulmonary arterial hypertension. Continuous-wave doppler echocardiographic detection of pulmonary regurgitation and its software to noninvasive estimation of pulmonary artery stress. Extraction of pulmonary vascular compliance, pulmonary vascular resistance, and right ventricular work from single-pressure and doppler circulate measurements in youngsters with pulmonary hypertension: a model new method for evaluating reactivity: in vitro and scientific studies. Noninvasive doppler tissue measurement of pulmonary artery compliance in kids with pulmonary hypertension. Standard reference for the six-minute-walk take a look at in wholesome kids aged 7 to sixteen years. Peri operative problems in children with pulmonary hypertension present process noncardiac surgery or cardiac catheterization. Bone morphogenetic protein receptor 2 mutations in adults and children with idiopathic pulmonary arterial hypertension: Association with thyroid illness. Prognostic value of b-rype natriuretic peptide in children with pulmonary hypertension. Biological serum markers in the administration of pediatric pulmonary arterial hypertension. Balloon occlusion pulmonary wedge angiography and lung biopsy assessment within the youngster with a congenital cardiac defect. Surfactant protein c mutations are the idea of a good portion of adult familial pulmonary fibrosis in a dutch cohort. Magnification pulomonary wedge angiography in the evaluation of kids with congenital heart illness and pulmonary hypertension. Pulmonary vascular input impedance is a mixed measure of pulmonary vascular resistance and stiffness and predicts scientific outcomes better than pulmonary vascular resistance alone in pediatric sufferers with pulmonary hypertension. Quantification of proper ventricular afterload in patients with and without pulmonary hypertension. The prognostic worth of pulmonary vascular capacitance determined by doppler echo cardiography in sufferers with pulmonary arterial hypertension. Noninvasive strategies for figuring out pulmonary vascular operate in kids with pulmonary arterial hypertension: Application of a mechanical oscillator mannequin. Quantitative three dimensional echocardiography in sufferers with pulmonary hypertension and compressed left ventricles: comparison with cross sectional echocardiography and magnetic resonance imaging. Role of cardiac magnetic resonance imaging within the administration of sufferers with pulmonary arterial hypertension. Cardiovascular magnetic resonance imaging as utilized to sufferers with pulmonary arterial hypertension. Weaning and discontinuation of epoprostenol in kids with idiopathic pulmonary arterial hypertension receiving concomitant bosentan, Am] CardioI2004;93:943-946. Serotonin transporter polyrnorphisms in familial and idiopathic pulmonary arterial hypertension. Prevalence and outcome in systemic sclerosis associated pulmonary arterial hypertension: utility of a registry approach. Epoprostenol for therapy of pulmonary hypertension in sufferers with systemic lupus erythematosus. Connective tissue disease presenting with indicators and signs of pulmonary hypertension in kids. Pulmonary arterial hypertension in adults born with a heart septal defect: the Euro heart survey on grownup congenital coronary heart disease. Assessment of operability of congenital cardiac shunts with increased pulmonary vascular resistance. Clinical applications of inhaled nitric oxide in youngsters with pulmonary hypertension. Measurement, interpretation and use of haemodynamic parameters in pulmonary hypertension associated with congenital cardiac disease. Late outcomes after correction of ventricular septal defect with extreme pulmonary hypertension. Validity of the LaFarge equation for estimation of oxygen consumption in ventilated children with congenital heart disease younger than 3 years-a revisit. The pulmonary vascular response to oxygen and its affect on operative leads to kids with ventricular septal defect. Genetic anticipation and irregular gender ratio at delivery in familial main pulmonary hypertension. The presence of genetic anticipation means that the molecular basis of familial primary pulmonary hypertension could also be trinucleotide repeat growth.
Caso P fungi definition yahoo answers cheap 150 mg diflucan otc, Acione L fungus dandruff diflucan 200 mg purchase line, Lange A antifungal uti discount diflucan 200 mg with amex, et al, Diagnostic worth of transesophageal echocardiography within the assessment of congenitally corrected transposition of the nice arteries in adult patients. Magnetic resonance evaluation of an grownup patient with congenitally corrected transposition of the nice arteries. Salehian 0, Schwerzmann M, Merchant N, et aL Assessment of systemic right ventricular perform in sufferers with transposition of the good arteries utilizing the myocardial performance index: comparison with cardiac magnetic resonance imaging. Cardiac resynchronization remedy for grownup congenital coronary heart illness patients with a systemic proper ventricle: analysis of feasibility and evaluate of early expertise. Left ventricular dysfunction after cardiac resynchronization remedy in congenital coronary heart disease patients with a failing systemic right ventricle. Cardiac resynchronization remedy (and multisite pacing) in pediatrics and congenital coronary heart disease: five years expertise in a single establishment. Ikeda U, Furuse M, Suzuki 0, et aL Long-term survival in aged patients with corrected transposition of the good arteries. Death and other events after cardiac repair in discordant atrioventricular connection. Postsurgical course of sufferers with congenitally corrected transposition of the nice arteries. Right ventricular dysfunction in congenitally corrected transposition of the great arteries. Myocardial perfusion defects and related systemic ventricular dysfunction in congenitally corrected transposition of the good arteries. Relation of systemic ventricular operate quantified by myocardial efficiency index (Tei)to cardiopulmonary train capacity in adults after Mustard procedure for transposition of the good arteries. Congenitally corrected transposition of the great arteries within the adult: functional status and problems. Intermediate-term end result after intracardiac repair of related cardiac defects in sufferers with atrioventricular and ventriculoarterial discordance. Maintaining tricuspid valve competence in double discordance: a problem for the paediatric heart specialist. Late outcomes of systemic atrioventricular valve alternative in corrected transposition. Congenitally corrected transposition of the good arteries: ventricular perform at the time of systemic atrioventricular valve alternative predicts long-term ventricular operate. Intention-to-treat evaluation of pulmonary artery banding in conditions with a morphological right ventricle ninety four. Early prophylactic pulmonary artery banding in isolated congenitally corrected transposition of the great arteries. Intermediate results of the anatomic restore for congenitally corrected transposition. Midterm outcomes after restoration of the morphologically left ventricle to the systemic circulation in patients with congenitally corrected transposition of the nice arteries. The hemi-rnustard/bidirectional glenn atrial change process in the double-switch operation for congenitally corrected transposition of the great arteries: rationale and midterm outcomes. As with much of congenital heart disease, the physiology and treatment of those defects derive from the embryology and morphology. In the conventional heart, the pulmonary valve sits up on the conus, a round tube of muscle, and is positioned anteriorly and superiorly (17). In contrast, the aortic, mitral, and tricuspid valves are all attached to the central fibrous physique of the center. The conal muscle beneath the aortic valve largely resorbs, leaving the aorta positioned inferiorly and posteriorly. There is a virtually normal length of conus beneath the pulmonary valve and minimal conus beneath the aortic valve. This form is morphologically and physiologically much like transposition of the nice arteries. In the center is a sort that has equal bilateral conus, such that the nice arteries are aspect by aspect, with neither vessel tucked in posteriorly. These variations are extra ambiguous both anatomically and physiologically and ought to be approached with an individualized administration plan. The extra conal muscle present beneath a semilunar valve, the more that valve is pushed superiorly and anteriorly. Aorta is pushed anteriorly and superiorly, resulting in rightward positioning of the aorta relative to the pulmonary artery. Coronary artery anomalies are of particular significance, as a result of they could alter concerns for surgical repair due to their effect on feasibility of conduit placement or coronary transfer. However, coronary artery anomalies are of explicit importance, as a result of they might alter considerations for surgical restore because of their impact on feasibility of conduit placement or coronary transfer (23). Likewise, related aortic arch coarctation, hypoplasia, or interruption-also present in about 10% of patientssignificantly increases the complexity of surgical restore when current (24,25). The chest radiograph demonstrates regular to mildly diminished pulmonary vascular markings. In a minority of patients, for instance those for whom the technical feasibility of a two-ventricle repair is debatable, cardiac catheterization is used to outline pulmonary vascular resistance to determine suitability for a Fontan operation. Hemodynamic assessment through cardiac catheterization may be essential for an additional small subset of patients in whom the results of streaming are variable and fewer apparent (10). Surgery is indicated to relieve the obstruction to pulmonary blood circulate and to septate the circulations. In most sufferers, however, surgery is performed electively between 2 and 4 months of age before the infant turns into excessively cyanotic or develops hypercyanotic spells. The chest radiograph demonstrates a normal-sized cardiac silhouette and mildly increased pulmonary vascular markings. Echocardiography often supplies complete anatomic definition with this kind as well. In particular, subcostal views can show the exact relationship of the great vessels and the size and extent of the subaortic conus. There must be a high index of suspicion for arch hypoplasia or interruption in neonates with severe subaortic narrowing. Surgery is indicated to enhance systemic oxygenation and is carried out within the neonatal period. Infants typically present with indicators of congestive coronary heart failure as the pulmonary vascular resistance falls between four and 8 weeks of age. In these, the distribution of conal tissue is closer to 50:50 beneath every semilunar valve. Relatively massive subaortic conus (small arrow) separates the aorta and pulmonary artery. In these variants, as a end result of the anatomy is extra ambiguous, the diagnostic evaluation must be as complete as possible, and serial assessments over time using complementary imaging modalities may be needed to plan the optimal method and timing of surgical repair. Additionally, patients with this variant, who prior to now both have been marginally palliated in infancy or had been deemed inoperable, at the second are resurfacing as adolescents and young adults for consideration for technically difficult operations. Young adult sufferers presenting for evaluation with out detailed details about their prior care warrant particular attention. Because serial information or multiple prior echocardiograms for comparison of the anatomy are often not available, acquiring multiple complementary imaging studies is crucial. Although intraoperative inspection of the anatomy is at all times essential, acquiring complete anatomic detail preoperatively minimizes the extra time on cardiopulmonary bypass required to determine the optimal operation. This is an important consideration since the bypass occasions for these sufferers are typically extended because of the technical complexity. In this variant, only fibrous versus muscular conal septum separates the leaflets of the pulmonary and aortic valves. The pathophysiology is predominantly left-to-right shunting with pulmonary overcirculation. Series of views of a pathologic specimen demonstrating Taussig-Bing anomaly with interrupted aortic arch. These pictures are all from the same specimen, which has been opened from totally different views sick each view to reveal different anatomic parts optimally. The ductus arteriosus supplies the descending aorta and the left subclavian artery. For patients with complex aortic arch anatomy, angiography might further outline related aortic arch coarctation, hypoplasia, or interruption.
Second natural history study of congenital coronary heart defects: results of remedy of sufferers with ventricular septa defects antifungal amazon 150 mg diflucan for sale. Transcatheter closure of congenital ventricular septal defects: outcomes of the European Registry antifungal detergent diflucan 150 mg discount free shipping. Long-term outcome of transcatheter secundum-type arrial septal defect closure using Amplatzer septal occluders vinegar for fungus gnats 150 mg diflucan purchase with amex. Outcomes of being pregnant in ladies with congenital heart disease: a literature review. Has there been any progress made on pregnancy outcomes among girls with pulmonary arterial hypertension Long-term survival of sufferers with restore of tetralogy of Fallot: 36-year follow-up of 490 survivors of the primary 12 months after surgical restore. Risk components for sudden death after restore of tetralogy of Fallot, Ann Thorac Surg 2003;seventy six: 1901-195. Magnetic resonance imaging to assess the hemodynamic results of pulmonary valve alternative in adults late after repair of tetralogy of fallot. Pulmonary valve alternative in adults late after restore of tetralogy of Fallot: are we working too late Advanced therapy could delay the necessity for transplantation in sufferers with the Eisenmenger syndrome. Lung and heart-lung transplantation in children and adolescents: a long-term single-center expertise. Twenty-year expertise of lung transplantation at a single middle: Influence of recipient diagnosis on longterm survival. The Copenhagan National Lung Transplant Group: survival after single lung, double lung, and heart-lung transplantation. Percutaneous pulmonary valve implantation in humans: ends in 59 consecutive sufferers. Impact of pumonary valve replacement on arrhythmia propensity late after restore of tetralogy of Pallor. Atrial arrhythmias in adults after restore of tetralogy of Fallot; correlations with scientific, train, and echocardiographic findings. Intrinsic histological abnormalities of aortic root and ascending aorta in tetralogy of Fallot: proof of causative mechanism for aortic dilatation and aortopathy, Circulation 2005;112:961-968. Cardiac rhythm after the Mustard operation for full transposition of the great arteries. Second pure historical past study of congenital heart defects: results of remedy of patients with pulmonary valvular stenosis. Long-term outcome after the Mustard repair for easy transposition of the great arteries. Atrial baffle procedures for complete transposition of the good arteries: pure course of sinus node dysfunction and threat factors for dysrhythrnias and sudden dying. Sudden dying and defibrillators in transposition of the nice arteries with intra-atrial baffles: a multicenter examine. Predictors of sudden cardiac death after Mustard or Senning repair for transposition of the good arteries. Radiofrequency catheter ablation of supraventricular tachycardia substrates after mustard and senning operations for d-transposition of the good arteries. Long-term hemodynamic and electrocardiographic evaluation following operative repair of tetralogy of Fallot. Detection of late arrhythmia and conduction disturbance after correction of tetralogy of Fallot. Interventions in leaks and obstructions of the interatrial baffle late after Mustard and Senning correction for transposition of the great arteries. Long time period outcome as much as 30 years after the Mustard or Senning operation: a nationwide multicentre study in Belgium. Right ventricular systolic function in adolescents and young adults after Mustard operation for transposition of the great arteries. Regression of tricuspid regurgitation after two-stage arterial swap operation for failing systemic ventricle after atrial inversion operation. Surgical administration of late right ventricular failure after Mustard or Senning repair. Long-term results of left ventricular reconditioning and anatomic correction for systemic right ventricu- 1493 139. Cardiac outcomes in young grownup survivors of the arterial swap operation for transposition of the great arteries. Pulmonary valve eccentricity in d-transposition of the good arteries: implication for arterial change operation. Results of the Bruce treadmill check in youngsters after arterial swap operation for simple transposition of the great arteries. Coronary occasions after arterial change operation for transposition of the good arteries. Long-term consequence and quality of life in grownup patients after the Fontan operarion. Frequency of late recurrence of intra-atrial reentry tachycardia after radiofrequency catherer ablation in sufferers with congenital coronary heart disease. Long-term survival, modes of dying, and predictors of mortality in patients with Fontan surgical procedure. Protein-losing enterophathy after the Fontan operation: an international multicenter examine. Perioperative danger components for development of protein-losing enteropathy following a Fontan procedure. Protein-losing enteropathy: integrating a new illness paradigm into recommendations for prevention and therapy. Late hepatic complications after Fontan operation; non-invasive markers of hepatic fibrosis and threat elements. Second pure history examine of congenital coronary heart defects: quality of lifetime of patients with aortic stenosis, pulmonary stenosis or ventricular septal defect. Task Force 9: training in the casre of grownup sufferers with congenital heart illness. Characteristics of the special care services for adults with congenital heart disease. Discussions regarding contraception and pregnancy ought to begin as quickly as adolescent girls reach an age when they may become sexually energetic. This assessment ought to include a full review of the underlying cardiac lesion and prior surgical procedures, willpower of the chance of pregnancy, and improvement of plans for cardiac interventions previous to pregnancy when indicated. Because the severity of a low-risk situation could also be misinterpreted or given undue importance, even women with low-risk cardiac lesions often profit from preconceptual counseling. Unfortunately, amongst girls with congenital heart illness preconception counseling is often not supplied and data of risks of contraception and being pregnant is usually suboptimal (1-3). The heart specialist plays a crucial function by providing and/or guaranteeing informed training of the patient, her companion, and her caregivers. As properly, preexisting heart disease may first be revealed throughout pregnancy when the center is challenged by an elevated hemodynamic burden. Blood volume will increase during being pregnant; the rise begins as early because the sixth week of gestation and peaks at an average of 50% more than the prepregnant state by the top of the second trimester (5,6) though individual increases range between 20% and 100 percent above prepregnant blood volume (7). Systemic (peripheral) vascular resistance decreases starting within the fifth week of gestation. This mediates a decrease in systemic arterial pressure that begins within the first trimester and reaches its nadir in midpregnancy, after which blood pressure stabilizes (11,12). Placental blood circulate will increase until in regards to the 25th week of gestation after which stays unchanged. Renal blood move also increases, accompanied by a 50% improve in glomerular filtration price (13). Cardiac output increases during being pregnant as a outcome of increases in each coronary heart fee and stroke quantity. Most of the early improve in cardiac output is a results of progressive improve in stroke quantity, whereas later in being pregnant the guts fee effect becomes extra necessary because the stroke quantity stabilizes while the guts fee continues to rise (11,14). The mean coronary heart price will increase to roughly 10 to 20 beats above prepregnancy ranges by term. Increase in cardiac output begins as early as the fifth week of gestation, reaches its zenith near the end of the second trimester, typically after the 24th week of gestation and then plateaus till time period at 30% to 50% above prepregnancy levels (11,15-17).
Long time period outcomes of percutaneous balloon valvuloplasty of congenital aortic stenosis: impartial predictors of consequence fungus yeast treatment 50 mg diflucan with visa. Aortic valvuloplasty in pediatric patients considerably postpones the necessity for aortic valve surgical procedure: a singlecenter experience of 188 sufferers after up to fungus and algae symbiotic relationship 400 mg diflucan quality 17 zeasorb antifungal powder diflucan 50 mg order visa. Aortic valve reinterventions after balloon aortic valvuloplasty for congenital aortic stenosis. Long-term mortality, cause of dying, and temporal tendencies in problems after percutaneous aortic balloon valvuloplasty for calcific aortic stenosis. Reappraisal of percutaneous aortic balloon valvuloplasty as a preliminary remedy technique in the transcatheter aortic valve implantation era. Indications for cardiac catheterization and intervention in pediatric cardiac disease: a scientific assertion from the American Heart Association. Familial membranous subaortic stenosis: evaluate of familial inheritance sample and a case report. Rapid evolution from "regular" left ventricular outflow tract to deadly subaortic stenosis in infancy. Potential role of mechanical stress in the etiology of pediatric heart illness: septal shear stress in subaortic stenosis. Abnormalities of the left ventricular outflow tract related to discrete subaortic stenosis in kids: an echocardiographic study. Tetralogy of Failor with extreme left ventricular outflow tract obstruction due to attachment of the mitral valve to the ventricular septum. Discrete subaortic stenosis: the value of cross-sectional sector echocardiography in evaluating different types of obstruction. Two-dimensional echocardiographic options with angiographic and surgical correlation. Mechanism of early systolic closure of the aortic valve in discrete membranous subaortic stenosis. Diagnosis of discrete subaortic stenosis by pulsed and continuous wave echocardiography. Serial hemodynamic observations in congenital valvular and subvalvular aortic stenosis. Natural historical past and surgical outcomes for isolated discrete subaortic stenosis in children. Discrete subaortic stenosis in adults: elevated prevalence and sluggish fee of development of the obstruction and aortic regurgitation. Natural history and risk stratification of discrete subaortic stenosis in kids: an echocardiographic study. Early experience with percutaneous transcatheter implantation of heart valve prosthesis for the remedy of end-stage inoperable patients with aortic stenosis. Left heart obstructive lesions and left ventricular development in the midtrimester fetus: a longitudinal examine. Critical aortic stenosis in early infancy: anatomic and echocardiographic substrates of successful open valvotomy. Critical aortic stenosis within the neonate: a multi-institutional research of management, outcomes, and danger factors. Echocardiographic hemodynamic and morphometric predictors of survival after two-ventricle restore in infants with crucial aortic stenosis. Borderline hypoplasia of the left ventricle in neonates: insights for decision-making from functional assessment with magnetic resonance imaging. Contemporary results of balloon valvuloplasty and surgical valvotomy for congenital aortic stenosis. Are outcomes of surgical versus transcatheter balloon valvotomy equivalent in neonatal critical aortic stenosis The Ross/Konno procedure in neonates and infants: intermediate-term survival and autograft operate. Ross-Konno operation with resection of endocardial fibroelasrosis for important aortic stenosis with borderline-sized left ventricle in neonates. Discrete subaortic stenosis: incidence, morphology and surgical impact of associated subaorric anomalies. The genetics and pathology of discrete subaortic stenosis in the Newfoundland canine. Surgery for discrete subvalvular aortic stenosis: actuarial survival, hemodynamic outcomes, and purchased aortic 1043 regurgitation. The syndrome of supravalvular aortic stenosis, peripheral pulmonary stenosis, mental retardation and similar facial appearance. Complete physical map of the widespread deletion region in Williams syndrome and identification and characterization of three novel genes. The aortic root in supravalvular aortic stenosis: the potential surgical relevance of morphologic findings. A developmental complex together with supravalvar stenosis of the aorta and pulmonary trunk. A 20-year clinical perspective with patch aortoplasty, Am] Cardiel 1983;fifty one: 256-260. Progressive left main coronary artery obstruction leading to myocardial infarction in a baby with Williams syndrome. Generalized arterial fibromuscular dysplasia and myocardial infarction in familial supra valvular aortic stenosis syndrome. Pathology of coronary arteries, myocardium, and great arteries in supra valvular aortic stenosis. Myocardial infarction resulting in sudden dying in Williams syndrome: report of three instances. Forty-one years of surgical expertise with congenital supra valvular aortic stenosis. An clarification of uneven upper extremity blood pressures in supra valvular aortic stenosis. Natural course of supravalvar aortic stenosis and peripheral pulmonary stenosis in Williams syndrome. Three decades of follow-up of aortic and pulmonary vascular lesions in the Williams-Beuren syndrome. Diagnosis and post-operative analysis of supravalvular aortic stenosis by magnetic resonance imaging. The pure course of supravalvar aortic stenosis and peripheral pulmonary artery stenosis in Williams syndrome. Acute aortic insufficiency complicating stent treatment of supra valvular aortic stenosis: profitable release of trapped leaflets by wiring the stent. Surgical management of left coronary artery ostial atresia and supravalvar aortic stenosis. Extended aortic and left main coronary angioplasty with a single pericardial patch in a affected person with Williams syndrome. However, considerable variation exists in coarctation anatomy as well as in its pathophysiology, scientific presentation, remedy choices, and outcomes. For instance, though typically a discrete stenosis, coarctation could additionally be a protracted section in nature, could additionally be related to hypoplasia of the transverse aortic arch (common in infancy), or may be belly in location. The pathophysiology of coarctation varies with the severity of the stenosis, and in addition is affected by the presence of related lesions, similar to patent ductus arteriosus, ventricular septal defect, or left ventricular outflow obstruction. The scientific presentation of coarctation also varies, ranging from heart failure in infancy to asymptomatic hypertension and/or a murmur in an older baby or grownup. Treatment options include surgical procedure (most commonly resection and end-to-end anastomosis) and percutaneous balloon angioplasty and stenting. In many patients, the late prognosis is affected by residual coarctation stenosis or arch hypoplasia, related intracardiac pathology, and resting or train hypertension. The gross morphology of coarctation includes an intimal and medial malformation and a outstanding posterior infolding (the posterior shelf), which, in some circumstances, extends around the whole circumference of the aorta (10). In infants, notably these with related left-ventricular outflow obstruction or a ventricular septal defect, there could also be diffuse hypoplasia of the transverse aortic arch. Less generally, coarctation of the aorta happens in other areas, such as the ascending aorta or the abdominal aorta. Coarctation of the stomach aorta is a posh long-segment stenosis that typically is associated with renal artery stenosis. Histologic examination reveals thick intimal and medial ridges that protrude posteriorly and laterally into the aortic lumen.






