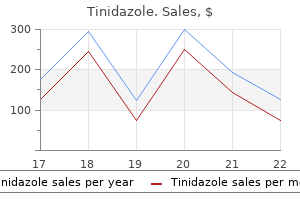
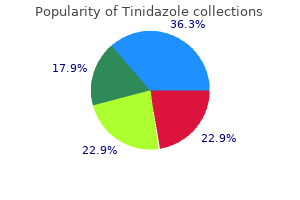
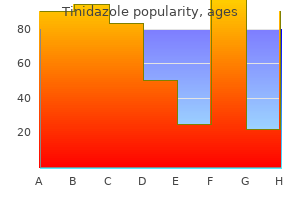
Tinidazole
Tinidazole
Tinidazole dosages: 1000 mg, 500 mg, 300 mg
Tinidazole packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Inadvertent tears or electrocautery burns can happen outdoors the visual field in both open and laparoscopic instances antibiotics bad for you 300 mg tinidazole buy with visa, and can have devastating postoperative consequences antimicrobial resistance ppt 500 mg tinidazole discount overnight delivery. Adhesive small bowel obstruction within the United States: has laparoscopy made an impression Abdominal adhesiolysis: inpatient care and expenditures in the United States in 1994 antibiotics for dogs online tinidazole 500 mg purchase amex. Novel opioid antagonists for opioid-induced bowel dysfunction and postoperative ileus. Systemic prokinetic pharmacologic therapy for postoperative adynamic ileus following stomach surgery in adults. Value of Gastrografin in adhesive small bowel obstruction after unsuccessful conservative remedy: a potential evaluation. Systematic review and meta-analysis of the diagnostic and therapeutic role of water-soluble contrast agent in adhesive small bowel obstruction. Letting the solar set on small bowel obstruction: can a simple risk score inform us when nonoperative care is inappropriate Small bowel obstruction is a surgical illness: patients with adhesive small bowel obstruction requiring operation have less expensive care when admitted to a surgical service. Trials of nonoperative management exceeding three days are related to elevated morbidity in patients undergoing surgery for uncomplicated adhesive small bowel obstruction. Early operation is related to a survival profit for sufferers with adhesive bowel obstruction. Laparotomy for small-bowel obstruction: first selection or last resort for adhesiolysis Laparoscopic compared with conventional therapy of acute adhesive small bowel obstruction. Laparoscopic versus open surgical management of adhesive small bowel obstruction: a comparability of outcomes. Long-term follow-up and price analysis following surgical procedure for small bowel obstruction caused by intra-abdominal adhesions. Nonoperative management of small-bowel obstruction with endoscopic lengthy intestinal tube placement. Accuracy of abdominal radiography in acute small-bowel obstruction: does reviewer experience matter Evaluation and management of small-bowel obstruction: an Eastern Association for the Surgery of Trauma follow management guideline. The management of patients with suspected early postoperative small bowel obstruction. Upper gastrointestinal distinction research in the management of small bowel obstruction-a potential randomised research. Clinically, volvulus refers to a larger than 180-degree twisting of a hole organ about its mesentery, leading to luminal obstruction, impaired venous return, and eventually ischemia and perforation. The consumption of large rare meals consisting of vegetables and high-fiber together with manual labor in an upright place has been postulated to account for this condition. This causes luminal obstruction, impaired venous return, and eventually ischemia and perforation. Volvulus of the small bowel is more frequent in kids, is most often secondary to malrotation, and is the cause for 1% of adult small bowel obstructions within the United States. Most patients present emergently (89%) with indicators and symptoms of acute small bowel obstruction, with 19% presenting with an acute abdomen. Although not specific or delicate, pain out of proportion to the physical findings should increase suspicion of vascular compromise and bowel ischemia, as ought to fever, tachycardia, peritoneal indicators, acidosis, and leukocytosis. As volvulus is a closed-loop obstruction, the bowel loops may be full of fluid and have little or no air and plain abdominal films could reveal a gasless lower abdomen. Gastrointestinal distinction research might present a corkscrew sample or an abrupt "fowl beak" on the level of obstruction, and angiography could demonstrate a spiraling sample of the mesenteric vessels described because the "barber pole" signal. The proximal afferent loop of bowel leading into the closed loop dilates, and the departing efferent phase collapses. Thus there are three dilated loops: two fashioned by the closed loop and the third by the proximal afferent loop, with all three loops tapering abruptly on the level of torsion, giving rise to the "chook beak" signal. Gangrenous bowel requires the appropriate segmental resection, with most collection advocating main anastomosis. For sufferers without ischemic bowel, the optimal surgical remedy is less clear. Most case series describe easy detorsion of the volvulus without resection, though no long-term follow-up is out there to determine recurrence fee. To stop recurrent volvulus, some authors have described bowel resection in the absence of gangrene whereas others have carried out intestinopexy of long segments of bowel. These procedures run the chance of brief intestine syndrome and elevated threat of adhesive bowel obstruction and have to be used with warning. The normal stomach is a really cellular intraabdominal organ and intermittently rotates without symptoms or sequelae. The right orientation of the stomach is maintained by its 4 anchoring ligaments (gastrohepatic, gastrocolic, gastrophrenic, and gastrosplenic) together with the gastroesophageal junction and the retroperitoneal duodenum. Failure of these gastric attachments may be the outcomes of agenesis, elongation, or disruption and may predispose the stomach to volvulize. The anatomic classification as proposed by Singleton50 in 1940 consists of (1) organoaxial rotation, (2) mesenteroaxial rotation, or (3) mixed- combination of the 2. In most instances the antrum rotates anteriorly and superiorly and the fundus posteriorly and inferiorly, twisting the larger curvature, which involves lie superior to the lesser curvature. The pylorus rotates anteriorly and superiorly (more common) or posteriorly from right to left in order that the posterior floor of the abdomen lies anterior. In 1904 Bouchardt61 described the triad of severe epigastric pain and distention, vomiting adopted by retching with an inability to vomit, and problem or inability to pass a nasogastric tube. This triad indicates an preliminary block at the pylorus, then on the cardia and later gastric distention as closed-loop obstruction develops. The higher curvature is intrathoracic, and the pylorus is in close proximity to the usually positioned gastroesophageal junction. Mortality rates as excessive as 30% to 50% have been reported for this condition, with the most important reason for dying being sepsis secondary to gastric strangulation. Small bowel volvulus: a standard explanation for mechanical intestinal obstruction in our region. Small bowel volvulus with intussusception: an unusual revelation of neuroendocrine tumor. Small bowel volvulus induced by mesenteric lymphangioma in an adult: a case report. The quick gastric vessels ought to be preserved, if potential, both to retain their blood supply and to assist to anchor the greater curvature. In septic or medically high-risk patients, discount and gastropexy alone could additionally be safer and enough, significantly in those with limited life expectancy. It is difficult to know the share of sufferers with a diaphragmatic hernia and intrathoracic stomach who will progress to acute gastric strangulation. However, the high morbidity and mortality associated with strangulation justify expeditious restore, even in asymptomatic sufferers. After the abdomen has been reduced, gastropexy could be achieved by placement of a percutaneous endoscopic gastrostomy tube. Laparoscopic and combined laparoscopic and endoscopic approaches have the potential to combine minimally invasive strategies with restore of the diaphragmatic defect. Small bowel volvulus within the grownup populace of the United States: results from a population-based research. Wandering spleen with gastric volvulus and intestinal non-rotation in an grownup male patient. Rare persistent gastric volvulus related to left atrial and mediastinal compression. Gastric wall necrosis from organo-axial volvulus as a late complication of laparoscopic gastric banding. Gastric volvulus as a complication within the recipients after adult living donor liver transplantation. Chronic and recurrent volvulus of the stomach with late outcomes of "colonic displacement".
The liver can store up to infection jobs indeed 1000 mg tinidazole purchase with visa a most of 65 g of glycogen for each kilogram of liver tissue antibiotics for acne online tinidazole 500 mg order on line. Glucose for the brain and red blood cells is produced by means of gluconeogenesis antibiotics for acne yes or no tinidazole 300 mg buy fast delivery. In the liver, glycerol, quite than fatty acids, supplies the carbon source for gluconeogenesis. During extended starvation, glucose use by the brain decreases, and ketone bodies generated by the liver turn out to be the major source of energy. It receives approximately 1500 mL of blood per minute, 30% from the hepatic artery and the remaining 70% from the portal vein. There are 25 to 30 mL of blood per one hundred g of liver under regular conditions, but that quantity might reach up to 60 mL/100 g in cases of congestion. Blood flow also varies because of different physiologic conditions, corresponding to ingestion of a meal. Hepatocytes are additionally able to internalize giant proteins and different macromolecules by endocytosis. Nonessential amino acids are synthesized within the liver from pathways primarily based on pyruvate, -ketoglutarate, and oxaloacetate (from the Krebs cycle). The nitrogen from the amino groups is excreted as urea within the urine after being processed by the urea cycle. The capability of the liver to regenerate has provided sufferers and surgeons with multitude of remedy options that have advanced over many years. This functionality begins on the molecular level and was initially described within the 1960s in a partial hepatectomy animal model. To recover after harm, hepatocytes must preserve function whereas replicating at high frequency to maintain physiologic wants of patients. This capability is affected by exterior in addition to inside elements, which embody ischemia, preservation injury, steatosis of liver, and age. The fully differentiated hepatocytes are the means by which fast liver regeneration happens after a partial hepatectomy. Right dwelling donor liver transplantation-an choice for grownup patients: single-institution experience with seventy four sufferers. Anatomical and physiological comparability of liver volumes among three frequent forms of parenchyma transection in live-donor liver transplantation. Embryology for Surgeons: the Embryological Basis of the Treatment of Congenital Anomalies. Terminology of liver anatomy and liver resection: coming to grips with hepatic Babel. Its operate entails absorption and digestion of dietary substances, ldl cholesterol excretion, and the elimination of toxic substances. Sur les tuniques qui enveloppent certains visc�res, et fournissent des gaines membraneuses � leurs vaisseaux. Procurement of liver and pancreas allografts in donors with replaced/accessory proper hepatic arteries. Recherches sur la chirurgie du confluent biliaire sup�rieur et des canaux h�patiques. Anatomical and physiological classification of hepatic vein dominance utilized to liver transplantation. Bases anatomiques des h�patectomies droite et gauche: strategies qui en d�coulent. Experimental researches into a brand new excretory perform of the liver: consisting in the removing of cholesterine from the blood, and its discharge from the physique within the form of stercorine. Such sufferers may never actually develop liver disease, however approximately 20% of them ultimately evolve to have a particular liver-related diagnosis during long-term follow-up. On the other hand, a predominant elevation of serum alkaline phosphatase with or with out elevated bilirubin suggests a illness process that interferes with bile circulate into and thru the bile ducts. An isolated hyperbilirubinemia may represent an increase in bilirubin production, or problems in its conjugation or canalicular transport. The length of elevation can additionally be another important consideration because the differential analysis for an acute, shorter process can be completely different from a persistent, longer-lasting disease (Table 119. Although serum levels of aminotransferases are elevated to a point in virtually all liver diseases, the very best levels are seen with acute viral hepatitis, toxin-induced hepatic necrosis, and ischemic liver harm. The remaining synthetic perform of the liver is extra precisely measured by the prothrombin time, which serves as the best software for predicting hepatic end result. Patients who bear surgical procedure may have preexisting liver diseases, which in some cases might influence the operation itself or the postoperative course. Others may develop acute and important hepatic dysfunction within the postoperative period, calling for a full investigation into the etiology to allow for appropriate management. The interpretation of irregular liver chemistry tests should be guided by the sample and acuity of the elevations, which can narrow the differential diagnoses to some extent. This must also be accomplished in the context of the clinical setting, incorporating the historical past, bodily examination, different laboratory tests, and radiologic research into the picture. Infiltrative diseases of the liver typically additionally lead to a rise in serum alkaline phosphatase levels. Serum unconjugated bilirubin ranges increase in problems that lead to overproduction of unconjugated bilirubin or in issues of the conjugation course of. It is discovered within the canalicular membrane of hepatocytes, in addition to in a variety of other tissues, including bone, gut, placenta, kidney, and leukocytes. Although modest elevations are seen in many types of hepatocellular disease, values that are threefold or extra above normal vary are indicative of bile duct obstruction or intrahepatic cholestasis. This enzyme catalyzes the transfer of -glutamyl teams from glutathione and different peptides to different amino acids. It is highly inducible by alcohol and medicines and may be elevated in certain medical circumstances corresponding to diabetes mellitus, renal failure, myocardial infarction, and chronic obstructive pulmonary illness. It has a half-life of approximately 20 days, which limits its utility as a synthetic marker throughout acute liver illness. It can be insensitive to gentle degrees of hepatic harm, but a major decline alerts a prolonged, and usually main, insult to the liver. Other elements that may have an result on the serum albumin levels embody nutrition and losses via the gastrointestinal and renal techniques. In sufferers with edema and ascites, the quantity of distribution for albumin could also be expanded, resulting in a reduction within the measured serum levels. The prothrombin time measures the speed of conversion of prothrombin to thrombin within the take a look at serum with added thromboplastin and calcium and indirectly assesses for the supply of the coagulation elements. Administration of parenteral vitamin K may help in differentiation of vitamin K deficiency from synthetic dysfunction of the liver. The analysis is usually made within the setting of both recognized hypotension or hypoxemia in critically sick or postoperative patients, and the absence of such threat factors ought to immediate a search for different etiologies, similar to viral hepatitis and drug damage. The majority of cases (79%) had a predisposing acute cardiac occasion, and sepsis was current in 23%. Intrinsic hepatotoxins embody brokers that cause liver damage by direct physicochemical results on the hepatocytes. Toxic hepatitis caused by intrinsic hepatotoxins is dose dependent and is mostly predictable in people uncovered to the offending agent. Hypersensitivity reactions resulting in hepatic damage develop inside 1 to 5 weeks of exposure to the offending agent, recur promptly on readministration of the agent (after one or two doses), and are normally accompanied by fever, rash, arthralgia, and eosinophilia. Drugs that will cause hypersensitivity reactions embody halothane, chlorpromazine, methyldopa, sulfonamides, phenytoin, and dapsone. Metabolically mediated hepatic harm outcomes from an aberrant metabolic pathway for the drug in a vulnerable patient, which ends up in the production of hepatotoxic metabolites. Drugs that will cause this sort of damage embody isoniazid, valproic acid, methyldopa, and perhexiline maleate. Acute liver failure can happen but is uncommon and should require liver transplantation or result in death. Cases that fulfill all these criteria have a 1 out of 10 chance of growing acute liver failure with a 10% to 50% mortality rate. Sulfonamides, macrolides, fluoroquinolones, tetracyclines, antifungal agents, and antiretroviral agents are additionally commonly associated with drug-induced cholestasis, along with antiinflammatory agents and a few psychotropes. A few medication, corresponding to oral contraceptives and anabolic steroids, trigger bland cholestasis. Vanishing bile duct syndrome, diagnosed by liver biopsy, has a protracted course of persistent bile duct harm that ultimately results in bile duct loss. Sclerosing cholangitis outcomes from damage to the hepatic arterioles that offer the biliary radicles, inducing ischemic cholangiopathy that manifests as biliary strictures.
A running approach for this suture is a useful alternative and avoids the location of intraluminal knots antibiotics gastritis best tinidazole 1000 mg. At the completion of the hepaticojejunostomy 001 bacteria tinidazole 1000 mg generic on line, the retrocolic tunnel and the mesenteric defects are repaired antibiotic bactrim uses order tinidazole 300 mg free shipping. A single, closed-suction drain is positioned posterior to the anastomosis, exiting via the side of the infant. A needle biopsy of the liver is all the time obtained on the time of operation to doc the diploma of hepatic irritation and fibrosis. Analysis of this tissue could turn out to be very helpful in figuring out the postoperative medical management. Biliary diversion or formation of one-way valves in the Roux limb has not measurably altered the development of this disease to biliary cirrhosis, although the incidence of cholangitis could also be decreased. Placement of the initial incision must be guided by ultrasound location of the porta or palpation of the liver under common anesthesia. Malrotation may be discovered related to the syndrome and may make retrocolic placement of the Roux limb unimaginable. Abnormalities of hepatic arterial supply and the presence of a preduodenal portal vein should be anticipated and recognized throughout portal dissection. Placement of the hepaticojejunostomy is guided by identification of the portal vein bifurcation. Reports of a laparoscopic approach to hepatoportoenterostomy are discovered in the literature with preliminary favorable outcomes. This clinical scenario is normally precipitated by cholangitis with subsequent damage to bile ducts and decreased bile flow because of that injury and the effect of an infection on bile manufacturing. That process could be very difficult and should lead to vascular damage to the portal vein or hepatic artery. Subsequently, the effect of repeated Kasai procedures is deleterious for liver transplantation. That process is undertaken just as it would be for an infant who may have biliary atresia. The gallbladder is usually regular or small in caliber and often incorporates bile, although it might be dilute. Once a catheter is secured within the dome of the gallbladder, injection of the contrast is performed with fluoroscopic visualization of the distinction injection. Contrast is often seen flowing into the duodenum, however the extrahepatic biliary constructions and the intrahepatic ducts are fairly small. No additional operative remedy is performed, and the incision is closed with no drain after suture closure of the gallbladder with absorbable sutures. Bile circulate could also be gradual at first and not reach regular proportions for several months. A medical routine of corticosteroids, ursodeoxycholic acid, and prophylactic antibiotics to prevent cholangitis appears to improve and sustain bile move. Wide variation is found in selection and length of treatment with antibiotics, steroids, and ursodeoxycholic acid. Systemic antibiotics and elevated corticosteroids may end in improved bile flow. At one time, repeat operation was advocated for infants who had drained bile initially and subsequently became jaundiced. This therapy is no longer advocated as a result of it has not had a excessive price of success. Nutritional requirements for all biliary atresia sufferers are greater than regular and especially so for many who stay jaundiced. In the syndromatic situation, the seek for associated anomalies includes session by ophthalmology, cardiology, nephrology, and gastroenterology. The child will require long-term follow-up to assess their progression of liver illness. Most challenging for the kid facing liver transplantation is the inadequacy of the donor organ pool. Segmental transplantation from cadaveric or stay donors can meet this want but is neither universally practiced nor possible without the cooperation of grownup transplant surgeons. Liver transplantation, whether or not previous to or after hepatoportoenterostomy, is simple, although technically difficult. Hepatic artery and portal vein anastomoses are facilitated by working loupes or microscope. Patient and graft survival charges are excellent; greater than 90% of youngsters are alive at 1 year, and of those, most are alive at 10 years. Sequential treatment of biliary atresia with Kasai portoenterotomy and liver transplantation: a review. Biliary atresia: surgical management and treatment choices as they relate to outcome. Syndromatic paucity of interlobal bile ducts (Alagille syndrome or arteriohepatic hypoplasia): evaluation of 80 instances. Technical innovation for noninvasive and early prognosis of biliary atresia: the ultrasonographic "triangular twine" sign. Design and validation of the biliary atresia research consortium histologic evaluation for cholestasis in infancy. Biliary atresia and other structural anomalies in congenital polysplenia syndrome. The anatomic pattern of biliary atresia at time of Kasai hepatoportoenterostomy and early postoperative clearance of jaundice are important predictors of transplant-free survival. Prognostic value of computerized quantification of liver fibrosis in children with biliary atresia. A recent systematic review of native liver survival with out transplantation at 10 years ranged between 24% and 52. Almost one-third of sufferers have solely modest or no improvement in the jaundice after hepatoportoenterostomy. Liver transplantation is the next line of therapy for the jaundiced child and for those with the sequelae of progressive liver disease. Transplantation could also be required in infancy because of the lack to obtain bile drainage with hepatoportoenterostomy or on the time of preliminary diagnosis if end-stage liver disease is current. Randomized, double-blind, placebo-controlled trial of corticosteroids after Kasai portoenterostomy for biliary atresia. Should open Kasai portoenterostomy be performed for biliary atresia in the period of laparoscopy Effect of repeat Kasai hepatic portoenterostomy on pediatric live-donor liver graft for biliary atresia. On the other hand, pancreaticobiliary maljunction, which was first famous by Kozumi and Kodama8 in an autopsy case with congenital biliary dilatation in 1916, is a congenital anomaly outlined as an abnormal union of the pancreatic and biliary ducts. Incidence Congenital biliary dilatation has usually been thought-about a rarity, however just lately the number of instances reported in the literature has steadily increased. In 1936 Yotuyanagi15 instructed that inequality within the proliferation of epithelial cells of the higher portion and the decrease portion of the widespread bile duct in the primitive stage may produce an abnormally dilated structure following recanalization. On the other hand, pancreaticobiliary maljunction is believed to develop as a misarrangement of the embryonic connections in the pancreaticobiliary ductal system, with the terminal bile duct joined to the second branch of the ventral pancreas. History Congenital biliary dilatation is characterised by localized dilatation of the choledochus and is associated with pancreaticobiliary maljunction. Todani refined the classification of bile duct cystic disorders into five sorts and included the concept of pancreaticobiliary maljunction. The major clinical signs are recurrent abdominal ache, nausea and vomiting, mild jaundice, an belly mass, and fever. Diagnosis of congenital biliary dilatation requires demonstration of abnormal dilatation of the bile duct and pancreaticobiliary maljunction on the idea of diagnostic imaging or anatomic abnormalities. The major issues are biliary stones, pancreatitis, spontaneous perforation of the bile duct, and carcinoma. Accordingly, the definitive treatment of congenital biliary dilatation is complete excision of the extrahepatic bile duct with Roux-en-Y hepaticojejunostomy.
Significant long-term pain reduction together with weight acquire and decreased narcotic dependence are achieved in a majority of sufferers who bear operative remedy antimicrobial activity 1000 mg tinidazole effective. However antibiotics for uti that start with m purchase 1000 mg tinidazole with amex, the optimal selection of particular surgical options in numerous settings is less clear virus 0 access tinidazole 1000 mg cheap online. Both procedures had been equally efficient in terms of pain relief and determination of problems to adjoining organs. Operative time and median hospital stay were shorter in patients who underwent the Berne modification. There were no variations in quality of life and ache control after a median follow-up of seven years. Treatment selections should be guided by affected person presentation however are hampered by the shortage of consensus pointers and by clinician bias. Therapeutic options embody risk modification, analgesic therapy, food plan, endoscopic therapy, and surgical remedy. Patients may be best handled in high-volume facilities with radiologic, endoscopic, and surgical experience, as nicely as an ancillary system of social employees, dietitians, and psychologists. Report of the Second International Symposium on the Classification of Pancreatitis in Marseille, France, March 28�30, 1984. Cigarette smoking as a danger factor for persistent pancreatitis: a case-control study in Japan. Potential carcinogenic results of cigarette smoke and Swedish moist snuff on pancreas: a study utilizing a transgenic mouse mannequin of persistent pancreatitis. Chronic pancreatitis associated with an activation peptide mutation that facilitates trypsin activation. Mutations in the cationic trypsinogen gene are associated with recurrent acute and continual pancreatitis. A sign peptide cleavage site mutation within the cationic trypsinogen gene is strongly related to continual pancreatitis. Mutations in exons 2 and 3 of the cationic trypsinogen gene in Japanese households with hereditary pancreatitis. Mutations in the gene encoding the serine protease inhibitor, Kazal type 1 are associated with continual pancreatitis. Variations in trypsinogen expression might affect the protective impact of the p. Pain, exocrine and endocrine pancreatic insufficiency and prognosis of the illness. Chronic pancreatitis and fracture: a retrospective, population-based Veterans Administration examine. Chronic pancreatitis is important for induction of pancreatic ductal adenocarcinoma by K-Ras oncogenes in adult mice. Effect of pancreaticojejunostomy on fibrosis, pancreatic blood circulate, and interstitial pH in chronic pancreatitis: a feline mannequin. A modified strategy of the Beger and Frey procedure in patients with chronic pancreatitis. Local resection of the pinnacle of the pancreas combined with longitudinal pancreaticojejunostomy within the administration of sufferers with continual pancreatitis. Total pancreatectomy and islet cell autotransplantation as a means of treating sufferers with genetically linked pancreatitis. Total pancreatectomy with and without islet cell transplantation for chronic pancreatitis: a sequence of eighty five consecutive patients. Factors related to insulin and narcotic independence after islet autotransplantation in patients with extreme persistent pancreatitis. Systematic evaluate of whole pancreatectomy and islet autotransplantation for chronic pancreatitis. Islet autotransplant outcomes after complete pancreatectomy: a contrast to islet allograft outcomes. Hospitalization, frequency of interventions, and quality of life after endoscopic, surgical, or conservative therapy in patients with persistent pancreatitis. A potential, randomized trial evaluating endoscopic and surgical therapy for persistent pancreatitis. Extended drainage versus resection in surgery for chronic pancreatitis: a prospective randomized trial evaluating the longitudinal pancreaticojejunostomy combined with native pancreatic head excision with the pylorus-preserving pancreatoduodenectomy. Long-term follow-up of a randomized trial comparing the Beger and Frey procedures for sufferers affected by continual pancreatitis. Long-term follow-up of a randomized medical trial evaluating Beger with pylorus-preserving Whipple procedure for chronic pancreatitis. Dynamic endoscopic manometry of the response to secretin in sufferers with persistent pancreatitis. Development and diagnostic accuracy of a breath check for pancreatic exocrine insufficiency in continual pancreatitis. Autoimmune-related pancreatitis is related to autoantibodies and a Th1/Th2-type cellular immune response. Prospective analysis of endoscopic ultrasonography and endoscopic retrograde cholangiopancreatography in patients with continual stomach pain of suspected pancreatic origin. A randomized managed trial of antioxidant supplementation for ache reduction in patients with continual pancreatitis. Long-term ache aid with optimized medical including antioxidants and step-up interventional therapy in sufferers with continual pancreatitis. Intrathecal narcotic infusion pumps for intractable ache of persistent pancreatitis: a pilot series. Endoscopic remedy of continual pancreatitis: a multicenter examine of one thousand sufferers with long-term follow-up. Success of extracorporeal shock wave lithotripsy in continual calcific pancreatitis management: a meta-analysis and systematic evaluate. Experience with resection of the pancreas in the remedy of chronic relapsing pancreatitis. Clinical end result in relation to timing of surgical procedure in chronic pancreatitis: a nomogram to predict pain relief. Is altered central pain processing related to illness stage in continual pancreatitis sufferers with pain Radical surgical procedure for sure instances of pancreatic fibrosis related to calcareous deposits. Pancreatoduodenectomy for chronic pancreatitis: long-term results in 105 sufferers. Duodenumpreserving head resection in persistent pancreatitis changes the natural course of the illness: a single-center 26-year expertise. Complications of adjacent organs in continual pancreatitis managed by duodenum-preserving resection of the head of the pancreas. Quality of life in continual pancreatitis-results after duodenum-preserving resection of the pinnacle of the pancreas. The consensus tips of the revised Atlanta classification of pancreatitis describe various features of acute pancreatitis, distinguishing between interstitial edematous pancreatitis and the more aggressive necrotizing pancreatitis (Table ninety three. A pancreatic pseudocyst is defined as a fluid assortment inside or adjoining to the pancreas that becomes fully encapsulated with a mature, nonepithelialized, fibrous, inflammatory wall. This strategy of acute pseudocyst formation requires no less than four weeks by definition. Acute necrotic collections usually form in the setting of necrotizing pancreatitis and are outlined as collections with variable quantities of fluid and necrosis, with no discrete encapsulating wall. Management of walled-off pancreatic necrosis is discussed in Chapter 94, though many of the same principles apply regarding stabilization of acute pancreatitis, pancreatic ductal analysis, and minimally invasive methods. Pancreatic fluid collections and pseudocysts occur in 40% and 5% to 15% of patients, respectively, as a consequence of acute pancreatitis. Any other etiologies of pancreatitis, corresponding to gallstones, trauma, and postprocedural points, also can result in pseudocysts. Biliary causes of pancreatitis extra typically lead to pseudocysts after acute pancreatitis, whereas alcohol is usually the purpose for pseudocysts in sufferers with continual pancreatitis. Release of inflammatory cytokines as part of the immunologic response of pancreatitis can lead to profound reactive fluid accumulation around the pancreatic parenchyma. These fluid collections are typically sterile and disappear with decision of the pancreatitis.
The affected person subsequently developed portal bacteria archaea eukarya purchase 1000 mg tinidazole visa, superior mesenteric treatment for sinus infection and bronchitis generic tinidazole 1000 mg visa, and splenic vein thrombosis antibiotic resistant uti in dogs order 1000 mg tinidazole fast delivery. The solely remnant of viable pancreas is the uncinate, resulting in the growth of diabetes. This adenocarcinoma of infancy consists of corpuscles of centrally localized squamous cells, an intermediate dark-staining zone of cells, and finally a peripheral rim of ductlike tubular constructions. A retrospective examine demonstrated enhancements in signs and in quality of life in seven of nine sufferers (average age: 13 years) who underwent the Frey procedure. They used a two-layer, side-to-side anastomosis between the opened pancreatic duct and a retrocolic, Roux-en-Y jejunal limb. These authors found significantly decreased rates of hospitalizations after 1 and three years and a big gain in share of best body weight after 3 years. The Duval process (distal pancreatectomy with Roux-en-Y pancreaticojejunostomy) may also be indicated in some sufferers. Of the 18 patients, thirteen have been weaned totally off ache drugs and required no additional hospitalizations, with a mean follow-up of seven. No declare may be made as to the relative superiority of one operative method over the other. As a common precept, pancreatic tumors in youngsters are properly demarcated somewhat than infiltrative. Patients are usually asymptomatic; nonetheless, presenting indicators and signs in pediatric patients could embrace a mass, ache, weight loss, or hypoglycemia, but jaundice is a much much less common presentation than is skilled with adults. Other pancreatic lots and cysts such as neuroendocrine tumors, serous cystadenomas, and hydatid cysts can occur in kids, and their administration parallels that of the same situations in adults. Originally termed childish pancreatic carcinoma, these tumors comprise each epithelial and stromal elements. Histologic prognosis may not be easy, and thus obtaining enough tissue to perform molecular diagnostic research could additionally be important. Solid pseudopapillary tumors happen in all areas of the pancreas with equal frequency. Depending on location, pancreaticoduodenectomy, central pancreatectomy with anastomosis of the distal portion to a Roux-en-Y jejunal loop, and distal pancreatectomy have every been utilized. However, primarily based on recent case stories with follow-up, select cases may be treated by a minimally invasive method and tissue-sparing resection. Blunt harm to the pancreas in kids usually occurs within the setting of three characteristic mechanisms. The administration of intravenous distinction is important to suitably visualize stable organ injury, however the utility of oral or intragastric distinction is debatable. Hemodynamic instability after volume resuscitation of 40 mL/kg (20 mL/ kg � 2) of crystalloid ought to prompt celiotomy, but this scenario is uncommon. Nonoperative management of pancreatic accidents has been reported in a number of case collection for the explanation that Nineteen Nineties. It is an epithelial tumor of low-grade malignant potential, occurring more incessantly in females of reproductive age that often presents as an asymptomatic large mass or with pain. Diagnosis may be made by fine-needle aspirate, which can be achieved at the time of endoscopic ultrasound in an adolescent affected person. A current evaluate of the National Trauma Database found that nonoperative administration of blunt pancreatic trauma in children is a feasible possibility with equivalent or higher outcomes in regard to death, size of stay, Intensive Care Unit size of keep, Intensive Care Unit use, and total problems. The distal duct presents more straightforward surgical options as a end result of a distal pancreatectomy could additionally be accomplished by normal suture or staple closure of the pancreatic remnant without the requirement for an enteric anastomosis. All which might be required is interval drainage of the doubtless resulting pseudocyst. Thus the healing of the ductal harm is attributed to decompression of the pancreatic duct as a whole. The investigators identified that these cases concerned ductal extravasation however not full-scale ductal transection. The remaining three required partial resection or operative treatment of a pseudocyst. Like open operative methods, these methods rely on the development of a rind across the pseudocyst cavity. Although the success price was higher than 90%, the authors reported a excessive complication fee of 33%. Ectopic drainage of the frequent bile duct into the lesser curvature of the gastric antrum in a new child with pyloric atresia, annular pancreas and congenital quick bowel syndrome. Recurrent pancreatitis brought on by pancreatobiliary anomalies in youngsters with annular pancreas. Nesidioblastosis of the pancreas: definition of the syndrome and the administration of the extreme neonatal hyperinsulinaemic hypoglycaemia. Pancreatic growth and function following surgical remedy of nesidioblastosis in infancy. The changing incidence of acute pan- creatitis in kids: a single-institution perspective. In- creasing incidence of acute pancreatitis at an American pediatric tertiary care middle: is greater consciousness amongst physicians responsible Epidemiology of acute pancreatitis in hospitalized children within the United States from 2000�2009. Cholelithiasis and its problems in kids and adolescents: replace and case dialogue. The modified Puestow procedure for sophisticated hereditary pancreatitis in youngsters. Primitive neuroectodermal tumors of the pancreas: a report of seven instances of a rare neoplasm. Malignant pancreatic tumors in childhood and adolescence: the Memorial Sloan-Kettering experience, 1967 to current. Primitive neuroectodermal tumor of the pancreas: a case report of an especially rare tumor. Persistent hyperinsulinaemic hypoglycemia of infancy: a heterogeneous syndrome unrelated to nesidioblastosis. Hyperinsulinism in youngsters: diagnostic worth of pancreatic venous sampling correlated with clinical, pathological, and surgical consequence in 25 circumstances. Partial elective pancreatectomy is healing in focal type of permanent hyperinsulinemic hypoglycemia in infancy: a report of forty five circumstances from 1983 to 2000. Fine-needle aspiration cytology of pancreatoblastoma with immunocytochemical and ultrastructural research. Internal drainage into an onlay-Roux-en-Y jejunal loop in isolated pancreatic injury with ductal transection: short-term and long-term follow-up in two pediatric instances. Complete disruption of the main pancreatic duct: a case successfully managed by percutaneous drainage. Laparoscopic prognosis and treatment of hyperinsulinism in two cases of focal adenomatous hyperplasia in infancy. Growth and endocrine function after near total pancreatectomy for hyperinsulinaemic hypoglycaemia. Long-term complication following subtotal pancreatectomy for nesidioblastosis: a case report. Variceal hemorrhage 18 years after pancreatectomy for nesidioblastosis: a case report and dialogue. Congenital anomaly of pancreas divisum as cause of obstructive pain and pancreatitis. Pancreas divisum and stenosis of the main and minor papillae in an eight-year-old girl: remedy by twin sphincteroplasty. The use of endoscopic ultrasound in the analysis of stable pseudopapillary tumors of the pancreas in kids. Long-term end result after nonoperative management of full traumatic pancreatic transection in youngsters. Operative vs nonoperative management of pediatric blunt pancreatic trauma: evaluation of the National Trauma Data Bank. Treatment of pancreatic duct disruption in children by an endoscopically placed stent. Successful endoscopic drainage of a posttraumatic pancreatic pseudocyst in a baby. Although the intensive therapy group benefited from lowered long-term complications, the risk of severe hypoglycemia, which compromised life quality related to tight glycemic management, was 3 times higher than in the conventional therapy group. Successful -cell replacement therapy within the type of pancreas or islet transplantation presents some great advantages of attaining regular or near-normal blood glucose control with out the risks of severe hypoglycemia associated with intensive insulin therapy.
Cutting balloons have been used with some success; nevertheless antibiotics for uti in puppies buy generic tinidazole 1000 mg, knowledge on safety and efficacy are nonetheless limited antibiotic 1 hour prior to incision purchase tinidazole 500 mg overnight delivery. An exterior pigtail drain is then left in place and capped externally for a trial of a quantity of weeks infection zombie movies generic 1000 mg tinidazole. Successful drain removing was achieved in 87% of patients who completed a full remedy period of 6 to 12 months of sequential upsizing and dilation with a stricture patency fee of 84% at 1 12 months, 74% at 5 years, and 67% at 10 years. These devices are everlasting and irretrievable as a end result of they induce intimal hyperplasia and turn out to be embedded within the biliary epithelium. Bare metallic stents also have a excessive rate of occlusion and are thus solely used for palliation in malignant disease. These gadgets are covered in a material that delays intimal hyperplasia and allows for simple removal. A current research of sixty eight sufferers who have been treated percutaneously with covered stents showed a scientific success rate of 87% in patients with each primary and refractory strictures and a patency rate of 91% at 1 year. Sphincterotomy or (less commonly) sphincteroplasty is performed with cholecystectomy to clear the frequent bile duct. When an endoscopic approach fails due to anatomic anomalies, alternative treatment for frequent bile duct stones could be pursued through either the postoperative drain (T tube or transcystic) positioned during cholecystectomy or via a transhepatic method. Success charges are reported at larger than 95%, with the most common complication, cholangitis, occurring in lower than 3% of instances. The balloon catheter is then deflated, reinflated proximal to the stone, after which used to push the stones into the duodenum. Success rates are reported as high as 97%, with the major complications, bile leak after tube removing, occurring in less than 10% of patients. Palliative aid of pruritus and management of cholangitis could be obtained by way of placement of percutaneous biliary drainage catheters, endoscopic or percutaneous biliary stenting, and surgical bypass. Internal-external drain was placed in the acute setting to enable decompression of the biliary system. A cholangiogram was carried out over a guidewire in preparation for stent deployment. Covered biliary stents exhibit improved patency compared with noncovered metallic stents, though the rate of stent migration and acute cholecystitis is increased. Primary stenting has been found to be more practical with fewer issues in contrast with secondary stenting, which is a staged process. The grading system could be helpful for both the determination of tumor resectability and planning for the drainage process. Multiple studies have evaluated the impact of the optimum location and variety of stents necessary to adequately drain an obstructed biliary system. Drainage and stenting of a single complete lobe is typically sufficient; however, draining several segments in one lobe is often not enough and will lead to elevated complication rates. Major issues associated to percutaneous biliary interventions embrace arterial bleeding, pseudoaneurysm formation, and biliary sepsis. Together, these could result in erosion of the blood vessel wall, resulting in pseudoaneurysm formation and eventually hemobilia upon rupture into an adjoining bile duct. On the other hand, biliary-venous communications usually have a tendency to cease spontaneously, owing to the low-pressure gradient, though venous hemobilia can nonetheless happen, significantly within the setting of portal hypertension. Treatment is usually conservative in these instances and may start with correcting any underlying coagulopathies. A trial of capping of the drain may facilitate hemostasis by eliminating an outlet for hemorrhage. Imaging is important for the diagnosis and planning of bile duct injuries, with each modality contributing completely different advantages and limitations. Bilomas might result in serious issues, such as an abscess formation, cholangitis, and sepsis. Single or bilateral percutaneous biliary drains may be required in bile duct injuries. U tube placement could also be thought of in patients requiring each biliary diversion and biliary drainage. A U tube is a simple straight drain with a quantity of side holes and two percutaneous exits. Blunt stomach trauma is commonly related to injuries of the gallbladder, common bile duct, and the intrahepatic ducts. Cholangiography in these circumstances hardly ever reveals a vascular communication as a outcome of the direction of bleeding is into the bile duct. The existing biliary drains should be eliminated over a guidewire previous to angiography to relieve the relative tamponade impact of the drain and to permit for higher visualization of the vasculature. Superselection of the right and left hepatic arteries, or of any vessels along the trail of the biliary drain, must be carried out if no lively bleeding or lesion is seen on celiac arteriography. Superior mesenteric arteriography is also beneficial to exclude accessory proper hepatic arterial sources of hemobilia. After the site of the bleeding is recognized, superselective catheterization with a microcatheter and microcoil embolization is performed. Pseudoaneurysms ought to be embolized across the neck of the aneurysm from distal to proximal to keep away from again bleeding from collateral arterial supply. Other embolic agents, such as glue (n-butyl cyanoacrylate) could be useful in choose cases, though they require larger operator experience. Placement of a lined stent across the site of vascular injury is an alternative option to embolization. This permits preservation of distal flow, which can be significantly useful in liver transplant sufferers. Percutaneous thrombin injection is an choice for cases of hemobilia secondary to hepatic artery pseudoaneurysm. There are numerous case reviews of percutaneous thrombin injection therapy of hepatic artery pseudoaneurysms, and it has been confirmed to be a protected and effective therapy. The risk of infection is elevated throughout cholangiography as a outcome of injected distinction can improve pressure inside the biliary tract, particularly in an obstructed system, and cause bacteremia. Prompt administration of a broad-spectrum antibiotic can forestall acute sepsis, but should it occur, the affected person should be managed immediately with vasopressors, inotropic brokers, and transfer to an intensive care setting. Percutaneous biliary drainage catheters must be left to bag drainage after intervention to allow clearance of contaminated blood or bile. Because of the adverse strain within the pleural space, percutaneous biliary drains that traverse the pleura may find yourself in bilothorax. This generally occurs when the drainage catheter aspect holes are positioned within the liver parenchyma or in the peritoneum. These sufferers typically require serial paracenteses or placement of a tunneled peritoneal drainage catheter. Evaluating the hepatic arterial anatomy is essential to the success of the process and to stop nontarget embolization. After being chosen, the vessels feeding the tumor are injected with both embolic materials and a chemotherapeutic agent. It is a minimally invasive, multiphasic process halting blood flow via embolization and providing radiation through the radioactive isotope Y-90. The remedy is particularly promising in sufferers with solitary tumors, with tumors regressing to the point of healing resection. Heat is usually most popular over cryoablation in the liver as a result of the elevated bleeding danger and the potential for a diffuse intravascular coagulation�like reaction with cryoablation. Patients with untreated unresectable cholangiocarcinoma have a median survival of 3. Traditional palliative approaches, similar to biliary decompression and intraductal stenting, are nonetheless widely used and discussed in prior sections. By interrupting the tumoral blood supply, chemoembolization induces ischemic tumoral necrosis by way of embolization after delivering focused high-dose intraarterial chemotherapy, sparing systemic publicity. Data counsel response charges and survival occasions enhance with intraarterial therapy within the setting of inoperable illness. Usefulness of 3D hybrid profile order method with 3T magnetic resonance cholangiography: comparability of image high quality and acquisition time. Hepatobiliary scintigraphy for the diagnosis of bile leaks produced after T-tube elimination in orthotopic liver transplantation. An efficient software in the administration of bile leak following laparoscopic cholecystectomy. Benign biliary strictures: diagnostic analysis and approaches to percutaneous remedy. Transhepatic balloon dilation of biliary strictures in liver transplant sufferers: a 10-year experience.
In their simplest and smallest form antimicrobial peptides work by discount tinidazole 300 mg on line, the vesicles are unilamellar bacteria h pylori symptoms purchase 500 mg tinidazole overnight delivery, but an aggregation might happen tetracycline antibiotics for acne treatment 500 mg tinidazole discount amex, resulting in multilamellar vesicles. Cholesterol solubility is determined by the relative focus of ldl cholesterol, bile salts, and phospholipids. In a solution composed of 10% solutes similar to bile, the realm underneath the curve represents the focus at which ldl cholesterol is maintained in answer. In the realm above the curve, bile is supersaturated with ldl cholesterol, and precipitation of ldl cholesterol crystals can occur. A mathematical mannequin of ldl cholesterol solubility has been developed and is influenced by the relative concentrations of lipid parts and the whole lipid composition. Gallstones form on account of the imbalance in concentration of solutes within the bile (bilirubin, bile salts, phospholipids, and cholesterol). After the bile is saturated, it precipitates into a more stable element: gallstones. Gallstones could be differentiated according to their composition into cholesterol and pigment stones. Cholesterol stones are usually a number of, of variable size, and irregular with color range from clear yellow to green and black. Pigment stones are dark as a outcome of the presence of calcium bilirubinate and solely 20% of ldl cholesterol. Black pigment stones are small and black, usually shaped as a consequence of hemolytic ailments such as hereditary spherocytosis and sickle cell illness. Cholesterol stones are more prevalent in Western international locations (>85%), principally as a outcome of obesity. Brown-pigmented stones are predominant in Asia primarily as a outcome of bacterial infections, biliary parasites, and stasis from partial biliary obstruction. The tetrahedral plot is used to record the relationships of the four main constituents of bile: water, bile salts, lecithin, and cholesterol. The triangular coordinates may be divided into 4 zones, representing the bodily state of the solutes in bile: crystals of cholesterol plus liquid (A); cholesterol crystals plus ldl cholesterol liquid crystals plus liquid (B); liquid crystals plus liquid (C); and the micellar zone during which cholesterol is in water resolution via the formation of cholesterol-lecithinbile salt micelles (D). Phospholipids are transferred extra efficiently than cholesterol, resulting in cholesterol enrichment of the remaining (remodeled) vesicles. Aggregation of these cholesterol-rich vesicles varieties multilamellar liquid crystals of cholesterol monohydrate. The remaining 15% to 20% is derived largely from the breakdown of hepatic hemoproteins. Although both could additionally be essential physiologically, the microsomal enzyme heme oxygenase, found in excessive focus all through the liver, spleen, and bone marrow, plays a major role within the initial conversion of heme to biliverdin. Bilirubin is sure avidly to plasma proteins, primarily albumin, earlier than uptake and additional processing by the liver. The liver is the sole organ capable of eradicating the albumin-bilirubin complicated from the circulation and esterifying the possibly poisonous bilirubin to water-soluble, unhazardous monoconjugated and deconjugated derivatives. After being extracted by the hepatocytes, bilirubin is conjugated with glucuronic acid to form bilirubin diglucuronide (conjugated bilirubin). The enzyme answerable for this response is glucoronil transferase present within the endoplasmic reticulum of the hepatocyte. Bilirubin is then transported throughout the hepatocyte by cytosolic binding proteins, delivering the molecule to the canalicular membrane for active secretion into bile. Conjugated bilirubin is then excreted into the duodenum in affiliation with combined lipid micelles. Once within the gut, bilirubin is transformed to urobilinogens by intestinal micro organism, which are then additional oxidized to pigmented urobilins. To serve this total perform, the gallbladder has absorptive, secretory, and motor capabilities. As a end result the gallbladder stores concentrated bile that reenters the distal bile duct and is secreted into the duodenum in response to a meal. The resultant mucin gel is believed to represent an important a half of the unstirred layer (diffusion-resistant barrier) that separates the gallbladder cell membrane from the luminal bile. However, considerable proof additionally means that mucin glycoproteins play a task as pronucleating agents for ldl cholesterol crystallization. Bile is normally concentrated fivefold by the absorption of water and electrolytes. The focus of calcium in gallbladder bile, which is a vital think about gallstone pathogenesis, is influenced by serum calcium, hepatic bile calcium, gallbladder water absorption, and the concentration of natural substances, corresponding to bile salts in gallbladder bile. The solubility within the micellar fraction is increased, but the stability of phospholipid-cholesterol vesicles is greatly decreased. Because cholesterol crystal precipitation occurs preferentially by vesicular somewhat than micellar mechanisms, the net effect of concentrating bile is an elevated tendency to nucleate cholesterol. However, the absorption of bilirubin, cholesterol, phospholipids, and bile salts is minimal compared with that of water. Thus these organic compounds are considerably concentrated by the normal absorptive process that happens within the gallbladder. The arrows indicate the route of water move across the cell membrane and into the intercellular areas. As water is transported into the space, the area distends, and an isotonic resolution enters the connective tissue area. Prostaglandins play an important function as stimulants of gallbladder mucin secretion. Furthermore, mucin glycoproteins are key pronucleating brokers for cholesterol crystallization. The acidification of bile happens by the transport of hydrogen ions by the gallbladder epithelium, through a sodium-exchange mechanism. Acidification of bile promotes calcium solubility, thereby preventing its precipitation as calcium salts. Compared with gallbladder bile, the bile secreted by the liver is barely alkaline, pH 7. When stimulated by consuming, the gallbladder empties 50% to 70% of its contents inside 30 to forty minutes. Many different hormonal and neural pathways are additionally necessary for the coordinated action of the gallbladder and sphincter of Oddi. Defects in gallbladder motility, which enhance the residence time of bile in the gallbladder, play a central position in the pathogenesis of gallstones. Endoscopic sphincterotomy: follow-up evaluation of results on the sphincter of Oddi. The sphincter regulates the circulate of bile and pancreatic juice into the duodenum and likewise prevents the regurgitation of duodenal contents into the biliary tract. These capabilities are achieved by preserving pressure inside the bile and pancreatic ducts greater than duodenal pressure. Thus sphincter pressure relaxes after a meal, allowing the passive move of bile into the duodenum. During fasting, high-pressure phasic contractions of the sphincter of Oddi persist by way of all phases of the migrating myoelectric advanced. Variations in origin and course of the hepatic artery and its branches: significance from a surgical viewpoint. Intestinal diffusion barrier: unstirred water layer or membrane floor mucous coat Recent progress in understanding ldl cholesterol crystal nucleation as a precursor to human gallstone formation. Interdigestive biliary output in man: relationship to fluctuations in plasma motilin and effect of atropine. This activity could additionally be a preventive mechanism against the accumulation of biliary crystals throughout fasting. The cholecysto�sphincter of Oddi reflex allows the human sphincter to relax as the gallbladder contracts. The gross anatomy and histology of the gallbladder, extrahepatic bile ducts, vaterian system, and minor papilla. The hepatic, cystic, and retroduodenal arteries and their relations to the biliary ducts with samples of the whole celiacal blood supply. The cystic artery and constituents of the hepatic pedicle: a examine of 500 specimens. Practical classification of the branching kinds of the biliary tree: an evaluation of 1094 consecutive direct cholangiograms.
If bleeding has not been recognized on endoscopy antibiotics for acne how long should i take it cheap tinidazole 1000 mg without prescription, a radiolabeled purple blood cell scan or angiography may be performed to higher delineate the placement of bleeding antibiotic resistant std 300 mg tinidazole discount. Surgical administration of pancreaticobiliary disease associated with juxtapapillary duodenal diverticula: case collection and evaluate of the literature antibiotic resistance fda cheap 1000 mg tinidazole with amex. Strictures and adhesions from prior diverticulitis, an inflammatory mass inflicting extrinsic compression of the bowel, volvulus of a phase with giant diverticula, and pseudoobstruction because of perform dysmotility can all lead to signs of stomach distention, nausea, and vomiting. If surgical intervention is indicated because of an entire obstruction, the enterolith could additionally be milked into the distal bowel and removed through an enterotomy in a healthy segment of bowel. Alternatively, it could be resected along with the diverticular disease, especially in the setting of related irritation. An upper gastrointestinal collection with small bowel follow-through and enteroclysis may be each diagnostic and therapeutic. The prognosis can be made on delayed images where contrast is retained within a diverticulum even after the enteric distinction has moved by way of the small bowel lumen. We are taught to think of a Meckel diverticulum when it comes to the Rule of 2s: located 2 toes (60 cm) from the terminal ileum, 2 inches in length, affecting 2% of the overall population, occurring twice as often in males, containing one or two types of heterotopic mucosa (most generally gastric or pancreatic), and presenting in the first 2 decades of life, most commonly in the first 2 years of life. However, sufferers who experience problems associated to small bowel diverticular disease ought to undergo segmental resection with primary anastomosis. Nonoperative administration may be pursued in additional chronic cases that current with imprecise stomach ache, bloating, or signs of bacterial overgrowth and malnutrition. A conservative approach is also indicated for sufferers with in depth illness the place surgical resection would end in short gut syndrome. Select instances of uncomplicated diverticulitis are efficiently managed with antibiotics as well, but acceptable affected person choice stays paramount. If there are any signs of hemodynamic instability, sepsis, or peritonitis, surgical resection is really helpful. In the third week of gestation, the vitelline duct, additionally known as the omphalomesenteric duct, is broadly patent permitting the yolk sac to communicate with the gut. Between the fifth and ninth week of gestation, the duct will obliterate and the placenta replaces the yolk sac as the source of fetal vitamin. This is why a Meckel diverticulum is a true diverticulum-and the one true diverticulum-of the small gut that contains all layers of the small bowel. Interestingly, failure of the vitelline duct to obliterate can result in different anomalies, although these are much less common than a Meckel diverticulum. Such anomalies embrace an ileal umbilical fistula, which happens if the entire duct stays patent; a vitelline duct cyst, which ends up from the failure of the umbilical aspect of the duct to obliterate; and a fibrous wire connecting the ileum to the umbilicus. A Meckel diverticulum is by far the most common, representing 90% of vitelline duct anomalies. Although pancreatic tissue is the most typical sort of heterotopic tissue, gastric tissue is the most typical sort in a symptomatic Meckel diverticulum, as later discussed. A Meckel diverticulum is normally positioned within one hundred cm of the ileocecal valve, though the mean distance varies with age: the older the affected person, the farther away the Meckel diverticulum is from the ileocecal valve. In youngsters less than 2 years of age, the mean distance is 34 cm, compared to 46 cm in children aged 3 to 21 years old and 67 cm in folks older than 21 years. Patients also can current with gastrointestinal bleeding, although that is more widespread in children. Bleeding can current as bright purple rectal bleeding or painless, sluggish, intermittent melena. In adults, the most common kind of complication is intestinal obstruction, accounting for approximately onethird of issues (Table 77. Mechanisms of obstruction embody enlargement of the small bowel around a fibrous band attached to the umbilicus, entrapment of an intestinal loop within a mesodiverticular band, intussusception with a free diverticulum appearing as a lead level, volvulus round an umbilical band, and stenosis secondary to chronic diverticulitis. Diverticulitis occurs in roughly 20% of patients with a symptomatic Meckel diverticulum and is arguably indistinguishable from acute appendicitis in each presentation and potential complications, including necrosis and perforation. The ectopic gastric mucosa can produce gastric acid and pepsin, which might cause ileal ulceration and subsequent bleeding. This is rare in sufferers older than 30 years of age because after this age, the gastric mucosa often atrophies. Several threat components are associated with increased complication charges including age, gender, and anatomic variants of Meckel diverticula. The risk of complications is inversely related to age, with a 4% to 5% danger at 2 years of age and 1% at forty years. Symptomatic Meckel diverticula are more common in males than ladies with a male-to-female ratio starting from 2: 1 to 5: 1. Anatomically, longer, narrow-based diverticula usually have a tendency to cause obstruction or irritation as compared to short, large-based diverticula, that are more vulnerable to entrapment. A Meckel diverticulum ought to be considered in patients with proper decrease quadrant ache or indicators of acute appendicitis and intraoperatively are discovered to have a normal-appearing appendix. If gastrointestinal bleeding is present, a 99m Tcpertechnetate scintigraphy (also referred to as a Meckel scan) could additionally be obtained. On imaging, a Meckel diverticulum is recognized as a focus of activity in the lower abdomen or upper pelvis that usually appears on the time the stomach is visualized and increases because the abdomen activity increases. Operative intervention is arguably the gold commonplace in making the diagnosis in comparison with an costly, and at instances, low-yield radiographic workup. A main anastomosis is then performed and the small bowel mesenteric rent is closed. In the asymptomatic patient, indications for surgical intervention have been the topic of many research, however regardless of these studies, the topic stays controversial. Part of the controversy is that older, retrospective evaluations cite excessive charges of morbidity and mortality following diverticular resection. Historically, studies from the Nineteen Fifties reported a mortality rate of 20% from a diverticulectomy. Since the Eighties, research have repeatedly reported a near-zero mortality fee, altering the dogma on surgical management. The present recommendation is that until there are strong contraindications, an by the way found Meckel diverticulum must be removed. The rules of resection are related for symptomatic and asymptomatic Meckel diverticula: the diverticulum and any related bands should be removed with an ileal resection or a easy diverticulectomy. The decision of which treatment choice to pursue lies in whether or not the affected person presents with bleeding. A two-layer closure is usually used with an inner operating layer of absorbable suture adopted by an outer layer of silk Lembert sutures. Additionally, a number of studies in children with symptomatic Meckel diverticula show that a laparoscopic approach is secure, possible, and may improve outcomes. Bleeding from a duodenal or jejunoileal diverticulum results from blood vessels related to the vasa recta. Bleeding from a Meckel diverticulum is a results of ulceration from the acid secretion from heterotopic gastric mucosa. A duodenal diverticulum can current a singular surgical problem given its shut proximity to the ampulla of Vater. Jejunoileal diverticula are the least widespread kind of small bowel diverticula, but are most probably to produce symptoms. It is for these reasons that the overall surgeon ought to be well versed in the analysis and administration of small bowel diverticula. Acquired jejunoileal diverticulosis and its problems: a review of the literature. Complicated small-bowel diverticulosis: a case report and evaluate of the literature. Diagnosis and administration of jejunoileal diverticular hemorrhage: a decade of experience. Thompson The first record of radiation enteritis was described in 1897 and concerned transient symptoms of pain and diarrhea that correlated with radiation exposure. The scope of this chapter will include radiation harm to the small intestine and colon. High-energy photons create ionizing electrons that then directly break chemical bonds.






