Nicotinell
Nicotinell
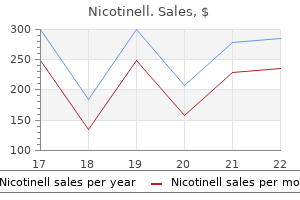
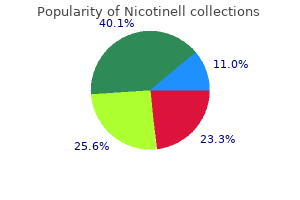
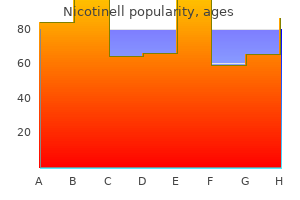
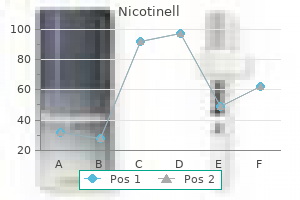
Nicotinell dosages: 52.5 mg, 35 mg, 17.5 mg
Nicotinell packs: 1 packs, 2 packs, 3 packs, 4 packs, 5 packs, 6 packs, 7 packs, 8 packs, 9 packs, 10 packs

Increasing attention is being given to the ability of molecular testing to detect a number of pathogens from a single specimen primarily based on clinical syndromes quit smoking patches nicotinell 17.5 mg purchase line, like respiratory or gastrointestinal diseases quit smoking symptom timeline generic nicotinell 35 mg with visa. In an evaluation of multiplex testing of gastrointestinal pathogens at our establishment quit smoking sore throat 35 mg nicotinell order fast delivery, we decided that sufferers with attainable infectious diarrhea had a mean of three bacterial, viral, or parasitic tests performed, with only an 8. Using a single multiplex molecular assay for 15 or 23 targets, relying on the assay used, the positivity rate elevated to > 30%. Rapidly cleared episodes of herpes simplex virus reactivation in immunocompetent adults. Evaluation of Chikungunya diagnostic assays: variations in sensitivity of serology assays in two independent outbreaks. Von M�ller L, Hampl W, Hinz J, Meisel H, Reip A, Engelmann E, Heilbronn R, G�rtner B, Kr�mer O, Einsele H, Hebart H, Ljubicic T, L�ffler J, Mertens T. International requirements and reference supplies for quantitative molecular infectious illness testing. Kimura H, Futamura M, Kito H, Ando T, Goto M, Kuzushima K, Shibata M, Morishima T. This type of "syndromic" testing from a single specimen collection allows clinicians to display screen for a panel of pathogens that present with overlapping medical symptoms (97). The convenience and advantage of testing multiple pathogens from a single specimen is becoming well-liked with clinicians, and, as a result, some laboratories are striving to provide broad testing panels from single-specimen assortment units, such as a single swab for analysis of gynecologic pathogens. Similarly, growing use of know-how like microfluidics, in addition to the miniaturization of diagnostic testing, is being investigated for identification of a number of analytes from just some drops of blood. These new strategies and units can potentially decrease incorrect specimen assortment, cut back the number of invasively collected specimens, and dramatically scale back the quantity of fabric that should be collected from a affected person. The threat of overtesting from single samples is misinterpretation of the scientific importance of a end result, which may lead to overtreatment and affected person hurt. Further developments and breakthroughs in know-how will improve our ability to characterize viral infections. Influenza virus nucleic acid is also extremely dynamic, and next-generation sequencing of the neuraminidase gene is getting used to monitor oseltamivir resistance (99, 100). The kind of testing platforms utilized in clinical laboratories for viral detection has evolved quickly and can proceed to achieve this as newer know-how emerges. The technological modifications that improve our capacity to detect multiple analytes from a single specimen have, and can, have an result on the specimen type, assortment gadgets, and quantity necessities which are needed for virus testing. A longitudinal molecular surveillance research of human polyomavirus viremia in heart, kidney, liver, and pancreas transplant sufferers. Guideline for the prevention and management of norovirus gastroenteritis outbreaks in healthcare settings. Histological patterns of polyomavirus nephropathy: correlation with graft consequence and viral load. Clinical utility of business enzyme immunoassays during the inaugural season of West Nile virus exercise, Alberta, Canada. Prospective identification of congenital cytomegalovirus an infection in newborns utilizing real-time polymerase chain reaction assays in dried blood spots. Detection of adenoviruses in stools from healthy individuals and patients with diarrhea by two-step polymerase chain response. Routine detection of herpes simplex virus and varicella zoster virus by polymerase chain reaction reveals that preliminary herpes zoster is regularly misdiagnosed as herpes simplex. An update on remedy of genotype 1 continual hepatitis C virus an infection: 2011 practice guideline by the American Association for the Study of Liver Diseases. Longitudinal observation of enterovirus and adenovirus in stool samples from Norwegian infants with the highest genetic threat of sort 1 diabetes. Diagnosis of enteroviral meningitis by use of polymerase chain reaction of cerebrospinal fluid, stool, and serum specimens. Comparative research of nasopharyngeal aspirate and nasal swab specimens for analysis of acute viral respiratory an infection. Clinical Laboratories Can Safely Manage Specimens from Persons Under Investigation for Ebola Virus Disease, on Department of Health and Human Services. Multiplex detection of gastrointestinal pathogens: a comparative evaluation of two business panels using clinical stool specimens. Mohamed S, Penaranda G, Gonzalez D, Camus C, Khiri H, Boulm� R, Sayada C, Philibert P, Olive D, Halfon P. Detection of resistance mutations to antivirals oseltamivir and zanamivir in avian influenza A viruses isolated from wild birds. Culture has lengthy been thought-about the "gold standard" for viral prognosis as a outcome of it secures an isolate for additional evaluation, is extra "open-minded" than strategies that target single brokers, and permits the unexpected and even novel agent to be recovered. In apply, use of specialised cell tradition methods, embryonated eggs, and laboratory animals is confined to research or main public well being reference laboratories, with cell cultures in monolayers the only real isolation system utilized in routine diagnostic laboratories. The previous two decades have seen standard cell culture strategies supplemented and even replaced by extra speedy and targeted cell tradition strategies. Rapid tradition methods can be performed by less skilled personnel, with much less labor, and with results reported within 1 to 5 days of inoculation. Isolating viruses in cell cultures in numerous configurations has been the principle diagnostic strategy in most medical virology laboratories, but this strategy is being used much less regularly now that viral antigen detection assays and molecular strategies have been improved in analytical sensitivity and specificity and simplified to enable their efficiency in routine laboratories. At this writing isolation in cell tradition is most frequently included into viral diagnostic algorithms to confirm optimum performance of other strategies, to validate newer strategies, or to aid the invention of latest viruses, quite than as the first diagnostic methodology. This change in the function of virus isolation in cell cultures is reflected within the lack of recent publications in progressive cell culture strategies for clinical diagnosis. Regardless of the breadth of utility throughout smaller scientific laboratories, virus isolation in tradition will proceed to be utilized in larger specialised virology and public well being laboratories and by those thinking about virus discovery. Thus this chapter will present particulars of present cell culture isolation methods used for viral prognosis and describe numerous medical purposes of virus isolation in cell tradition. Cell cultures are typically separated into three varieties (Table 1): main cells, that are prepared directly from animal or human tissues and can usually be subcultured for only one or two passages; diploid cell cultures, that are usually derived from human tissues, either fetal or new child, and can be subcultured 20 to 50 times before senescence; and continuous cell strains, which may be established from human or animal tissues, from tumors, or following the spontaneous transformation of regular tissues. These have a heteroploid karyotype and could be subcultured an indefinite number of times. However, sensitivity to virus an infection may change after serial passage and after passage in different laboratories. Variation in Sensitivity to Different Viruses Cell cultures vary greatly in their sensitivity to totally different viruses (Table 2). When small quantities of virus are present in a clinical pattern, a positive end result may be obtained only when probably the most sensitive methods are used. Laboratories should periodically monitor the sensitivity traits of cell cultures, since significant adjustments can happen over time or even from season to season for rapidly changing viruses such as influenza (2�4). Supplies and Equipment Needed the materials needed for the isolation of viruses in cell culture are given in Table three. Maintaining totally different cell cultures in healthy situation is totally essential to ensure good outcomes. A broad number of cell cultures are available commercially and may be bought and delivered a few times a week based on the needs of the laboratory. The cell type(s) most sensitive to the suspected viruses in the clinical specimen ought to be included. Ideally, only actively dividing cultures should be used because aged cells are much less sensitive to virus infection. All cell cultures should be examined underneath the microscope before inoculation to be sure that the cells are in good condition. Inoculation and Incubation Although strategies might differ considerably for various viruses, normally, the following procedures apply for noncentrifuged typical cultures: 1. Allow specimen to adsorb (in a horizontal place in a stationary rack) in the incubator at 35�C to 37�C for 30 to 60 minutes. Compare the appearance of the inoculated tubes with uninoculated management tubes from the same lot of cell cultures. Culture medium containing a phenol pink indicator should appear light orange or peach coloured. Some continuous cell lines have been genetically engineered to present a reporter system for fast and simplified detection, or for higher sensitivity. The use of cryopreserved cell cultures, that could be saved at - 70�C and thawed to be used as wanted, can provide extra flexibility (5, 6). Obtaining and Processing Specimens It is necessary to reiterate that without appropriate specimens which are properly collected early in sickness and promptly transported to the laboratory, the following effort and time spent in isolation makes an attempt will be wasted. Accomplishing this is an important task of the scientific virology laboratory and requires continuing communication with and training of the suppliers.
Monitoring In placenta previa quit smoking k2 nicotinell 17.5 mg purchase on-line, the gap between the placental edge and cervical os is monitored during being pregnant as a result of the placental location can change with advancing pregnancy quit smoking medication generic nicotinell 35 mg overnight delivery. Women with any diploma of Vaginal Bleeding Late in Pregnancy placental overlap ought to be delivered by cesarean section quit smoking results timeline nicotinell 52.5 mg generic without prescription. When the placental edge is larger than 0 mm however lower than 20 mm from the internal cervical os, vaginal delivery may nonetheless be attainable, though the likelihood of cesarean part is way higher. When vasa previa is recognized, serial ultrasound is indicated as a end result of irregular vessels regress in up to 15% of women. When undiagnosed prior to labor, vasa previa carries a fetal mortality rate of 55% to 95%. Antenatal analysis with deliberate cesarean section decreases fetal mortality to 3% and reduces the necessity for transfusion from 60% to 3%. Because the hemorrhage is fetal blood, maternal threat from vasa previa is complications related to cesarean part. Complications Maternal risks associated with placenta previa include want for cesarean part, postpartum hemorrhage, and blood transfusion. Perinatal problems embody prematurity, intrauterine progress restriction, anemia, coagulopathy, and dying. Maternal risks include surgical risk associated with cesarean section, hypovolemic shock and hemorrhage, and hysterectomy. Leukemia was as soon as a uniformly deadly diagnosis, with less than a 5% to 10% cure fee until the mid to late Nineteen Sixties. Further successive, incremental enhancements in end result have been achieved due to scientific trials conducted by massive single facilities and national and worldwide cooperative groups which have efficiently enrolled a excessive percentage of eligible kids. Classification the first degree of classification of leukemia is acute versus chronic. Acute leukemia is characterized by the predominance of very immature white blood cell precursors, or blasts, and is an aggressive, rapidly deadly disease if left untreated. Chronic leukemia is characterised by proliferation of relatively mature white blood cells and is often an indolent disease. The second level of classification is lymphoid versus myeloid, relying on whether the leukemic cells display characteristics of lymphocyte precursors or myelocyte (granulocyte, erythrocyte, monocyte, or megakaryocyte) precursors. Predispositions the answer to the primary question is unknown within the vast majority of instances. Attempts to correlate varied genetic features or environmental or infectious exposures with danger of childhood leukemia have been largely uninformative. Although a quantity of constitutional and single-gene issues are identified to confer an elevated danger of childhood leukemia (Table 2), in whole, these are concerned in only a really small minority of instances. The peak age at onset of leukemia for children with Down syndrome is sooner than for different kids. Children with Down syndrome are inclined to present with biologically favorable subtypes of leukemia, but they also undergo increased toxicity from remedy. Leukemia accounts for roughly 30% of childhood cancers, making it the most common type of childhood most cancers. Box 1 Classification of Childhood Acute Myeloid Leukemia (World Health Organization Criteria) components for childhood leukemia, including electromagnetic fields from power traces. Cellular Pathogenesis Three major characteristics of leukemia cells distinguish them from normal hematopoietic cells. This results in a progress advantage for leukemia cells, leading to progressive alternative of the conventional bone marrow with an enormous clonal population of poorly differentiated leukemic blasts. Another characteristic of leukemia cells is their tendency to unfold all through the physique and infiltrate organs other than the bone marrow. Molecular Pathogenesis As is true of most human cancers, growth of leukemia is a multihit process. The initiating occasions are sometimes chromosomal rearrangements that activate expression of cellular proto-oncogenes by fusing them to transcriptionally active immunoglobulin or T-cell receptor genes or by joining two genes from completely different chromosomes to create a new fusion gene that encodes a chimeric protein with unique practical properties. The most common of these sentinel chromosomal rearrangements are translocations (exchanges of genetic material between chromosomes), which can serve as a singular marker of the malignant clone. The solely environmental exposures that are known to predispose to leukemia are ionizing radiation (such as was seen with atomic bomb survivors) and prior exposure to certain chemotherapy medicine (cyclophosphamide [Cytoxan], etoposide [Vepesid]). There is good proof that in utero publicity to maternal diagnostic radiation additionally increases the chance of childhood most cancers (including leukemia), significantly if the exposure is within the first trimester. Examples of particular genetic hits identified to be associated with the development of childhood leukemia are summarized in Table 3. Clinical Presentation Most signs and indicators of childhood leukemia are the outcome of the propensity of leukemia cells to replace the bone marrow and infiltrate multiple other organs throughout the body. The alternative of regular bone marrow is responsible for the characteristic abnormal blood counts, which typically embrace the triad of neutropenia, anemia, and thrombocytopenia. Depending on the variety of circulating leukemic blasts in the peripheral blood, the entire white blood cell rely could also be low, normal, or excessive. The neutropenia is commonly profound (absolute neutrophil rely <500/L), and is related to an elevated danger of serious infection. Blood cultures and broad-spectrum intravenous antibiotic protection are indicated in any patient with newly recognized leukemia and fever. Anemia is often manifested by fatigue, lethargy, headache, pallor, and, in extreme circumstances, congestive heart failure that could be precipitated by vigorous transfusion or intravenous hydration. Thrombocytopenia often results in bruising and petechiae; nevertheless, clinically significant hemorrhage is uncommon in industrialized nations. Platelet transfusion is indicated for bleeding or for very low platelet counts (<10,000� 20,000/L). Infiltration of organs other than the bone marrow with leukemia cells is liable for additional presenting scientific features. Box 2 summarizes the organ techniques most often involved in leukemia and the standard medical manifestations. Medical Emergencies in Childhood Leukemia Newly diagnosed leukemia in a child is a medical emergency. There are a quantity of potentially life-threatening complications which might be current at prognosis or can develop inside a brief while after analysis. Renal insufficiency can develop because of the nephrotoxic results of precipitated urate crystals in the renal tubules; in severe circumstances, dialysis could also be necessary. Management consists of aggressive hydration to reduce tubular uric acid concentration and alkalinization of urine to promote solubility of urate crystals. The xanthine oxidase inhibitor allopurinol (Zyloprim) is routinely used during the first 3 to 7 days of leukemia remedy to decrease uric acid production. Frequent electrolyte monitoring with normal management of irregular levels is essential. Management consists of treating the leukemia as soon as potential and performing exchange transfusion or leukopheresis in instances where symptoms are prominent. This association results from the discharge of thromboplastin from the cytoplasmic granules in promyelocytic blasts. Despite these measures, as a lot as 10% of patients die of bleeding issues in the course of the preliminary weeks of remedy, and extra sufferers endure lasting morbidity from retinal hemorrhages and nonfatal central nervous system hemorrhages. Patients can current with respiratory distress, cough, orthopnea, complications, syncope, dizziness, facial swelling, or plethora. This evaluation must precede any makes an attempt at sedation for diagnostic procedures, because even light sedation can precipitate acute airway collapse. Diagnostic materials ought to be obtained by the least invasive methodology potential earlier than treatment. If essential, emergent airway compromise could be treated with radiation or steroids, or both. Differential Diagnosis Although leukemia should be thought-about in cases of isolated neutropenia, anemia, or thrombocytopenia, the vast majority of leukemia patients current with depressions in more than one cell line. Pancytopenia on the premise of bone marrow failure (from acquired aplastic anemia or uncommon inherited bone marrow failure syndromes) can be distinguished from leukemia by bone marrow biopsy for assessment of total marrow cellularity. Risk Stratification In the final several years, treatment choices for kids with newly identified acute leukemia have been primarily based on the idea of risk stratification. Using elements recognized during medical trials to predict a excessive or low danger of relapse, sufferers are separated into risk groups before the start of therapy or on the end of the primary month of induction therapy. Different centers and cooperative groups usually make use of different risk-stratification methods. Early response has historically been measured by the response to a prednisone prophase that includes a single dose of intrathecal methotrexate and seven days of prednisone, or by the proportion of blast cells remaining in the bone marrow after 7 to 14 days of multiagent remedy.
Superficial infections in kids with mild to reasonable neutropenia could also be treated with acceptable oral antibiotics quit smoking medication nicotinell 17.5 mg generic line. Doses starting from 2 to 50 g/kg per day lead to quit smoking hypnosis seminars in my area nicotinell 52.5 mg buy with mastercard dramatic increases in neutrophil counts quit smoking 6 weeks pregnant nicotinell 35 mg cheap mastercard, resulting in marked attenuation of infection and irritation. Autoimmune neutropenia may be aware of intermittent corticosteroids, particularly if it is part of an underlying disease course of such as systemic lupus erythematosus. Hematopoietic stem cell transplantation is indicated in sufferers who develop myelodysplasia or acute myelogenous leukemia as seen in problems such as severe congenital neutropenia or Shwachman�Diamond syndrome. Hematopoietic stem cell transplantation is also useful for aplastic anemia or hemophagocytic lymphohistiocytosis complicating syndromes talked about earlier. The natural historical past and prognosis of those range greatly from indolent and slow-growing types (over many years) to highly aggressive (within weeks) types. Expert hematopathology evaluate incorporating morphologic, immunophenotypic, and genetic features is crucial for an accurate analysis. The illness is very aware of treatment with a wide selection of remedy options (remission rates exceeding 90% with combined rituximab/chemotherapy), though the scientific course is characterized by repetitive relapses. The highest relative threat of growing a secondary malignancy occurs greater than 21 to 30 years after original prognosis. The time period malignant lymphoma was originally launched by Billroth in 1871 to describe neoplasms of lymphoid tissue. Leukocyte problems: Quantitative and qualitative disorders of the neutrophil, Part 1. Extended spectrum of human glucose-6phosphatase catalytic subunit three deficiency: Novel genotypes and phenotypic variability in extreme congenital neutropenia. Primary autoimmune neutropenia in children: A study of neutrophil antibodies and clinical course. Genotype/phenotype correlation in glycogen storage disease type 1b: A mutlicentre examine and evaluation of the literature. However, additional elements are likely answerable for this sudden improve in incidence. Etiology and Risk Factors Chromosomal Translocations and Molecular Rearrangements Nonrandom chromosomal and molecular rearrangements play an necessary position in the pathogenesis of many lymphomas and infrequently correlate with histology and immunophenotype. The modeled rates are the purpose estimates for the regression strains calculated by the Joinpoint Regression Program (Version four. Low-Grade or Indolent Lymphomas Painless, slowly progressive peripheral adenopathy is the commonest scientific presentation in sufferers with low-grade lymphomas. Patients generally report a history of waxing and waning adenopathy earlier than in search of medical consideration. Spontaneous regression of enlarged lymph nodes can occur, which may cause a lowgrade lymphoma to be confused with an infectious condition. Infection with Borrelia burgdorferi has been detected in about 35% of patients with major cutaneous B-cell lymphoma in Scotland. Studies point out that Campylobacter jejuni and immunoproliferative small intestinal illness are associated. European reviews have noted an affiliation between infection with Chlamydia psittaci and ocular adnexal lymphoma. Attempts to affirm this affiliation in the Western hemisphere have been unsuccessful. High-Grade or Aggressive Lymphomas the scientific presentation of high-grade lymphomas is extra diversified. Lymphoblastic lymphoma typically manifests with an anterior superior mediastinal mass, superior vena cava syndrome, and leptomeningeal illness. Diagnosis A definitive diagnosis could be made solely by biopsy of pathologic lymph nodes or tumor tissue. It is important typically to carry out an excisional lymph node resection to keep away from false-negative results and inaccurate histologic classification; fine-needle aspirations or core biopsies are often insufficient for diagnostic functions. In addition to morphologic evaluate and immunostaining of tissue, other studies similar to detailed cellular immunophenotyping and genotyping for related oncogenes are sometimes wanted to full the analysis. An aberrant clonal intraepithelial T-cell inhabitants could be present in up to 75% of sufferers with refractory celiac sprue before overt T-cell lymphoma develops. Additionally, systemic lupus erythematosus and rheumatoid arthritis have been associated with a barely increased threat of B-cell lymphoma. Another way to group the many totally different lymphoma histologies is by medical presentation and prognosis (Table 1). In the pre-rituximab era, individuals with no danger factors or one danger factor had a predicted 5-year overall survival of 73%, compared with 26% for high-risk patients with 4 or 5 threat components. In addition to a detailed historical past and physical examination, baseline staging research are warranted. Upper gastrointestinal endoscopy or gastrointestinal series with small bowel follow-through is recommended in patients with head and neck involvement (tonsil, base of tongue, nasopharynx) and people with primary gastrointestinal disease. Mantle cell lymphoma is associated with a high incidence of occult gastrointestinal involvement. However, in some cases, radiation therapy or, hardly ever, surgical resection performs a task. Biological approaches, together with monoclonal antibodies and antibody-drug conjugates have shown vital activity and are now incorporated into most therapy paradigms. Autologous and allogeneic stem-cell transplantation are principally reserved for sufferers with recurrent or refractory illness. The disease is conscious of treatment (remission charges above 90% with combined rituximab/chemotherapy), although the scientific course is characterised by repetitive relapses. Radiotherapy is a valid therapy choice for these sufferers (especially stage I), and related 15- to 20-year disease-free survival charges are higher than 50%. Treatment choices for relapsed indolent lymphoma include repeating rituximab without or and not using a totally different chemotherapy regimen, radioimmunotherapy, or stem-cell transplantation. Autologous stem-cell transplantation is an possibility for patients with relapsed illness, though an improvement in overall survival is debated. Allogeneic stem cell transplantation is a potential curative modality for sufferers with relapsed or refractory disease, though patient choice is critical owing to potential morbidity and mortality related to this therapeutic choice. The variety of treatment cycles is determined by stage of disease and response to therapy. Prompt initiation of remedy, together with aggressive supportive care measures, is commonly warranted. Recent evidence with use of initial rituximab-based therapy suggests significantly improved outcomes in the fashionable era. Mycosis fungoides and Sezary syndrome are cutaneous T-cell � lymphomas that originally might present eczematous lesions. It is commonly tough to establish prognosis, but eventually the lesions become plaques and tumors. Sezary syndrome is a variant of � mycosis fungoides and exhibits peripheral blood involvement; patients usually have diffuse erythroderma. Measures to stop this complication include aggressive hydration, allopurinol (Zyloprim), alkalinization of the urine, and frequent monitoring of electrolytes, uric acid, and creatinine. Rasburicase (Elitek), a recombinant urate oxidase enzyme, is an costly but potent agent for treating hyperuricemia. Some groups induction therapy with aggressive high-dose cytarabine1 (Cytosar-U)based chemotherapy adopted by consolidative autologous stemcell transplantation in first remission. As famous later, there has been 1 Novel Treatment Options and Modalities Many new agents focusing on specific molecular targets such as the ubiquitin-proteasome pathway can be found for the therapy of lymphoma. Early detection of recurrent illness is essential in part as a result of these patients could also be candidates for potentially healing therapy. Long-term risk of heart problems after remedy for aggressive non-Hodgkin lymphoma. Thus, the chance of certain radiation-induced issues has been decreased in sufferers treated more lately. All chemotherapy brokers might cause long-term morbidity; in particular, patients who acquired an anthracycline.
Ocular decontamination entails irrigation with copious amounts of tepid water or zero quit smoking medication nicotinell 35 mg order overnight delivery. Gastrointestinal decontamination quit smoking 28 days order nicotinell 52.5 mg with amex, if the ingestion was recent quit smoking 4th week nicotinell 17.5 mg cheap mastercard, involves the administration of activated charcoal. If the patient is symptomatic (bradycardia or bronchorrhea), a take a look at dose ought to be administered, zero. If no indicators of atropinization are current (tachycardia, drying of secretions, and mydriasis), atropine ought to be administered instantly, 0. Beneficial results are seen within 1 to 4 minutes and maximum impact in eight minutes. The common dose in the first 24 hours is forty mg, however one thousand mg or more has been required in severe instances. The most dose ought to be maintained for 12 to 24 hours, then tapered and the patient observed for relapse. Successful therapy with pralidoxime chloride may enable a reduction within the dose of atropine. The deadly dose of malathion is bigger than 1375 mg/kg and that of chlorpyrifos is 25 g; the latter compound is unlikely to cause death. The onset of acute ingestion toxicity occurs as early as three hours, usually earlier than 12 hours and at all times earlier than 24 hours. The metabolites are eradicated within the urine and the presence of p-nitrophenol within the urine is a clue up to 48 hours after publicity. Diaphoresis, extreme salivation, miosis, and muscle twitching are helpful clues to prognosis. Early, a cholinergic (muscarinic) disaster develops that consists of parasympathetic nervous system exercise. It should be given early before "aging" of phosphate bond produces tighter binding. However, current reports indicate that pralidoxime chloride is beneficial even a quantity of days after the poisoning. Cardiac and blood strain monitoring are advised during and for a number of hours after the infusion. Contraindicated drugs embody morphine, aminophylline, barbiturates, opioids, phenothiazine, reserpine-like drugs, parasympathomimetics, and succinylcholine. Seizures may respond to atropine and pralidoxime chloride however usually require anticonvulsants. Cardiac dysrhythmias may require electrical cardioversion or antidysrhythmic remedy if the affected person is hemodynamically unstable. The route of elimination is by gastric secretion, liver metabolism, and 10% urinary excretion of conjugates and free phencyclidine. Manifestations the traditional picture is bursts of horizontal, vertical, and rotary nystagmus, which is a clue to diagnosis (occurs in 50% of cases), miosis, hypertension, and fluctuating altered psychological state. Mild intoxication with 1 to 6 mg produces drunken and weird habits, agitation, rotary nystagmus, and blank stare. Violent conduct and sensory anesthesia make these sufferers insensitive to pain, self-destructive, and dangerous. Most are communicative within 1 to 2 hours, are alert and oriented in 6 to eight hours, and recover completely in 24 to 48 hours. Moderate intoxication with 6 to 10 mg produces extra salivation, hypertension, hyperthermia, muscle rigidity, myoclonus, and catatonia. Recovery of consciousness occurs in 24 to 48 hours and full restoration in 1 week. Severe intoxication with 10 to 25 mg ends in opisthotonus, decerebrate rigidity, convulsions, extended fluctuating coma, and respiratory failure. Recovery of consciousness happens in 24 to 48 hours, with complete normality in a month. Medical issues include apnea, aspiration pneumonia, cardiac arrest, hypertensive encephalopathy, hyperthermia, intracerebral hemorrhage, psychosis, rhabdomyolysis and myoglobinuria, and seizures. Fatalities happen with ingestions of higher than 100 mg and with serum ranges larger than 100 to 250 ng/mL. In instances of intentional poisoning, the patients require psychiatric clearance for discharge. Observation of milder circumstances of carbamate poisoning, even those requiring atropine, for six to 8 hours symptom-free could also be sufficient to exclude important toxicity. Phencyclidine (Angel Dust) Phencyclidine is an arylcyclohexylamine associated to ketamine and chemically related to the phenothiazines. It is inexpensively manufactured by "kitchen chemists" and is mislabeled as different hallucinogens. Improper phencyclidine synthesis could release cyanide when heated or smoked and may trigger explosions. Measurement of phencyclidine in the gastric juice is recognized as for as a result of concentrations are 10 to 50 times higher than in blood or urine. Phencyclidine may be detected within the urine of the common person for 10 days to three weeks after the last dose. The analogs of phencyclidine may not produce constructive check outcomes for phencyclidine in the urine. Cross-reactions with bleach and dextromethorphan may trigger false-positive urine take a look at outcomes on immunoassay, and crossreaction with doxylamine may produce a false-positive finding on fuel chromatography. Toxic Dose the usual dose of phencyclidine blended with marijuana joints is a hundred to 400 mg of phencyclidine. Management the patient should be noticed for violent, self-destructive, weird behavior and paranoid schizophrenia. Patients ought to be positioned in a low sensory setting and harmful objects must be faraway from the world. In circumstances of extreme toxicity (stupor or coma), continuous gastric suction may be tried (with protection of the airway) because the drug is secreted into the gastric juice. Physical restraints could also be necessary, but they should be used Kinetics Phencyclidine is a lipophilic weak base, with a pKa of 8. It is rapidly absorbed when smoked and snorted, poorly absorbed from the acid abdomen, and rapidly absorbed from the alkaline middle small gut. The onset of action when smoked is 2 to 5 minutes, with a peak in 15 to half-hour. Its duration of action at low doses is four to sparingly and for the shortest time potential because they improve threat of rhabdomyolysis. Pharmacologic intervention consists of diazepam (Valium) 10 to 30 mg orally or 2 to 5 mg intravenously initially and titrated upward to 10 mg; however, as much as 30 mg could additionally be required. Phenothiazines and butyrophenones should be prevented in the acute phase as a result of they decrease the convulsive threshold; nonetheless, they may be wanted later for psychosis. In the case of emergent hypertensive disaster (blood strain >200/115 mm Hg) nitroprusside can be utilized in a dose of 0. Rhabdomyolysis and myoglobinuria are treated by correcting quantity depletion and insuring a urinary output of larger than 2 mL/kg/h. Phenothiazines and Nonphenothiazines (Neuroleptics) Toxic Mechanism Neuroleptics have complex mechanisms of toxicity, including (a) block of the postsynaptic dopamine receptors; (b) block of peripheral and central -adrenergic receptors; (c) block of cholinergic muscarinic receptors; (d) quinidine-like antidysrhythmic and myocardial depressant effect in circumstances of huge overdose; (e) reducing of the convulsive threshold; (f) effect on hypothalamic temperature regulation (Table 25). Toxic Dose Extrapyramidal reactions, anticholinergic effects, and orthostatic hypotension could occur at therapeutic doses. Kinetics these agents are lipophilic and have unpredictable gastrointestinal absorption. Peak levels happen 2 to 6 hours postingestion and have enterohepatic recirculation. The imply serum half-life in phase 1 is 1 to 2 hours and the biphasic half-life is 20 to forty hours. Chlorpromazine taken orally has an onset of motion in 30 to 60 minutes, peak in 2 to four hours, and length of four to 6 hours. With sustained-release preparations, the onset is in 30 to 60 minutes and length is 6 to 12 hours. Elimination is by hepatic metabolism, which ends up in a quantity of metabolites (some are active).
Hypotension and myocardial depression are managed by correction of dysrhythmias quit smoking virginia nicotinell 17.5 mg buy without prescription, Trendelenburg position quit smoking symptoms purchase nicotinell 52.5 mg mastercard, fluids quit smoking 6 years generic nicotinell 35 mg on-line, glucagon, or amrinone (Inocor), or a combination of these. Hemodynamic monitoring with a Swan-Ganz catheter or arterial line may be necessary to manage fluid remedy. It is given as an intravenous bolus of 5 to 10 mg3 over 1 minute and adopted by a steady infusion of 1 to 5 mg/h (in youngsters, zero. In large doses and in infusion therapy D5W, sterile water, or saline ought to be used as a dilutant to reconstitute glucagon instead of the zero. Life-threatening hyperkalemia is treated with calcium (avoid if digoxin is present), bicarbonate, and glucose or insulin. Extraordinary measures corresponding to intra-aortic balloon pump assist may be instituted. If seizures or irregular rhythm or vital signs are current, the patient ought to be admitted to the intensive care unit. If a large dose of a sustained-release preparation was ingested, whole-bowel irrigation may be thought of, however its effectiveness has not been investigated. If the patient is symptomatic, quick cardiology seek the guidance of should be obtained, because a pacemaker and hemodynamic monitoring could also be needed. Hypotension and bradycardia could be treated with positioning, fluids, and calcium gluconate or chloride, glucagon, amrinone (Inocor), and ventricular pacing. Calcium normally reverses depressed myocardial contractility but might not reverse nodal depression or peripheral vasodilation. The calcium response lasts 15 minutes and may require repeated doses or a continuous calcium gluconate infusion zero. If calcium fails, glucagon could be tried for its optimistic inotropic and chronotropic impact, or each. Amrinone (Inocor), an inotropic agent, might reverse the consequences of calcium channel blockers. In case of hypotension, fluids, norepinephrine (Levophed), and epinephrine could additionally be required. For cases of calcium channel blocker toxicity that fail to reply to aggressive administration, latest research demonstrate that insulin and glucose have therapeutic worth. Potassium levels must be monitored regularly, as they may shift in response to the insulin. Calcium Channel Blockers Calcium channel blockers are used in the treatment of effort angina, supraventricular tachycardia, and hypertension. Toxic Mechanism Calcium channel blockers scale back inflow of calcium via the gradual channels in membranes of the myocardium, the atrioventricular nodes, and the vascular smooth muscle tissue and lead to peripheral, systemic, and coronary vasodilation, impaired cardiac conduction, and melancholy of cardiac contractility. All calcium channel blockers have vasodilatory action, however solely bepridil, diltiazem, and verapamil depress myocardial contractility and cause atrioventricular block. Toxic Dose 21 Physical and Chemical Injuries Any ingested quantity higher than the maximum day by day dose has the potential of severe toxicity. The maximum oral daily doses in adults and poisonous doses in youngsters of every are as follows: amlodipine (Norvasc), 10 mg for adults and more than zero. Peak impact for verapamil is 2 to 4 hours, for nifedipine 60 to 90 minutes, and for diltiazem 30 to 60 minutes, but the peak motion could also be delayed for six to eight hours. The onset of motion for sustained-release preparations is often four hours but may be delayed, and peak impact is at 12 to 24 hours. Patients receiving digitalis and calcium channel blockers run the chance of digitalis toxicity, as a result of calcium channel blockers improve digitalis levels. Manifestations Cardiac manifestations include hypotension, bradycardia, and conduction disturbances occurring half-hour to 5 hours after ingestion. Hyperglycemia may be current due to interference in calcium-dependent insulin launch. It shifts the oxygen dissociation curve to the left, which impairs hemoglobin release of oxygen to tissues and inhibits the cytochrome oxidase enzymes. Toxic Dose and Manifestations Table thirteen describes the manifestations of carbon monoxide toxicity. Creatine kinase is usually elevated, and rhabdomyolysis and myoglobinuria may happen. This may be misleadingly low in the anemic affected person with less hemoglobin than regular. The manifestations listed in Table 13 for each degree are along with these listed at the stage above. A degree of carbon monoxide larger than 40% is usually related to apparent intoxication. The pulse oximeter has two wavelengths and overestimates oxyhemoglobin saturation in carbon monoxide poisoning. The true oxygen saturation is decided by blood fuel analysis, which measures the oxygen certain to hemoglobin. The patient must be faraway from the contaminated space, and his or her vital capabilities should be established. The mainstay of therapy is 100 percent oxygen by way of a nonrebreathing mask with an oxygen reservoir or endotracheal tube. The fetus should be monitored, as a outcome of carbon monoxide and hypoxia are potentially teratogenic. Metabolic acidosis ought to be treated with sodium bicarbonate provided that the pH is beneath 7. Acidosis shifts the oxygen dissociation curve to the proper and facilitates oxygen delivery to the tissues. The choice to use the hyperbaric oxygen chamber have to be made on the premise of the ability to deal with different acute emergencies that will coexist in the patient and of the severity of the poisoning. Testing ought to embrace the following: general orientation memory testing involving tackle, phone quantity, date of start, and current date; and cognitive testing, involving counting by 7s, digit span, and forward and backward spelling of three-letter and four-letter words. Patients with delayed neurologic sequelae or recurrent signs up to 3 weeks could benefit from hyperbaric oxygen chamber treatment. Chest radiograph may be helpful in cases of smoke inhalation or if the patient is being thought of for hyperbaric chamber. Patients with carbon monoxide poisoning requiring treatment want follow-up neuropsychiatric examinations. Caustics and Corrosives the phrases caustic and corrosive are used interchangeably and may be divided into acids and alkalis. Consumer Product Safety Commission Labeling Recommendations on containers for acids and alkalis indicate the potential for producing serious damage, as follows: � Caution-weak irritant � Warning-strong irritant � Danger-corrosive Some frequent acids with corrosive potential include acetic acid, formic acid, glycolic acid, hydrochloric acid, mercuric chloride, nitric acid, oxalic acid, phosphoric acid, sulfuric acid (battery acid), zinc chloride, and zinc sulfate. Some widespread alkalis with corrosive potential embody ammonia, calcium carbide, calcium hydroxide (dry), calcium oxide, potassium hydroxide (lye), and sodium hydroxide (lye). Oropharyngeal and esophageal harm is more incessantly caused by solids than by liquids. Significant injury is extra doubtless with a substance that has a pH of lower than 2 or larger than 12, with a chronic contact time, and with giant volumes. General scientific findings are stridor; dysphagia; drooling; oropharyngeal, retrosternal, and epigastric pain; and ocular and oral burns. Patients ought to obtain only intravenous fluids following dilution till endoscopic consultation is obtained. The indications are controversial, with some authorities recommending it in all instances of caustic ingestions no matter signs, and others selectively utilizing medical features corresponding to vomiting, stridor, drooling, and oral or facial lesions as standards. We recommend endoscopy for all symptomatic patients or sufferers with intentional ingestions. Some really feel they could be useful for sufferers with second-degree circumferential burns. They suggest beginning with hydrocortisone sodium succinate (Solu-Cortef) intravenously 10 to 20 mg/kg/d within forty eight hours and altering to oral prednisolone 2 mg/kg/d for 3 weeks before tapering the dose. Emergency medical therapy consists of brokers to inhibit collagen formation and intraluminal stents. Interposition of the colon may be needed if dilation fails to provide an adequate-sized passage. Management of inhalation cases requires instant elimination from the surroundings, administration of humid supplemental oxygen, and observation for airway obstruction and noncardiac pulmonary edema. Formaldehyde causes metabolic acidosis, hydrofluoric acid causes hypocalcemia and renal harm, oxalic acid causes hypocalcemia, phenol causes hepatic and renal harm, and picric acid causes renal harm.
The narrowest spectrum quit smoking 1800 number purchase nicotinell 35 mg without prescription, least expensive agent to which the isolated pathogen is susceptible must be chosen quit smoking injection discount nicotinell 52.5 mg line. Longer courses of therapy could additionally be required for choose patients with difficult pyelonephritis quit smoking vapor sticks generic nicotinell 52.5 mg overnight delivery. For outpatients, preliminary empiric remedy with a fluoroquinolone is beneficial, with adjustment of therapy, if needed, based mostly on the outcomes of urine culture. Although potential randomized trials are missing, a number of retrospective studies in addition to several prospective nonrandomized trials suggest that outpatient management is secure for many patients. Pathophysiology Renal calculi are broadly classified into two main categories of calcareous (calcium containing) or noncalcareous stones primarily based on the presence or absence of calcium. Calcareous stones account for approximately 80% of urinary calculi, with the most typical stone composition being calcium oxalate (70%), followed by calcium phosphate (5% to 10%). Commonly occurring noncalcareous stones include struvite or an infection stones (15% to 20%) uric acid (10%) and less-common cystine stones (1%). The strategy of stone formation begins when urine throughout the nephron becomes supersaturated with stone-forming salts that finally precipitate out of solution as crystals. This is a posh process, with interplay between the urinary solutes and stone inhibitors. Natural stone inhibitors corresponding to citrate, Tamm�Horsfall glycoprotein, and nephrocalcin try and block this process, but as soon as the focus of stone-forming crystals reaches a certain threshold (concentration product), stone crystals can form. Small crystals are sometimes unstable and may dissolve; however, if the supersaturated state exists along with low levels of citrate, then the stone crystals form by homogenous aggregation. Once formed, the crystal construction continues to grow by way of a means of heterogeneous aggregation by adsorption of different forms of crystals or cellular debris. Hypercalciuria (more than 200 mg per 24 hours) is the most typical urinary abnormality related to the formation of calcium stones. Type I absorptive hypercalciuria occurs in approximately 55% of stone formers and is recognized with high urinary calcium (more than 200 mg per 24 hours) within the presence of a low-calcium food plan (400 mg/ day). Other, less-common forms of hypercalciuria include increased calcium leakage from the kidney (renal hypercalciuria) or on account of elevated bone resorption from excess parathyroid hormone (primary hyperparathyroidism). Primary hyperparathyroidism is current in lower than 5% of patients with stone disease, however it ought to be considered in any stone affected person with serum calcium higher than 10mg/dL. Hyperoxaluria (more than forty five mg per 24 hours) also can contribute to stone formation. Enteric hyperoxaluria is the most typical cause for increased urinary oxalate and is found in sufferers with chronic diarrhea. Malabsorption of enteric fat results in saponification of divalent cations (calcium and magnesium), leading to increased oxalate absorption. This is commonly seen in patients with short-bowel syndrome, following bariatric surgical procedure, or resulting from inflammatory bowel disease. Increased dietary consumption of oxalate (nuts, chocolate, tea, rhubarb, broccoli, spinach) can also result in hyperoxaluria. Primary hyperoxaluria is the results of an autosomal recessive inborn error of metabolism that may result in early end-stage renal failure (by age 15 years) and dying without a combined liver and kidney transplant. Lastly, a low stage of the oxalate-degrading bacteria Oxalobacter formigenes has been shown to improve the danger of forming oxalate stones. Hyperuricosuria (more than 600 mg per 24 hours) along with a urinary pH lower than 5. High uric acid is commonly the result of a high-protein food regimen however it can also happen in patients with end-ileostomies, gout, or myeloproliferative illnesses. Struvite (infection) stones are composed of magnesium, ammonium, and calcium phosphate and are the leading trigger of huge stones that occupy the complete renal pelvis (staghorn calculi). These stones are caused by urea-splitting micro organism, which result in alkalization of the urine. The commonest organisms related to struvite stones are Klebsiella pneumoniae, Proteus mirabilis, and Follow-up Most sufferers will reply to acceptable antibiotic remedy. International clinical apply pointers for the treatment of acute uncomplicated cystitis and pyelonephritis in women: a 2010 update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Ciprofloxacin for 7 days versus 14 days in girls with acute pyelonephritis: a randomised, open-label and double-blind, placebo-controlled, non-inferiority trial. Moreover, up to 50% of these sufferers will expertise a recurrent stone inside 5 years of their unique episode. Most stone sufferers have their first stone between the ages of 20 and 60 years of age, with peak incidence within the fourth to sixth decade of life. These ages coincide with the years of peak employment and productiveness, which could be affected considerably by kidney stones. Ethnic European men are more probably than Hispanic, Asian, or African American men to develop a stone. Patients who live within the southeastern United States have the best charges of kidney stones when in comparability with residents of other areas, with the very best incidence of stones peaking 1 to 2 months after the most popular months of the yr. Persons with occupations exposing them to continual excessive temperatures have been found to have an roughly eightfold increased price of forming a kidney stone compared to different workers. Simply being adequately hydrated by rising water intake has been shown to decrease stone recurrence charges by virtually a third. Patients with inflammatory bowel illness or with historical past of gastric bypass procedures even have an increased risk for stone formation. Failure to deal with these stones carries an elevated danger of renal damage, sepsis, and possibly dying. Cystinuria (more than 250 mg per 24 hours) leads to stone formation as a end result of an autosomal recessive dysfunction of dibasic amino acid transport. Homozygous patients often present with their first stone during childhood, which may be pure cystine or may be blended with calcium oxalate. Pure cystine stones are radiolucent on plain radiographic imaging and are yellow in look. Ultimately, roughly 98% of stones 5 mm or much less cross spontaneously, taking a mean time of 12 days to dislodge. Invasive Treatment If the affected person has signs of sepsis, intractable ache, or nausea and vomiting, then instant procedural intervention ought to be considered. Options embrace cystoscopy with placement of a ureteral stent to quickly decompress the obstruction, or placement of a percutaneous nephrostomy tube. Septic patients must be emergently decompressed with a ureteral stent or a nephrostomy tube. The determination to suggest a procedural intervention is commonly multifactorial, involving factors corresponding to probability for spontaneous passage, absolute indications for intervention, and patient choice and work and household requirements. Ureteral stones bigger than 1 cm have a minimal chance of passing and require surgical treatment typically. After ureteroscopy a ureteral stent may be left in place, which is usually eliminated within the office in 1 to 2 weeks. Stents are usually well tolerated, however some patients do expertise bothersome urinary symptoms including urgency, frequency, and bladder pain on the finish of urination. Percutaneous entry is obtained by both interventional radiology or by the urologist, and a 30-F working tract is created. The calculus is then fragmented by ultrasonic or pneumatic lithotripsy units, and fragments are eliminated. Clinical Manifestations Patients with renal calculi generally present for evaluation when the stone begins to transfer down the urinary tract. Some patients additionally experience nausea and vomiting throughout these episodes and might have varying amounts of blood within the urine. Patients with staghorn calculi can current with indicators and symptoms of a systemic infection and are at risk for development to sepsis. Diagnosis A thorough historical past ought to be taken during the preliminary analysis, with questions focusing on the nature and location of the pain, radiation of the pain, duration of ache, and presence of nausea, vomiting, dysuria, and hematuria. Questions directly associated to stone disease should be requested, corresponding to private or family history of stone illness, age of first stone, and history of recurrent urinary tract infections. If the patient has had prior stones, it is necessary to ask how the stone was managed, did it move spontaneously or was an intervention required The physical examination often demonstrates important costovertebral angle or flank tenderness to palpation. Patients with fevers, tachycardia, or labile blood pressure and flank pain ought to be considered to have an obstructing stone and should be treated emergently.
Despite this quit smoking cold turkey side effects buy cheap nicotinell 52.5 mg on line, no difference in survival was seen between the tamoxifen and placebo group quit smoking injection purchase nicotinell 52.5 mg on line. Infiltrating lobular carcinoma originates from the lobular buildings of the breast and accounts for 15% of all invasive breast cancers quit smoking hypnosis seminars in my area nicotinell 52.5 mg discount overnight delivery. Other less-common subtypes symbolize lower than 10% and include tubular, medullary, mucinous, and papillary carcinoma. Major adjustments to the staging system embody the next: � All invasive cancers should be assigned a histologic tumor grade using the Elston-Ellis modification of the Scarff-Bloom- Richardson grading system (Nottingham mixed histologic grade). Silverstein confirmed in retrospective studies that the recurrence rate in such sufferers is roughly 4%. Changes within the 2003 American Joint Committee on Cancer staging for breast cancer dramatically have an result on stage-specific survival. At a certain point in the evolution of a breast most cancers, the illness changes from a local illness to a systemic illness. The Halsted paradigm promotes more intensive local remedy to eradicate the most cancers, whereas the Fisher paradigm promotes less aggressive native therapy with the addition of systemic therapy in most girls, even with relatively early illness. Because of this philosophy change and the detection of earlier illness by way of diligent screening techniques, surgical remedy of breast cancer is progressing toward much less radical surgery and extra adjuvant remedy, with equal or better outcomes. Staging of breast cancer can be divided into scientific staging versus pathologic staging. Factors used for scientific staging include the dimensions of the tumor throughout the breast, presence or absence of pathologically confirmed lymph nodes, and presence or absence of distant metastasis. Stage zero is outlined because the presence of in situ illness solely, without proof of nodal or distant metastasis. Stage I is taken into account breast cancer confined to the breast, which is 2 cm or less in size. Exceptions to this general characterization embody tumors with extension to the chest wall or skin and inflammatory breast cancers. The addition of radiation remedy to wide local excision in patients with noninvasive and invasive carcinoma is currently the usual of remedy. Mastectomy A patient with contraindications to breast conservation should have a mastectomy with or with out immediate reconstruction. Total mastectomy surgically removes the breast parenchyma, pectoral fascia, nipple, and the areola complex. A radical mastectomy, not often done at present, includes elimination of the pectoralis major and minor muscles and axillary dissection. One generally used method of breast reconstruction is a tissue expander breast implant. A tissue expander is placed beneath the pectoralis muscles, and expansions are carried out over a period of several weeks to months to stretch the subpectoral pocket to accommodate the permanent implant. The permanent saline or silicone implant is then inserted as a secondary procedure. This process may be carried out as a free flap with the arterial and venous supply anastomosed to vessels within the axilla or as a pedicle flap with the arterial and venous supply from the superior epigastric vessels. Surgical Treatment of the Breast A important paradigm shift in the therapy of breast most cancers has occurred over the past a number of decades. The Halsted paradigm, popularized at the beginning of the 20th century, hypothesized that breast cancer spreads in a contiguous fashion from the breast to the axillary lymph nodes after which to distant websites elsewhere within the body. The Fisher paradigm, which views breast most cancers as systemic from very early in the midst of the disease, modified this Breast Disease Surgical Treatment of the Axilla the standing of the axilla should be assessed for metastases in any patient with invasive breast cancer for a quantity of causes. The presence or absence of axillary lymph node metastases is predictive of the prognosis and facilitates decisions by the medical oncology group concerning adjuvant remedy. Relapse-free survival is closely related to the variety of lymph nodes which are optimistic. In a research of 2873 patients, Hilsenbeck discovered that the relapse-free survival at 5 years was 80% in sufferers with node-negative illness. This quantity decreased to 70%, 60%, and 40% with 1 to three optimistic nodes, four to 9 positive nodes, and greater than 10 constructive nodes, respectively. Surgical elimination of metastatic nodes within the axilla significantly decreases the risk of axillary recurrence. Sentinel Lymph Node Biopsy Axillary dissection traditionally was performed on all patients with invasive breast most cancers. In a study by Specht, 25% of palpable suspicious axillary lymph nodes proved benign on last pathology. The success rate is decided by the variety of nodes beforehand removed, with a success price of 87% when fewer than 10 nodes are removed versus a success price of 47% when more than 10 nodes are removed. The American College of Surgeons Z11 trial, published in 2011, attempted to prove that the elimination of completion axillary dissection in patients with involved axillary lymph nodes was not dangerous to patients. Women with limited axillary nodal metastases and generally favorable index lesions have been randomized to an entire dissection or no further axillary remedy. The examine opened in 1999 and closed in 2004 after accruing solely 891 of the 1900 patients needed to acquire statistical significance. The authors reported that there was no benefit to performing the axillary node dissection within the control group, although the median number of nodes that contained breast cancer was the identical in each arms. Also, the intent to deal with group was included in the treated group, which meant that over one hundred patients who were simply lost to follow-up were included within the analysis. These components allied themselves to render this trial underpowered to adequately address the question that it was ostensibly asking. As a non-inferiority trial (in which we reverse the null hypothesis and the alternative hypothesis) this represents a type 1 statistical error. Despite these essential caveats, the authors concluded that a completion axillary dissection can be prevented in these sufferers. Until further research show in any other case, completion axillary dissection should remain our standard practice. Adjuvant Therapy Historically, adjuvant cytotoxic chemotherapy was used to deal with sufferers with a significant probability for the development of metastatic disease. Randomized clinical trials in patients with negative axillary lymph nodes advised that the risk was adequate in virtually all sufferers whose index tumor was larger than 1 cm in diameter. Herceptin can be given in conjunction with the chemotherapy brokers Adriamycin, Cytoxan, and either Taxol or docetaxel (Taxotere). It may additionally be given with the chemotherapy medication Taxotere and carboplatin (Paraplatin)1 or alone after treatment with a quantity of different therapies, including an anthracycline (Adriamycin)-based remedy. Several different studies looking at threat for recurrence and demise have proven supporting evidence of the advantages of Herceptin use. The potential risk of axillary dissection consists of the accumulation of a seroma, ipsilateral arm lymphedema, and numbness across the space of the intercostal brachial innervation if the nerve is sacrificed at the time of surgical procedure. Because of the lifetime elevated chance of arm lymphedema and possible infection, patients ought to avoid any trauma or procedures such as venipuncture or blood stress measurements on the ipsilateral arm. Wasif reported that only 23% of 537 American Society of Clinical Oncology surgeons and medical oncologists "all the time" carry out an axillary dissection for findings of micrometastatese in the sentinel node. Combination chemotherapy resulted in the enchancment of 10-year-overall survival from 71% in node-negative sufferers not receiving chemotherapy to 78% in those that did receive chemotherapy. This enhance was much more dramatic in node-positive sufferers, with an improvement of overall survival from 42% to 53%. In this group of sufferers, survival was elevated from 67% to 69% when node-negative patients not receiving chemotherapy were compared to these receiving chemotherapy. In node-positive elderly patients, improvement in general survival was additionally minimal, with a rise of survival from 47% to 49% with chemotherapy. Breast cancers are considerably distinctive in their propensity to be dependent upon steroid binding hormones (such as estrogen). Estrogen ablative therapy can be achieved by way of a variety of methods, together with the use of selective estrogen receptor modulators (tamoxifen citrate, raloxifene [Evista]1), aromatase inhibitors (anastrozole [Arimidex], letrozole [Femara], exemestane [Aromasin]) or estrogen receptor downregulators (fulvestrant [Faslodex]). Ablation in premenopausal girls can additionally be achieved surgically by way of bilateral salpingo-oophorectomy. This effect is even higher in the postmenopausal inhabitants, with a 26% proportional discount in 10-year mortality rates.
Patient support groups have been involved by the follow of iron fortification of meals quit smoking 2 12 years nicotinell 52.5 mg buy online, however much of this iron is in an inexpensive form with poor bioavailability quit smoking body effects nicotinell 52.5 mg generic on-line. The growth of a diagnostic genetic take a look at has improved the feasibility of the objective of prevention of morbidity and mortality from hemochromatosis quit smoking inspirational quotes buy nicotinell 52.5 mg online. Vaccinations for Streptococcus pneumoniae, Haemophilus influenzae kind B, and Neisseria meningitidis must be administered earlier than surgery. Hemochromatosis mutations within the common population: Iron overload development rate. Reversibility of hepatic fibrosis in handled hemochromatosis: A study of 36 cases. Examination of the peripheral smear may reveal findings that guide additional diagnostic testing. A useful classification divides the hemolytic anemias mechanistically into immune or nonimmune causes. Alloantibody-induced hemolytic anemia contains hemolytic transfusion reactions and hemolytic illness of the fetus and new child. Hemolysis takes place both in the spleen or liver (extravascular hemolysis) or inside the vasculature (intravascular hemolysis). Anti-I is characteristic of Mycoplasma pneumonia-induced hemolysis, whereas anti-i is characteristic of infectious mononucleosis Paroxysmal Cold Hemoglobinuria. These mechanisms are induced by drug or hapten adsorption, neoantigen formation, and autoantibody binding. Typically, these antibodies are noncomplement binding and trigger extravascular hemolysis. Enzyme defects in the Embden-Meyerhof pathway are typically associated with persistent hemolysis; enzyme defects in the hexose monophosphate pathway are often associated with episodic hemolysis. This enzyme is responsible for diverting glucose from the Embden-Meyerhof pathway to the hexose monophosphate pathway and for restoring intracellular decreased nicotinamide adenine dinucleotide phosphate, which functions as an antioxidant. These substances embrace arsenic; lead; copper; and insect, spider, and snake venoms. Other systemic disease states inflicting hemolysis embrace liver failure and in depth burns. In liver failure, the ratio of ldl cholesterol to phospholipid in the purple cell membrane is altered, resulting in membrane instability and hemolysis. The underlying defect in paroxysmal nocturnal hemoglobinuria is impaired manufacturing of a key anchoring cellular membrane protein. Clinical Manifestations the clinical manifestations of all hemolytic anemias, largely, rely upon the severity of the anemia and the rapidity of the hemoglobin decline in addition to any associated manifestations associated to the underlying trigger. Physical examination not only includes the everyday findings of anemia (pale sclerae and nail beds) however may reveal icteric sclera and jaundice if the indirect bilirubin is sufficiently increased. As noted beforehand, hemolysis can happen within the intravascular or extravascular area, relying upon the etiology. Clinical manifestations of intravascular hemolysis versus extravascular hemolysis differ. Patients with acute transfusion reactions may experience fevers and chills as nicely as flank pain. Specific manifestations of sure disorders can occur and could additionally be helpful in establishing the prognosis. A number of mutations affect the forces maintaining this structural integrity and may end up in degradation and precipitation of the hemoglobin inside the cell. Another hemoglobinopathy, and the commonest, sickle cell disease, outcomes from the alternative of valine for glutamic acid in the sixth position of the -globin subunit. The presence of a Donath-Landsteiner antibody is confirmed by specialized testing aimed toward detecting the temperature dependency of the antibody-mediated hemolysis. The presence of hemolysis at 37 C following incubation at 4 C, but not at incubation at only 4 C or 37 C, constitutes a optimistic antibody take a look at end result. Abnormalities seen on the peripheral smear examination generally recommend the trigger of the hemolysis and direct additional, specialized testing (Table 1). Other checks that could be helpful to verify the presence of hemolysis embrace serum haptoglobin, plasma and urinary free hemoglobin, and urinary hemosiderin. Haptoglobin, synthesized by the liver, binds any free hemoglobin within the plasma; the advanced is then eliminated in hepatic parenchymal cells. If the speed of hemolysis exceeds the clearance price of this complex, the haptoglobin degree might be decreased. Intravascular hemolysis may find yourself in detection of free hemoglobin within the plasma if the plasma hemoglobin-binding proteins are saturated; urine hemoglobin shall be detected if the capability of renal tubular cells to take in free hemoglobin is exceeded. As these cells slough into the urine, the hemosiderin could be detected by a Prussian blue stain approximately 5 to 7 days following a hemolytic episode. This test is therefore useful to detect intravascular hemolysis days after the hemolytic occasion. For the hemolytic anemias, examination of the bone marrow is seldom helpful and usually not necessary in the diagnostic course of. A delayed transfusion reaction is often not appreciated however should be suspected when the hemoglobin level falls more rapidly than anticipated following a transfusion. The diagnosis may be made by demonstrating a brand new serum alloantibody within the recipient of the transfused blood. A urine hemosiderin can additionally be positive, reflecting hemolysis that occurred several days beforehand. Congenital Hemolytic Anemias the analysis of congenital nonimmune hemolytic anemias is usually suspected when the anemia is long-standing. A household historical past of anemia, splenectomy, or gallstones may additionally be a clue to a congenital course of. A specialized take a look at, osmotic gradient ektacytometry, can be used to help in diagnosing these problems. A supravital stain, similar to crystal violet, brilliant cresyl blue, or methylene blue, can show Heinz our bodies. If the diagnosis continues to be suspected after acquiring a normal end result, a repeat take a look at 2 to three months after the acute hemolytic episode must be performed. Hemoglobin electrophoresis ought to be carried out to diagnose a suspected hemoglobinopathy. The commonest hemoglobinopathy causing hemolysis, sickle cell anemia, is quickly identified by this test. However, different hemoglobinopathies inflicting hemolysis, specifically the unstable hemoglobins, could additionally be electrophoretically silent. If the analysis of an unstable hemoglobinopathy is suspected, a supravital stain can show Heinz our bodies and a heat stability test should be obtained for definitive prognosis. The peripheral smear is normally very helpful in diagnosing the acquired causes of nonimmune hemolytic anemias. The peripheral smear can be diagnostic of sure infections (malaria, babesiosis). The diagnosis of paroxysmal nocturnal hemoglobinuria is made by circulate cytometry utilizing peripheral blood cells or bone marrow aspirate and the demonstration of deficiency of hematopoietic cell proteins normally linked to the anchoring glycosylphosphatidylinositol protein. Acquired Nonimmune Hemolytic Anemias the prognosis of acquired causes of nonimmune hemolytic anemias is suspected when a hemolytic anemia is new in onset and previous hemoglobin ranges have been regular. Even although the anemia 851 Differential Diagnosis the differential diagnosis of the hemolytic anemias consists of the reticulocytosis that could be seen with correction of anemia as a end result of alternative of a deficiency (iron, folate, vitamin B12) or recovery from bleeding. Approximately 80% of sufferers have a fast response to corticosteroids, usually inside 1 week after starting therapy. The majority of adult patients obtain high-dose oral prednisone 1 mg/kg/day through the initial part of therapy. Intravenous methylprednisolone (Solu-Medrol) can also be used at day by day doses of a hundred to 200 mg. Hemolytic Anemia 852 Once the hematocrit has elevated, the dose ought to be decreased and subsequently tapered at a gradual price over several months. Rituximab, given at a dose of 375 mg/m2 weekly for 4 weeks, results in an general response fee of 82% with many sustained responses. Recently described is the usage of a lower dose of rituximab, 100 mg, weekly for four weeks. For cases refractory to steroids, splenectomy and rituximab might reply to other immunosuppressive therapies such as cyclophosphamide (Cytoxan), azathioprine (Imuran),1 or cyclosporine (Neoral). Other treatment choices which were used with some success include danazol (Danocrine)1 and plasmapheresis. High-dose intravenous immune globulin (Gammagard)1 could also be effective in some instances, but the response is short-lived (1�4 weeks).






