Torsemide

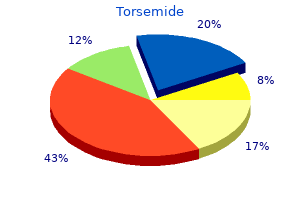
Torsemide
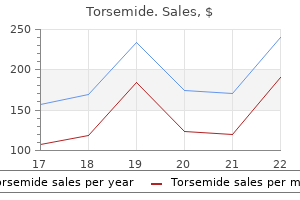
Torsemide dosages: 20 mg, 10 mg
Torsemide packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Orthotic treatment or casting can help cut back the severity of the deformity by sustaining the bones of the foot in proper alignment during the course of the Charcot process hypertension guideline 20 mg torsemide order mastercard. It is extraordinarily important never to walk on the foot without orthosis or solid in place prehypertension at 36 weeks pregnant torsemide 20 mg generic without a prescription. Painless swelling of shoulder joint in syringomyelia with extensive lack of bone mass blood pressure chart omron order 10 mg torsemide fast delivery, effusion, and detritus Severe hallux valgus because of diabetic neuropathic joint illness. Prompt attention to minor trauma is essential to stop progressive of joint disease. Supportive measures such as the usage of braces, splints, orthotics, or casts to stabilize the joint and crutches or a walker could assist to decrease the disability. Physical remedy to promote strengthening and occupational therapy to help in expertise of actions of day by day living must be thought-about. Bisphosphonates could additionally be of worth in retarding injury within the early phases of Charcot arthropathy. Arthrodesis (joint fusion) may be useful in the foot, ankle, knee, or spine after therapeutic of the active section. Acute gouty arthritis is a direct result of the inflammatory response to urate crystals deposited in joint constructions. Primary gout, also described as classic or idiopathic gout, is an inherited inborn error of metabolism and is nearly at all times related to inefficient renal excretion of uric acid. Secondary gout is a consequence of elevated uric acid levels due to systemic sickness or drug. Great toe swollen, purple, painful After repeated attacks Chronic tophaceous arthritis Gout is diagnosed primarily in males. Males have higher levels of serum uric acid than girls till menopause because estrogen has a uricosuric effect. Although the genetic factors underlying hyperuricemia are presumably present at birth, the dysfunction produces no clinical signs or signs until the hyperuricemia has continued for years. Clinical manifestations of gout normally seem in middle age in males (age 30 to 50 years) and later in females (see Plate 5-38). Patients with severe hyperuricemia, and a few others for unexplained causes, may develop gout assaults at a youthful age. The excessive concentration of uric acid within the blood is responsible for gouty arthritis. Some of the factors contributing to hyperuricemia (in addition to the renal inefficiency in excreting uric acid) embrace obesity, meat and seafood ingestion, beer and liquor use, and low dairy intake. Factors that can induce an acute assault of gouty arthritis embody sudden increase or lower within the level of (chronically elevated) serum uric acid, surgical procedure, fasting, alcohol ingestion, and joint trauma. The first scientific proof of gout is often acute arthritis in one or a few peripheral joints. A fulminant synovitis begins abruptly, usually during the night, regularly involving the first metatarsophalangeal joint, midfoot, or different lower extremity joint. The affected joint becomes very swollen, purple, scorching, tender, and excruciatingly painful (see Plate 5-38). If untreated, acute monarticular gouty arthritis lasts three or four days; if a number of joints are severely infected, the assault might persist 2 or 3 weeks. After a quantity of assaults the gouty episodes tend to be more extreme, last longer, and involve a quantity of additional joints, tendons, or bursae. After several years of persistent hyperuricemia, deposits of monosodium urate generally known as tophi type in joint constructions (and different tissues). Tophi are the hallmark of persistent gout, occurring in a big minority of patients. If tophi are periarticular, the affected joints show irregular knobby swelling and indicators of persistent irritation. Tophi typically form in extra-articular constructions as nicely, especially in the extensor tendons of the fingers and toes, the olecranon and infrapatellar bursae, the calcaneal tendon, the cartilage of the exterior ear, and the parenchyma of the kidney (see Plate 5-39). Gout in women might initially contain a number of joints and will embrace the distal interphalangeal finger joints. Radiographs present marked destruction of bone and cartilage and "punched-out" areas in the bone with adjoining bone proliferation stimulated by the urate deposits (see Plate 5-38). The presence of urate crystals in synovial fluid taken from the infected joint confirms the diagnosis and is the gold normal for the diagnosis, which ought to ideally be achieved earlier than initiating lifetime therapy designed to decrease serum uric acid ranges and scale back assaults. Late in the disease, the presence of tophi or attribute radiographic findings makes the analysis obvious. A traditional radiographic finding is the overhanging ledge, which represents intraosseous tophi that break via cortical bone (see Plate 5-38). Decreased excretion of uric acid could be a cause of secondary gout with extended use of diuretics and in nephritis as a outcome of lead poisoning (saturnine gout) or selective tubular dysfunction. The choice of agent is usually dictated by comorbidities, affected person choice, and value. When the serum uric acid concentration is persistently excessive and attacks are frequent, and in all cases of persistent tophaceous gout, the serum uric acid level ought to be lowered to a degree significantly under the saturation level of 6. In most instances, this can be completed with administration of sufficient every day dosages of the xanthine oxidase inhibitor allopurinol. Severe gout might require concurrent remedy with allopurinol and a uricosuric drug if the renal function is fairly normal. Frequent determinations of the serum uric acid focus are required to monitor the effective dosage. However, the initiation of hypouricemic remedy quite regularly causes acute assaults of gout. These attacks may be prevented or decreased with using low-dose day by day colchicine (if renal function is good) for at least several months after initiating uric acid�lowering remedy. With correct treatment and affected person compliance, gout can practically at all times be managed. In sufferers with severe chronic gout, pegloticase results in speedy and profound decreasing of uric acid levels to well below four mg/dL (transiently to ~ 1 mg/dL right after infusion). Pegloticase is a treatment choice (biweekly intravenous infusions) that will quickly resolve tophi, however its use is complicated by anti-drug antibodies that cause important infusion-related allergic reactions and lack of efficacy. The dramatic uric acid�lowering impact is predictably related to dramatic and extreme flares in gouty arthritis. Serum calcium, phosphate, and alkaline phosphatase levels are normal, as is urinary calcium excretion. Attacks are notably frequent after parathyroidectomy as therapy for hyperparathyroidism. Other circumstances have weaker associations, together with hypothyroidism, Wilson illness, and acromegaly. The crystals might induce inflammation by similar mechanisms to the urate crystal�induced synovitis of gout (see Plates 5-38 and 5-39). Pseudogout affects women and men, and sufferers are typically middle-aged or aged. A self-limiting dysfunction, an episode of pseudogout lasts from 1 or 2 days to a number of weeks. However, in some sufferers a subacute or persistent polyarthritis happens that resembles rheumatoid arthritis. This manifestation happens both with or without the assaults of acute synovitis typical of pseudogout. About half of older patients with chondrocalcinosis (mostly women) also exhibit progressive degenerative modifications in plenty of joints (osteoarthritis). The knee joint is the most typical website of involvement, adopted by the wrist, metacarpophalangeal, hip, shoulder, elbow, and ankle joints. Most joints with radiographic indicators of chondrocalcinosis are asymptomatic, even in sufferers with synovitis in other joints. Diagnosis of pseudogout should be suspected in instances of acute synovitis in a large joint of an older particular person whose serum uric acid level is normal. Biopsy disclosed calcium pyrophosphate crystals seen underneath polarized gentle microscopy. Anteroposterior radiograph of knee reveals densities as a outcome of calcific deposits in menisci. In lateral radiograph, calcific deposits in articular cartilage of femur and patella appear as fluffy white opacities.
Sublobular vein Central vein Hepatic vein Liver arteria coronaria sinistra 10 mg torsemide generic with mastercard,Gallbladder blood pressure 3rd trimester purchase 10 mg torsemide with amex,andExocrinePancreas 313 Interlobular connective tissue Central vein Hepatocyte cords Portal triad Portal triads Portal triad in portal tract Proper hepatic artery Hepatic portal vein Common hepatic duct Perivascular fibrous (Glisson) capsule extending into porta hepatis alongside vessels and bile duct Hepatic lobule pulse pressure is quizlet discount 20 mg torsemide visa. Liver organized as series of hexagonal lobules, every composed of sequence of hepatocyte cords (plates) interspersed with sinusoids. Each lobule surrounds a central vein and is bounded by 6 peripheral portal triads (low magnification). Its boundaries are marked by portal areas (arrows) at its corners, varied quantities of connective tissue, and portal triads. The remaining 20% is stroma, a delicate supportive framework of connective tissue that types the outer Glisson capsule. At the porta hepatis, this capsule is steady with the arborization of connective tissue that accompanies the branching pattern of the entering hepatic artery and portal vein and the emerging bile duct. In humans, the lobules are poorly outlined, the amount of connective tissue between lobules being scanty. In each lobule, a fragile stroma of reticular fibers forms a supportive network for hepatocytes and surrounding sinusoids. Hepatocellular carcinoma-the most common primary hepatic neoplasia-usually arises from hepatocytes. Chronic liver disease-most typically related to persistent hepatitis B or hepatitis C infection-is the leading cause. Clinical indicators may include hepatomegaly, jaundice, fatigue, and elevated serum levels of certain liver enzymes. More commonly, the liver is concerned in metastatic (or secondary) unfold of tumors from different websites. In most patients with metastatic liver illness, such malignancies mainly arise from the lung, colon, pancreas, and breast. Depending on the stage of disease, therapy choices differ and embrace surgical resection, focused radiation remedy, percutaneous hepatic perfusion of chemotherapeutic agents, and liver transplant surgical procedure. Hepatocytes in liver arranged as cell plates separated by thin-walled hepatic sinuosids. Glycogen in liver cells (Above) stained with Best carmine (Left), easy H&E (Right). Hepatic artery branch Portal vein branch Bile ducts Sinusoids Liver cell "plates" Central veins (tributary to hepatic vein through sublobular veins) Portal triad Portal department Bile ducts Bile ductules Bile canaliculi Hepatic artery department Normal lobular sample with portal triad. Portal triads surrounded by small amounts of interlobular connective tissue sit at corners of every lobule in areas called portal tracts, around which are limiting plates of hepatocytes. Triads also mark peripheral meeting locations of adjoining lobules, which appear to be a mosaic of interlocking tiles. In transverse part, each lobule consists of plates of hepatocytes, one or two cells thick, which are separated by hepatic sinusoids and seem to radiate out from a small central vein. Hepatocyte arrangement resembles that of a sponge, with sinusoids represented by the areas. Each triad consists of a branch of the bile duct, portal vein, and hepatic artery, which divide into smaller branches. The portal vein brings nutrient-rich blood from the gastrointestinal tract-75% of the total blood to the liver; hepatic arteries provide 14. Terminal branches of portal veins, about 300 mm in diameter, frequently give off inlet venules, which empty into thin-walled, fenestrated hepatic sinusoids which are in intimate contact with hepatocytes. Terminal branches of hepatic arteries, which ramify with portal vein branches, end as arterioles that drain into sinusoids, which thus obtain a combination of arterial and venous blood. Sinusoids converge towards a central vein, also known as a terminal hepatic venule, and empty into it within the middle of each lobule. Central veins unite to kind sublobular veins, which lead into larger hepatic veins that travel alone and branch repeatedly. Hepatic veins coalesce to be a part of the inferior vena cava, the primary drainage route of blood from the liver. Important for understanding lobule group and hepatocyte operate, blood and bile move by way of lobules in opposite instructions. This thin-walled vein is surrounded by parenchyma and receives blood from several sinusoids. In transverse part, the hepatic arteriole consists of 1 to three layers of clean muscle cells and a relatively small lumen. The portal venule has a larger, often collapsed lumen with a more attenuated wall. The bile ductule is lined by simple cuboidal to columnar epithelium and drains exocrine secretions of hepatocytes from the liver. The lumen of every central vein has numerous openings, which permits a number of hepatic sinusoids to drain freely into them. The parenchyma is manufactured from hepatocytes organized in common, branching, interconnecting plates that are interposed with a community of thin-walled hepatic sinusoids. Hepatic sinusoids Lymph vessel Connective tissue Bile duct Periportal bile ductule (canal of Hering) Portal vein branch Portal arteriole Hepatic artery branch Periportal arteriole Intralobular arteriole Inlet venule Central vein Sinusoids Central veins Perisinusoidal areas (of Diss�) Sublobular vein Central vein Three-dimensional schematic of liver structure. In this section of fetal liver, hepatic sinusoids are replete with nucleated blood cell precursors. The parenchyma consists of an anastomosing network of interconnecting plates, one or two cells thick, which resemble walls of a building with spaces in between. In humans, one-cell-thick plates are commonest in the normal adult liver; two-cell-thick plates happen within the embryo and in adults during regeneration in sure ailments. Via electron microscopy or particular mild microscopic methods, slim fluid-filled perivascular spaces-spaces of Diss� (or perisinusoidal spaces)-can be seen separating the endothelial lining of sinusoids from the hepatocyte surfaces. These spaces allow plasma to circulate between sinusoidal lumina and hepatocyte surfaces, which allows speedy change of soluble, noncellular substances between blood and parenchyma. In the fetus and in continual anemias, these spaces are sites of extramedullary hematopoiesis. Hepatic lymph originates in these spaces and eventually drains to small lymphatic vessels in portal tracts. Oval to ellipsoidal, the acinus comprises parts of two adjoining classic hepatic lobules. The border between the 2 lobules forms the central equatorial axis of the acinus, around which are three concentric zones (1, 2, 3). Its brief axis runs along the border of two basic hepatic lobules; its long axis is an imaginary line between two central veins closest to the brief axis. Hepatocytes within the acinus are arranged in three concentric, elliptical zones across the quick axis. Zone 1, most central, is closest to the terminal distributing branches of the portal venule and hepatic arteriole. This zone first receives oxygen, hormones, and nutrients from the bloodstream, and most glycogen and plasma protein synthesis by hepatocytes occurs here. Zone 3 is furthest from the distributing vessels; between zones 1 and three is the intermediate zone 2. A gradient of metabolic exercise exists for many hepatic enzymes in the three zones. The highest elevations occur in patients with acute viral hepatitis and toxin-induced hepatic necrosis. A high ratio suggests advanced alcoholic liver disease; decrease values are seen in those with viral hepatitis. Whereas persistent disorders, similar to cirrhosis, result in decreased serum levels of albumin (a protein synthesized exclusively in the liver), bile duct obstruction and intrahepatic cholestasis cause elevations in alkaline phosphatase (an enzyme current in the biliary duct system). Fibroblasts and small vessels, together with an arteriole (A) and lymphatic channel (L), are interspersed with densely packed connective tissue fibers. A skinny extension of Glisson capsule (arrows) getting into the hepatic parenchyma consists of connective tissue, which accommodates small blood vessels. The mesothelium acts as a shield, particularly in opposition to entry of pathogenic bacteria and other probably dangerous substances. The capsule comprises often organized collagen and elastic fibers and supplies exterior support and form to the liver.
Subendothelial connective tissue in these veins contains a community of elastic fibers with scattered fibroblasts arteria jugular torsemide 10 mg purchase otc. In contrast blood pressure chart webmd discount torsemide 10 mg fast delivery, the adventitia-the thickest layer in massive veins-may contain bundles of longitudinally oriented easy muscle cells interspersed with collagen and elastic fibers blood pressure pediatric 10 mg torsemide proven. At their entrances to the center, venae cavae and pulmonary veins have a small quantity of cardiac muscle in the adventitia. Compared with arterial partitions, partitions of veins have extra in depth vasa vasorum, penetrating from the adventitia into deeper areas. Most generally affected veins are superficial ones in the upper and decrease elements of the legs. Varicose veins can also develop within the esophagus on account of cirrhosis of the liver or within the hemorrhoidal venous plexus on the rectoanal junction. Such varicose dilations normally happen when valves turn out to be weakened and incompetent. Another critical complication is deep vein thrombosis, which may lead to pulmonary embolism. In this partly constricted artery, the lumen (*) caliber is small relative to the muscular wall thickness. The arterial wall has extra elastic fibers (in black), whereas the vein has more collagen (in orange). Walls of both muscular arteries and veins have three tunics, every structurally totally different in accordance with vessel kind. Smooth muscle dominates the tunica media, which is the thickest layer of the arteries. The number of smooth muscle layers varies with artery measurement: from 3-4 in small arteries to 20-40 in larger ones. In the media, smooth muscle cells are circularly or helically disposed and communicate with neighboring muscle cells through hole junctions. Between smooth muscle layers are variable numbers of elastic fibers mixed with collagen fibers and occasional fibroblasts. Larger arteries have elastic fibers organized concentrically in laminae, which type a conspicuous inside elastic lamina at the border with the intima and an exterior elastic lamina on the interface with the adventitia. As muscular arteries become smaller, the number of elastic fibers and layers of clean muscle steadily lower. The tunica adventi tia-loose connective tissue containing helically or longitudinally oriented collagen and elastic fibers-usually blends imperceptibly with surrounding connective tissue. A thin intima is adjoining to a deeper media, which incorporates small bundles of circularly arranged smooth muscle cells. Walls of veins usually have extra collagen, which imparts great tensile energy, than elastic fibers. The adventitia is prominent, with longitudinally oriented easy muscle interposed with massive quantities of collagen. Veins have well-developed vasa vasorum in their partitions, and many veins have valves, that are folds of intima with a connective tissue core lined on either side by endothelium. Not the same as frostbite, it may happen alone or as a half of extra serious diseases. Skin discoloration in affected areas is attributable to arterial spasm inflicting severely restricted blood flow. Small arteries of digits show endothelial dysfunction, intimal thickening, and luminal narrowing. Episodes might last less than 1 minute to several hours; affected digits quickly flip white due to diminished blood flow, then seem blue (cyanosis) due to prolonged lack of O2, and switch pink because of sudden vascular dilation. Although the etiology is unknown, a2-adrenergic receptors on vascular easy muscle cells are hypersensitive in individuals with this dysfunction. Endothelium 183 Left coronary artery Smooth muscle cell Collagen Lamina propria Intima Circumflex department of left coronary artery Right coronary artery Internal elastic lamina Muscle and elastic tissue External elastic lamina Collagen fibers Adventitia Vasa vasorum Media Verhoeff-van Gieson. Note nearly complete occlusion of lumen (*) by intimal atherosclerosis with fatty accumulation and calcium deposition. These arteries are often concerned in atherosclerosis and coronary artery disease, so information of their regular histology is important. Like different arteries, coronary arteries encompass three concentric tunics with a histologic structure much like that of other muscular arteries, plus unique features. The adventitia, for instance, is kind of thick relative to that of other muscular arteries; it consists of loosely packed collagen, adipose tissue, and a few elastic fibers. Because coronary arteries bend repeatedly during systole and diastole, each media and adventitia contain bundles of longitudinally oriented clean muscle as properly as circularly organized bundles. Coronary arteries are additionally distinctive in their excessive collagento-elastic fiber ratio, which displays excessive tensile power and relatively low stretchability. Branching sites of these arteries show normal, periodic thickenings of the intima, known as musculoelastic cushions. These focal areas may contribute to development of atherosclerosis (via accumulation of low-density lipoproteins and speedy lesion formation). Collateral connections between arterioles type in response to disease-induced obstruction of a coronary artery. Compared with males, women usually have coronary arteries with smaller diameters, so coronary artery surgical procedure is commonly tougher and will contribute to a poorer outcome. Involvement of coronary arteries may lead to ischemic coronary heart disease and life-threatening myo cardial infarction. High circulating ranges of low-density lipoproteins injury arterial endothelium, which normally results in formation of atherosclerotic plaques. Blood monocytes migrate throughout the endothelium to turn out to be macrophages, which accumulate lipids. Smooth muscle cells within the media also migrate to affected intimal websites and turn into cholesterol-laden foam cells. These modifications could set off formation of a thrombus, which may obstruct lumina of affected arteries. Arterioles, which department repeatedly and become smaller, are simply distinguished from larger muscular arteries through diameter-outer diameters of one hundred mm and inside diameters of about 30 mm-and the variety of clean muscle cells within the walls. Arteriole partitions are thick relative to the lumen, with the media, essentially the most distinguished tunic, consisting of one or two layers of carefully packed, helically organized easy muscle cells. Physiologically, arterioles are resistance vessels and can undergo vasoconstriction or vasodilation in response to neural and nonneural stimuli. Deep to the intima is an internal elastic lamina, which is prominent in bigger arterioles however both extremely thin or absent in the smallest arterioles; in sections this lamina often appears corrugated, depending on the state of vessel constriction at fixation. Arteriolar adventitia consists largely of loosely organized collagen and elastic fibers. Arterioles obtain blood from larger muscular arteries and ship blood to capillaries. Terminal segments of arterioles, or metarterioles, encompass a single layer of smooth muscle and, by vasoconstriction, management the quantity of blood coming into capillaries. Because the vasculature had been perfused before tissue processing, the arteriole looks distended and the venule is barely collapsed. The venule, nevertheless, lacks easy muscle and has ill-defined tissue layers in its wall. Walls of each vessels contain processes of fibroblasts (Fi) and collagen fibers (Co). Both vessels are lined by steady endothelium, though that of venules is normally looser than that of arterioles. Intraluminal strain differences usually trigger venules to appear collapsed in part and with an irregular contour; arterioles often have round profiles because of a comparatively excessive elastin content material in the walls. Its coordinated contraction enables blood flow and distribution to be regulated before entering capillaries. The skinny venule wall is adapted to features in fluid change and as common sites of transendothelial leukocyte migration, known as diapedesis. Endothelium (En) strains the lumen, and an intercellular junction (circle) lies between two endothelial cells. As secretory cells, they produce giant quantities of elastic tissue in arterial walls and different connective tissue elements of extracellular matrix, corresponding to collagen fibers and ground substance. These cells, usually arranged in helical or circular layers, are linked to adjacent smooth muscle cells by many hole junctions. These intercellular specializations are websites of electrical coupling that allow cells to act synchronously, especially during narrowing of the vessel lumen.
Less widespread kidney tumors are transitional cell carcinoma blood pressure jumps up and down 10 mg torsemide cheap free shipping, Wilms tumor heart attack vol 1 pt 14 torsemide 10 mg purchase without prescription, and renal sarcoma blood pressure 50 purchase torsemide 10 mg amex. Each cell has a spherical euchromatic nucleus surrounded by cytoplasm full of organelles. Apical canaliculi (Ca), quite a few vesicles (*), and plenty of pleomorphic mitochondria (Mi) are seen. Mitochondria (Mi) and endocytotic vesicles under the plasma membrane (arrows) are shown. Extensive interdigitations of plasma membranes, which are linked by intercellular junctions, make lateral cell boundaries indistinct. Apical components of cells present tubular invaginations of the cell membrane and heaps of vesicles and canaliculi within the cytoplasm. These morphologic features are in maintaining with epithelial cells concerned in energetic transport. Proximal tubules resorb greater than 60% of the glomerular filtrate, including a lot of the water, glucose, amino acids, bicarbonate, ascorbic acid, and all the protein. Nuclei of straightforward squamous cells of the parietal layer of Bowman capsule are indicated (*). The ascending thick limb of the distal tubule returns to the renal cortex and contacts the vascular pole of its own renal corpuscle between afferent and efferent arterioles. At this contact web site, a cluster of dark-stained cuboidal cells with intently packed nuclei constitutes the macula 16. These membrane-bound vesicles (10-40 nm in diameter) have a moderately electron-dense core, typically with a crystalline interior. They include the hormone renin or its precursor and are polarized toward the cell membrane, adjoining to the afferent arteriole endothelium. Renin regulates systemic arterial blood strain and influences sodium ion (Na+) focus. Renin can be engaged in feedback management of glomerular filtration price in particular person nephrons by way of the renin-angiotensin system. Cells of the macula densa are narrow, carefully packed epithelial cells of the distal tubule. The macula densa screens Na+ ranges and ultrafiltrate quantity within the distal tubule lumen. It is lined by a skinny layer of straightforward squamous epithelial cells, which have nuclei (small arrows) protruding into the lumen. Other areas include blood capillaries and ascending (straight) portions of distal tubules. Sparse organelles, corresponding to vesicles (Ve) and a few lysosomes (Ly), characterize the cytoplasm. Except for a somewhat thicker wall and lack of blood cells, Henle loops resemble systemic capillaries. Loops encompass flattened epithelial cells with nuclei (*) that bulge slightly into the lumen. Capillaries that type the vasa recta are near the loops and have very thin walls. The flattened cells are 1-2 mm thick and have lenticular, carefully spaced nuclei that protrude into the lumen. Henle loops intently resemble blood capillaries, but their epithelium is thicker than the endothelium of surrounding capillaries. Intercellular junctions, including tight junctions and desmosomes, link cell processes laterally. Highly permeable to water, Henle loops play a task in the countercurrent multiplication a part of urinary concentration by establishing a focus gradient in tissue fluid. Lined by massive, pale cells with round nuclei, the tubules normally cross medullary rays that penetrate the cortex. Simple cuboidal to low columnar epithelium characterizes accumulating tubules (*); the smaller loops of Henle are made of easy squamous epithelium. These vessels are intimately associated with loops of Henle and accumulating ducts and function as countercurrent exchangers. Conduits for urine, they start in the cortex as arched amassing tubules, which prolong toward the medulla in medullary rays. They then merge with different arched tubules to form straight accumulating tubules that run within the medulla. At tips of medullary pyramids, papillary ducts perforate the renal papilla to form the area cribrosa. In transverse section, most accumulating tubules show a large lumen; proximal and distal tubules have comparatively narrow lumina. Along their extent, the collecting tubule diameter progressively will increase, as does the height of the epithelium. Lining cells bulging into the lumen kind a simple epithelium, which ranges from cuboidal to low columnar. Their bases rest on a skinny basement membrane, and their apical surfaces contact a big central lumen. A lack of intercellular projections or invaginations makes lateral cell borders extra distinct than in different parts of the uriniferous tubule. Each cell has a round, central nucleus, pale cytoplasm, and relative paucity of organelles in comparison with different components of the uriniferous tubule. Around nuclei is commonly a halo pattern, which is due mostly to glycogen that by light microscopy usually appears washed out. Short basal infoldings of plasma membrane (arrows) improve floor area and comprise ion pumps. Tight junctions (circle) hyperlink apicolateral cell borders and seal the lumen from the extracellular space. Dark cells, which can play a extra active function in urine acidification, have extra organelles, apical vesicles, and basal infoldings than do gentle cells. Apical surfaces of dark cells also have extra quite a few and stubby microvilli; mild cells could bear a single cilium. Tight junctions join each cell types; basal plasma membranes rest on a thin basement membrane. Thus, not only are accumulating ducts conduits, however they also play a job in concentrating urine and regulating acid-base steadiness. Somite Intermediate mesoderm (nephrotome) Pronephric tubule Pronephric duct Ectoderm Pronephric duct forming UrinarySystem 375 Dorsal aorta Glomerulus Coelom Gut Pronephric tubules degenerating Mesonephric duct Mesonephric tubules in nephrogenic tissue Ureteric bud (metanephric duct) Metanephrogenic tissue Topography of the pronephros, mesonephros, and metanephric primordium. Somite Dorsal aorta Glomerulus Posterior cardinal vein Mesonephric duct Mesonephric tubule Genital ridge Coelom Gut Cloaca Horseshoe kidney. This widespread renal fusion defect occurs when intermediate mesoderm that provides rise to the metanephric blastema fails to separate. Both techniques arise from mesoderm: At 4 weeks of gestation, intermediate mesoderm separates from successive somites to type segmentally arranged nephrotomes, which are simply lateral to the genital ridge. They give rise, in a cranial to caudal path, to three successive kidneys-pronephros, mesonephros, and metanephros. The pronephros forms seven pairs of pronephric tubules and a pronephric duct, which extends to the caudal a half of the embryo to attain the cloaca. The vestigial and nonfunctional human pronephros is rapidly changed caudally by the mesonephros, which serves briefly as an excretory organ within the fetus. The mesonephros consists of tubules that fuse with an extension of the pronephric duct, known as the mesonephric (wolffian) duct. Successive formation of tubules in the caudal part of intermediate mesoderm continues for several weeks, with 16. Primitive renal glomeruli form in the mesonephros between blind ends of tubules and capillaries derived from branches of the dorsal aorta. After mesonephros regression, the metanephros (permanent kidney) appears in the fifth week of gestation. Other than symptomatic remedy, surgical intervention may be undertaken in some circumstances to improve urine flow. Mesonephron Mesonephric duct Hindgut Cloacal membrane Cloaca Metanephrogenic tissue Metanephric duct (ureteric bud) Metanephrogenic tissue Capsule Pelvis Major calyx Minor calyx Collecting ducts Nephroblastoma (Wilms tumor).
The cells in vitro are known to be linked by gap junctions hypertension vision order torsemide 10 mg fast delivery, which has similarities to the in vivo situation blood pressure medication kills torsemide 10 mg discount without prescription. Most are glial filaments blood pressure chart what your reading means 20 mg torsemide with visa, though actin filaments, in addition to microtubules, can also occupy the cell interior. Although not nicely resolved at this magnification, gap junctions are an essential junction kind that electrically links the cells. This heterogeneous population consists of fibrous and protoplasmic astrocytes within the mind and spinal wire, M�ller cells in the retina, and pituicytes in the posterior pituitary. Many elaborate, branched cell processes lengthen from the stellate cell bodies into the encircling parenchyma of the mind and spinal wire. Terminal expansions of the processes, often known as perivascular end-feet, kind an intimate relationship with surfaces of small blood vessels, with a whole masking forming around capillaries. They are additionally discovered round preliminary segments of neurons and naked axonal segments, the nodes of Ranvier. It is the most typical type of glioma (tumor of glial cells) and might happen in most components of the mind or spinal cord. It usually develops in the frontal and parietal lobes of the cerebrum and is most typical in adults, especially middle-aged men. At least three differing kinds exist, the most malignant of which is glioblastoma multiforme. As for many brain tumors, the etiology is unknown, and analysis making an attempt to uncover attainable causes is beneath way. Tight junction Capillary endothelial cell Astrocyte Histpathology: perivascular infiltration with mononuclear cells in disrupted mind tissue. These endothelial cells have sparse pinocytotic vesicles, which take part in lively, unidirectional transport of protein and fluids from blood to brain. The end-feet cowl greater than 85% of the floor of the basement membrane; between the end-feet are gap junctions, which allow transport of potassium and other ions between the blood and the neuronal microenvironment. Acute encephalitis is mostly a viral an infection, whereas a kind that results in abscess formation often implies a extremely damaging bacterial an infection. A diffuse inflammatory response commonly impacts grey matter disproportionately in contrast with white matter. Overlying basement membrane is barely seen at this magnification, and the perivascular area may be very slender. Scattered organelles, including a number of mitochondria of varied sizes, occupy cytoplasm of the astrocyte. Surrounding nervous tissue, generally recognized as the neuropil, consists of many tightly packed processes of neurons and glia. A few brain regions-pineal gland, posterior pituitary, and elements of the hypothalamus-lack this barrier and contain capillaries which would possibly be highly permeable and fenestrated. Unmyelinated axons of peripheral neurons (sensory, somatic motor, or visceral motor) being surrounded by cytoplasm of a neurilemmal (Schwann) cell Neurilemmal (Schwann) cell Periaxonal area Axons Axon B. Myelinated axon of peripheral neuron (sensory, somatic motor, or visceral motor) being surrounded by a wrapping of cell membrane of a neurilemmal (Schwann) cell Neurilemmal cell Axons C. Concentric rings of Schwann cell membrane that kind the multilayer myelin sheath encompass the axon. Axoplasm (cytoplasm of the axon) of the nerve fiber and the surrounding extracellular space are seen. Myelin is an electrical insulator that will increase conduction velocity of nerve fibers and is the bodily foundation for speedy saltatory conduction (in which impulses bounce from one node of Ranvier to another). Myelination, a sequence of advanced occasions, begins in the third fetal trimester and ends throughout early childhood. They are known as myelinating and nonmyelinating Schwann cells, though differentiation into two groups is probably mediated by axons: nonmyelinating cells collectively ensheath groups of several small axons; myelinating cells are most frequently associated with one massive axon. Unlike oligodendrocytes that wrap around numerous axons, one Schwann cell myelinates one section of an axon. Schwann cells also help debris removal and function guides for sprouts of regenerating axons after damage. Damage to myelin is widespread in neurologic diseases and leads to blocked axonal conduction, secondary damage to axons, and probably permanent neurologic deficits. Campylobacter jejuni, a major reason for bacterial gastroenteritis, is the most frequent infectious agent; others are cytomegalovirus, Mycoplasma pneumoniae, and Epstein-Barr virus. Symptoms are progressive ascending weak spot (flaccid paralysis) of the limbs, diminished tendon reflexes, and autonomic dysfunction. Histopathology includes lymphocytic (mostly Tcell) infiltration of endoneurium of peripheral nerves followed by macrophage-mediated segmental demyelination of nerve fibers. By electron microscopy, macrophage pseudopodia are seen penetrating Schwann cell basal laminae close to nodes of Ranvier. It is likely that immune responses directed to the infectious pathogen induce manufacturing of antibodies to gangliosides and glycolipids. The cytoplasm (Cy) of this myelin-producing cell incorporates many scattered ribosomes and profiles of rough endoplasmic reticulum. Several myelinated nerve fibers (*) are in close contact with the cell and appear to be embedded in its cytoplasmic processes. Several skinny cytoplasmic processes emanate from the cell body, so, as its name implies, the oligodendrocyte resembles a tree with a couple of branches. Their cytoplasm accommodates abundant free ribosomes and tough endoplasmic reticulum, scattered mitochondria, and a Golgi complicated; the cytoplasm can also be replete with microtubules but lacks intermediate filaments and glycogen. During myelination, the plasma membrane of the oligodendrocyte becomes tightly wrapped round axons, the number of layers determining the thickness of the myelin sheath. The disease course is unpredictable, and the sort and severity of symptoms can differ significantly. Although its etiology remains enigmatic, a leading principle proposes an autoimmune or viral cause. A few isolated ependymal cell nests (arrows) are also seen nearby, and their presence is normal in the adult. The central canal of the spinal twine is often patent in the youngster and younger grownup however with advancing age usually becomes obliterated. The ventricular lumen (*) has a ciliated ependymal lining composed of carefully apposed cuboidal cells, some of which bear apical cilia (arrows). These cells bear apical microvilli to improve surface area, and most also have motile cilia that project into the ventricular lumen. Characteristic of the ependyma is the presence of apical intercellular junctions between lateral borders of contiguous cells; different forms of junctions are adherens, tight, and gap junctions. Intracranial lesions, arising from the roof of the fourth ventricle, normally happen in youngsters, whereas spinal cord tumors typically occur in adults. Treatment is dependent upon neurosurgical intervention to facilitate definitive prognosis. Postoperative adjuvant therapy contains radiation of the brain or spinal wire, chemotherapy, or radiosurgery. A causal relationship between these mutations and tumor development has not but been proved, nonetheless. Hemisection of brain, brainstem, and spinal cord, with the extent of section through the anterior diencephalon proven. A leaf-like course of covered by simple cuboidal epithelium (Ep) is raised into small surface protrusions referred to as villi (Vi). The choroid plexus consists of extremely branched leaf-like folds of vascularized pia mater covered by a modified ependyma, which is a secretory and ion-transporting epithelium. This easy cuboidal or low easy columnar epithelium rests on a skinny basement membrane. A core of free connective tissue of the pia mater accommodates a tortuous community of enormous fenestrated capillaries which might be highly permeable. This course of involves lively transport of sodium ions and passive diffusion of water. Tight junctions link lateral borders of epithelial cells, and basal membranes of the cells have many infoldings just like those seen in different ion-transporting epithelial cells. With age, frivolously eosinophilic and calcified concretions, generally recognized as corpora arenacea, might accumulate within the choroid plexus. To purchase fluid, a spinal needle is inserted into the subarachnoid house between lumbar vertebrae L3/L4 or L4/L5.
The cell is associated with two intently apposed fenestrated capillaries and abuts two different spongiocytes arrhythmia list buy torsemide 20 mg free shipping. A euchromatic nucleus with a distinguished nucleolus (nu) is typical of this lively cell blood pressure chart runners torsemide 20 mg generic overnight delivery. Non�membrane-bound lipid droplets blood pressure zestril torsemide 10 mg low cost, additionally ample, are storage websites for ldl cholesterol, a precursor to corticosteroid hormones. Mitochondria right here have an elevated floor space of internal cristae to accommodate catalytic enzymes concerned within the cleavage. Lipid-soluble hormones are launched into the bloodstream via adjoining fenestrated capillaries. Spongiocyte plasma membranes often bear short, stubby microvilli, which amplify surface space for secretion. Next to the perivascular space, these membranes are in contact with a skinny, intervening basal lamina of the attenuated, fenestrated endothelium of adjoining capillaries. Ultrastructural options of secretory cells in zonae glomerulosa and reticularis are similar to these of spongiocytes in the fasciculata, however normally fewer lipid droplets are found. Lipofuscin, a wear-and-tear pigment associated with tertiary lysosomes, is often extra plentiful in the zona reticularis than in other cortical layers. Part of the zona reticularis (Left) shows spongiocytes and a closely associated network of sinusoidal capillaries (*). Closely packed chromaffin cells have spherical euchromatic nuclei and cytoplasm filled with many dense-core secretory vesicles. Vesicles storing epinephrine are often smaller with a light-weight or reasonably dense core. These Golgi-derived cytoplasmic organelles, 150-350 nm in diameter, are storage websites for the 2 major peptide hormones of the medulla. As a rule, epinephrine is stored in smaller vesicles with a light-weight or moderately dense core; norepi- 10. Mammals such as rodents have two kinds of chromaffin cells- one with only epinephrine vesicles and one with entirely norepinephrine vesicles. In humans, nonetheless, most vesicles comprise norepinephrine, and the identical chromaffin cell typically consists of both hormones. Preganglionic sympathetic neurons, which innervate these cells, regulate their secretion. Immunofluorescent remedy localizes antibodies to insulin in beta cells (Red) and glucagon in alpha cells (Green). Asadi) Relative density of distribution of islets in various elements of the pancreas. Gomori aldehyde fuchsin and ponceau stain: beta granules stain purple; alpha granules, orange-pink. Delicate free connective tissue (*) invests a compact mixture of pale islet cells. Precise identification of particular person cells requires both electron microscopy or more specialised immunocytochemistry. Triple-labeling reveals localization of antibodies to insulin in beta cells (Red), glucagon in alpha cells (Blue) and somatostatin in delta cells (Green). Early in embryonic development, groups of cells arise from ends of endodermally derived ducts after which lose connection with them. These cells kind small spherical clumps and become the endocrine components of the pancreas, the islets of Langerhans. Richly vascularized, islets are incompletely separated from the exocrine pancreas by scanty funding of delicate reticular connective tissue. Vascular supply to every islet via an insuloarterial portal system consists of several afferent arterioles at the islet periphery leading into a wealthy network of fenestrated capillaries. Large capillaries leaving each islet ramify into capillaries that offer blood to surrounding pancreatic acini. Islet cells make up compact, cord-like clusters and in H&E sections seem as closely packed, pale-stained polygonal cells. Such tumors might produce elevated circulating levels of specific hormones, inflicting dramatic scientific symptoms. The commonest kind, beta cell tumors (or insulinomas) often induce episodes of profound hypoglycemia. Patients with this syndrome additionally develop pituitary and parathyroid tumors as properly as a quantity of cutaneous angiofibromas. Patients with sort 1 diabetes require a number of daily insulin injections, which could be accomplished by hypodermic needle, jet injector, or insulin pump. Companion immunostained sections of islets of the traditional (Left) and kind 1 diabetic (Right) mouse pancreas. They are treated immunofluorescently to localize antibodies to insulin in beta cells (Red) and glucagon in alpha cells (Green). In the conventional islet, beta cells occupy the central region and are the predominant cell type, whereas alpha cells are largely discovered on the periphery. This form of diabetes is caused by an autoimmune destruction of beta cells accompanied by in depth lymphocytic infiltration of islets. Asadi) Companion sections of islets of the normal (Left) and kind 2 diabetic (Right) human pancreas. These fluorescent images present beta cells (Red) and alpha cells (Green) immunolabeled for his or her respective hormones. This powerful software can show how sure diseases such as diabetes have an result on islet cell morphology. Islet cells show a topographic distribution of cell types, with some variation, in islets; whereas beta cells are often in the central core, the opposite cell types are generally seen throughout the islet. During fetal development, some islet cells co-produce insulin and glucagon, but after delivery, each kind of islet cell sometimes secretes a single hormone. Type 1-insulin-dependent diabetes-is attributable to autoimmune destruction of islet beta cells. Lymphocytes (mostly T cells) infiltrate islets; islets later fail to produce insulin and show fibrosis. In sort 2-non�insulindependent diabetes-islets often appear regular but produce inadequate amounts of insulin, and target cell receptors for insulin are irregular. At superior stages, discount in islet cell mass and accumulation of amyloid occur. Individuals with kind 2 could require insulin remedy however are sometimes managed by oral hypoglycemic drugs and life-style modifications. Parts of several tightly packed polyhedral islet cells are close to a fenestrated capillary. A dominant feature of these cells is dense-core secretory vesicles (arrows) whose size and look. Beta cell vesicles within the mouse have an electron-dense homogeneous core surrounded by an electron-lucent space, and bounded externally by a membrane. Numerous hole junctions between beta cells are believed to synchronize oscillations in intracellular Ca2+ during hormone secretion. Islets are innervated by the sympathetic and parasympathetic nervous techniques; adrenergic and cholinergic nerve terminals end instantly on islet cells, which may modulate hormone secretion. The predominant characteristic of their cytoplasm is the various membrane-bound secretory vesicles of assorted sizes and inner density. The protein hormones concerned in regulation of carbohydrate metabolism are insulin, which lowers blood glucose by selling its entry into cells, and glucagon, which raises blood glucose levels. Somatostatin inhibits glucagon and insulin secretion, pancreatic polypeptide inhibits secretion of somatostatin and pancreatic enzymes, and ghrelin stimulates appetite. Most are electron-dense with a pale halo; one appears to be fusing with the plasma membrane prior to exocytosis. It helps elucidate intracellular pathways in synthesis and secretion of insulin and discharge of this peptide hormone by exocytosis into circulation. Distinctive membrane-bound secretory vesicles, which derive from the Golgi complicated, dominate the cytoplasm, normally between the ovoid nucleus of the cell and the plasma membrane, which abuts a fenestrated capillary. Vesicle morphology differs markedly amongst species and amongst different islet cell sorts, however secretory vesicles in human beta cells, about 200-250 nm in diameter, usually have an electron-dense crystalloid composed of an insulin�zinc 10.
Genetically mediated disordered regulation of the innate immune system unifies these syndromes and results in blood pressure medication ed torsemide 20 mg for sale recurrent and stereotypical assaults of fevers and associated symptoms blood pressure up torsemide 20 mg buy cheap. Mevalonate Isoprenylated kinase proteins Inflammasome Cryopyrin Caspase 1 the innate immune system represents the first-line response to immunologic challenges and is composed of cellular defenses (neutrophils hypertension differential diagnosis torsemide 10 mg trusted, dendritic cells, macrophages, and natural killer cells), proinflammatory signaling proteins known as cytokines, and the complement system. Nearly all mutations found within the autoinflammatory syndromes disrupt normal management of inflammatory signaling and lead to era of a proinflammatory state and inflammatory signs. Erysipeloid erythema, an intensely erythematous warm, tender, plaquelike lesion on the lower extremities, can be noted in up to 40% of sufferers. Over time, these recurrent episodes of irritation may lead to amyloidosis of the kidneys or liver. Those sufferers with genotypes resulting in gentle illness have a lower likelihood of growing amyloidosis, and thus prognosis is favorable. Most of those mutations are missense mutations in highly conserved areas of protein resulting in a partial lower in mevalonate kinase exercise. More than 90% of patients will exhibit important cervical lymphadenopathy, and 80% will develop a nonspecific erythematous rash. Oral corticosteroids are effective, however long-term sequelae from these drugs are undesirable. Systemic corticosteroids are additionally efficient but require ever-increasing doses and unacceptable systemic adverse effects. In this condition, patients develop stereotypical assaults on a predictable schedule. Owing to the self-limited nature of the syndrome, treatment is reserved for these sufferers with extreme illness or these sufferers whose condition creates tough socioeconomic circumstances for the household. In patients requiring therapy, one or two doses of systemic prednisone (1 mg/kg) within 6 hours of fever onset is effective in aborting fever in 90% of patients. However, up to 50% of sufferers may expertise an elevated frequency of assaults after therapy with systemic corticosteroids. Without intervention, 40% of sufferers experience a significant reduction in the severity and frequency of fever assaults within 5 years of prognosis. Malignancy and an infection should be considered in all patients; nevertheless, the repetitive and stereotypical nature of the assaults will differentiate the autoinflammatory conditions. The utility of acute section reactant assessment within the diagnostic analysis of sufferers is limited as a outcome of all situations will result in irregular values. Dermatologic manifestations must be examined first hand and imaging for fascial irritation as nicely as full-thickness biopsy thought-about at the time of rash incidence. Gross bony abnormalities should be evaluated with plain radiography, and audiologic testing may be indicated within the diagnostic evaluation of patients with recurrent fevers. Finally, genetic testing is out there commercially for patients with suspected hereditary autoinflammatory syndromes; nonetheless, up to 30% of sufferers with phenotypic manifestations attribute of a given autoinflammatory syndrome have a traditional genetic testing. Genetic testing might ultimately be indicated for proper counseling of reproductive danger. Vasculitis can occur secondary to an underlying disease or trigger or as a half of a primary vasculitic illness. Many types of vasculitis could be organ and life threatening, which makes early prognosis with immediate treatment of critical significance. The prognosis of most forms of vasculitis is often established by the presence of suitable scientific options mixed with histologic and/or arteriographic evidence. These options play a distinguished function in differentiating the vasculitides, which can additionally range broadly with regard to epidemiology, laboratory and imaging features, treatment, and end result. Each vasculitic illness will are inclined to predominantly have an effect on a certain vessel dimension; and though this can be conceptually useful, most forms of vasculitis can affect a various vary of vessels. The focus right here is on polyarteritis nodosa, granulomatosis with polyangiitis (Wegener), microscopic polyangiitis, Churg-Strauss syndrome, and Henoch-Sch�nlein purpura. Biopsies reveal necrotizing irritation of the medium-sized or small arteries with neutrophils, fibrinoid changes, and disruption of the inner elastic lamina. Sinonasal disease occurs in more than 95% of patients and may lead to nasal septal perforation and/or saddle-nose deformity, with 85% growing pulmonary involvement. Glomerulonephritis, which is current in 20% of patients at the time of prognosis but manifests in 80% along the disease course, may be rapidly progressive and result in renal failure. Because renal illness is normally asymptomatic, urine microscopy to search for dysmorphic pink blood cells or pink blood cell casts is crucial in detecting glomerulonephritis. Chest imaging must be performed in all sufferers because up to one third of patients with pulmonary disease could additionally be asymptomatic. Pulmonary radiographic findings can embody single or multiple nodules, infiltrates, or cavities, as well as ground-glass infiltrates that recommend alveolar hemorrhage. The highest constructive yield of greater than 90% comes from surgical biopsies of affected lung, with biopsies of the higher airways being diagnostic less than 20% of the time. Renal histology is that of a focal, segmental, necrotizing, crescentic glomerulonephritis with few to no immune complexes. Cyclophosphamide may either be given orally as 2 mg/ kg/day taken suddenly within the morning or intravenously as 15 mg/kg each 2 weeks for 3 doses and each three weeks thereafter. It has a major side effect profile that includes infection, cytopenia, bladder toxicity, infertility, and myelodysplasia. To prevent leukopenia, blood cell counts must be measured each 1 to 2 weeks for as lengthy as the affected person is taking cyclophosphamide. Cavity in upper lobe of proper lung lined with necrotic materials High-resolution computed tomography sample of a number of, bilateral pulmonary nodules in granulomatosis with polyangiitis (Wegener). Clinical manifestations of granulomatosis with polyangiitis (Wegener) Upper respiratory involvement Ulcerative lesions of nostril, sinuses, mouth, pharynx Granulomatosis irritation. In the absence of side effects, maintenance remedy is given for no less than 2 years, after which era consideration could also be made on an individual basis whether to continue the maintenance agent or to taper remedy to discontinuation. However, relapse happens in 50% to 70% of sufferers and disease-related organ damage is frequent. It is regarded as having three phases: a prodromal part, with allergic rhinitis and bronchial asthma, an eosinophilic part, with peripheral and tissue eosinophilia, and vasculitis of the peripheral nerve (70%-80%), lung (40%-70%, which incorporates eosinophilic, granulomatous and vasculitic lung disease), heart (25%-35%), skin (40%-75%), gastrointestinal tract (30%), or kidney (10%-40%). Although these phases are conceptually useful, they is in all probability not identifiable in all sufferers and they might not occur in sequence. Two thirds of patients report an antecedent upper respiratory tract infection, though no particular inciting organism has been recognized. Gastrointestinal manifestations include colicky belly ache, vomiting, and potentially intussusception. Renal biopsy may have prognostic utility and is an immune complicated glomerulonephritis containing IgA. Glucocorticoids might lower tissue edema, arthritis, and stomach discomfort and decrease the speed of intussusception. Uncontrolled research suggest that glucocorticoids in combination with a cytotoxic agent could additionally be helpful in sufferers with lively glomerulonephritis and progressive renal insufficiency. Relapse happens in up to 40% of cases, usually within the first 3 months after the preliminary episode. Morbidity comes from disease itself, as well as a greater danger of most cancers, infections, heart problems, and osteoporosis. High estrogen ranges have been related to elevated variety of autoreactive B lymphocytes, a predominantly Th2 response, and increased antibody production. Diffuse proliferative kind Glomerulus displaying proliferative change, fibrinoid necrosis and hematoxylin physique (arrow) (H & E) D. Typically, the patient is a young girl with some, or extra, of the next features: a butterfly rash over the face, fever, joint pain and swelling, pleuritic chest ache, and photosensitivity. These patients feel disturbed by brilliant lights, which irritate them and make them feel light-headed and trigger a brief transient rash. A careful history in these patients will elicit a variety of different stress-related symptoms, together with melancholy, anxiousness, and poor sleep. Cutaneous Electron microscopic diagram: large subendothelial deposits of immune complexes Electron microscopic diagram: diffuse subepithelial deposits * All fluorescence slides stained with fluorescein-labeled rabbit antihuman gamma globulin lesions can be additional classified as acute, subacute, and continual lesions. One of probably the most well known features of lupus is the malar or butterfly rash that can last for a quantity of weeks after brief solar publicity. Hair loss happens in most patients with lupus and may contain the scalp, eyebrows, eyelashes, beard, and physique hair. Some develop Jaccoud arthropathy, a reducible arthropathy as a result of capsular laxity, involving the same joints as rheumatoid arthritis.






