Cymbalta
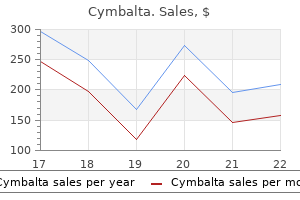
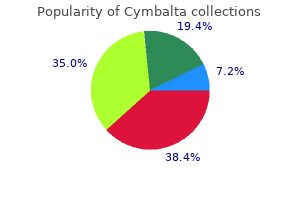
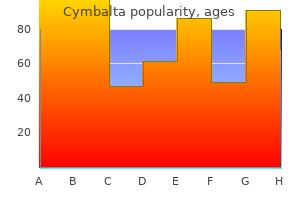
Cymbalta
Cymbalta dosages: 60 mg, 40 mg, 30 mg, 20 mg
Cymbalta packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Therefore solely a small fraction of these probably toxic substances are eradicated from the body by excretion resulting from filtration alone anxiety symptoms while driving 40 mg cymbalta order amex. Thus secretion of organic anions and cations anxiety symptoms nausea cymbalta 40 mg effective, together with many toxins from the peritubular capillary into the tubular fluid anxiety symptoms depression cymbalta 20 mg purchase with visa, promote elimination of these compounds from plasma entering the kidneys. These receptors, called multiligand endocytic receptors, can bind a wide range of peptides and proteins and thereby mediate their endocytosis. Megalin and cubilin mediate protein and peptide endocytosis in the proximal tubule. Both are glycoproteins, with megalin being a member of the low-density lipoprotein receptor gene household. A thorough analysis of urine contains macroscopic, microscopic, and biochemical assessments. This is carried out by visible assessment of the urine, microscopic examination of urinary sediment, and biochemical evaluation of urinary composition utilizing dipstick reagent strips. It is regular to find trace quantities of protein in urine, particularly concentrated urine. Because the mechanism for protein reabsorption is "upstream" of the thick ascending limb. However, proteinuria in larger than trace quantities is often indicative of renal disease. Organic cations, together with xenobiotics such as the antidiabetic agent metformin, the antiviral agent lamivudine, and the anticancer drug oxaliplatin, and plenty of essential monoamine neurotransmitters together with dopamine, epinephrine, histamine, and norepinephrine are secreted by the proximal tubule. Uptake of natural cations is pushed by the magnitude of the cell-negative potential difference throughout the basolateral membrane. These transport mechanisms are nonspecific, and several organic cations usually compete for secretion through a given transport pathway. Similar competitors is observed for natural cation secretion by the proximal tubule, and elevated plasma ranges of 1 transported cation species can inhibit secretion of the other competing cations. For instance, the histamine H2 antagonist cimetidine used to deal with gastric ulcers is secreted via natural cation transport mechanisms within the proximal tubule. If cimetidine is given to sufferers receiving procainamide (a drug used to treat cardiac arrhythmias), cimetidine reduces urinary excretion of procainamide (also an natural cation) by direct competition for a standard secretory pathway. As a consequence, coadministration of cationic medication competing for a similar pathway can improve the plasma focus of each medication to ranges a lot larger than these noticed when the medication are given alone. The optimistic voltage within the lumen performs a major role in driving the passive paracellular reabsorption of cations. Because the apical membrane is conductive primarily to K+, the apical membrane voltage is extra unfavorable than the basolateral membrane voltage, which is conductive to K+ and Cl-, thereby resulting in a lumen optimistic transepithelial potential. Reabsorption of water, but not NaCl, within the descending skinny limb will increase [NaCl] within the tubule fluid entering the ascending skinny limb. As the NaCl-rich fluid strikes towards the cortex, NaCl diffuses out of the tubule lumen throughout the ascending thin limb and into the medullary interstitial fluid, down a concentration gradient directed from the tubule fluid to the interstitium (see Chapter 35 for details). This transporter maintains a low intracellular [Na+], which supplies a positive chemical gradient for the motion of Na+ from tubular fluid into the cell. Using the potential energy launched by the downhill movement of Na+ and Cl-, this symporter drives the uphill movement of K+ into the cell. These K+ channels allow the K+ transported into the cell via the 1Na+/1K+/2Cl- symporter to recycle back into tubule fluid. Because the [K+] in tubule fluid is relatively low, K+ recycling is required for continued operation of the 1Na+/1K+/2Cl- symporter. The operation of the Na+/H+ antiporter in the apical membrane ends in mobile uptake of Na+ in change for H+. The voltage across the thick ascending limb is important for reabsorption of a quantity of cations. The tubular fluid is positively charged relative to blood because of the distinctive location of transport proteins in the apical and basolateral membranes. The importance of the paracellular pathway to solute reabsorption is underscored by the remark that inactivating mutations of the tight junction protein claudin-16 reduce reabsorption of Mg++ and Ca++ by the ascending thick limb, even in the presence of a lumen positive transepithelial voltage. In summary, NaCl reabsorption throughout the thick ascending limb occurs via transcellular and paracellular pathways. A number of proteins have now been identified as parts of the tight junction, together with proteins that span the membrane of one cell and hyperlink to the extracellular portion of the same molecule within the adjacent cell. Of these junctional proteins, claudins seem to be major determinants of the permeability characteristics of tight junctions. Claudin-2 is permeable to water and could additionally be liable for paracellular water reabsorption across the proximal tubule. Claudin-4 has been shown in cultured kidney cells to control the permeability of the tight junction to Na+, whereas claudin-15 determines whether a tight junction is permeable to cations or anions. Thus the permeability traits of the tight junctions in numerous nephron segments are determined no much less than partly by the precise claudins expressed by the cells in that segment. Thus dilution of tubular fluid begins within the thick ascending limb and continues within the early phase of the distal tubule. The final segment of the distal tubule (late distal tubule) and the amassing duct are composed of three cell types: principal cells and two types of intercalated cells. Reabsorption of Na+ generates a adverse luminal voltage across the late distal tubule and amassing duct, which provides the driving force for paracellular reabsorption of Cl-. A variable quantity of water is reabsorbed throughout principal cells within the late distal tubule and accumulating duct. Although the adverse potential inside these cells favors intracellular K+ retention, the electrochemical gradient throughout the apical membrane promotes secretion of K+ from the cell into tubular fluid (see Chapter 36). As a consequence these distal nephron segments possess the flexibility to both secrete and reabsorb K+ through independently regulated mechanisms, which contrasts with the final tendency to reabsorb Na+ along most nephron segments. However, other hormones (including dopamine and adrenomedullin), Starling forces, and the phenomenon of glomerulotubular steadiness also affect NaCl reabsorption. Taken together, these actions enhance Na+ uptake across the apical cell membrane and facilitate Na+ exit from the cell interior into blood. The increase in reabsorption of Na+ generates a unfavorable transepithelial luminal voltage across the late distal tubule and the amassing duct. This negative voltage within the lumen offers the electrochemical driving drive for reabsorption of Cl- throughout the tight junctions. Aldosterone secretion is decreased by hypokalemia and natriuretic peptides (discussed in more detail next). Through its stimulation of NaCl reabsorption in the amassing duct, aldosterone additionally indirectly will increase water reabsorption by this nephron section. As noted earlier, aldosterone stimulates each NaCl reabsorption and K+ secretion by the collecting duct. By distinction, throughout hyperkalemia, K+ excretion by the kidneys is increased to normalize plasma [K+], albeit without an accompanying change in NaCl excretion. This phenomenon-the obvious unbiased effects of aldosterone on urinary Na+ and K+ excretion-is known as the aldosterone paradox. It inhibits NaCl and water reabsorption across the medullary portion of the amassing duct. Uroguanylin and guanylin are produced by neuroendocrine cells in the intestine in response to oral ingestion of NaCl. Studies in Sgk1 knockout mice reveal that this kinase is required for animals to survive extreme NaCl restriction and K+ loading. NaCl restriction and K+ loading enhance plasma [aldosterone], which quickly (in minutes) will increase Sgk1 protein expression and phosphorylation. These mutations increase the variety of Na+ channels in the apical cell membrane of principal cells and thereby the quantity of Na+ reabsorbed. The cause of the autosomal dominant kind is an inactivating mutation within the mineralocorticoid receptor. First, NaCl and water reabsorption by the nephron (especially the proximal tubule) falls. Second, aldosterone secretion decreases, thus decreasing NaCl reabsorption within the thick ascending limb, distal tubule, and amassing duct. Third, as a end result of angiotensin is a potent vasoconstrictor, a reduction in its focus permits the systemic arterioles to dilate and thereby lower arterial blood pressure. The involvement of these gut-derived hormones helps explain why the natriuretic response of the kidneys to an oral NaCl load is extra pronounced than when delivered intravenously. Catecholamines released from the sympathetic nerves (norepinephrine) and the adrenal medulla (epinephrine) stimulate reabsorption of NaCl and water by the proximal tubule, thick ascending limb of the loop of Henle, distal tubule, and accumulating duct.
An astute clinician will usually attempt to anxiety 025 30 mg cymbalta purchase mastercard biopsy a well-developed however "contemporary" lesion that demonstrates the expected main pathology anxiety symptoms jaw cymbalta 20 mg order fast delivery, freed from secondary adjustments similar to erosions anxiety symptoms weak legs cymbalta 40 mg order mastercard, excoriations, and lichenification. This allows the dermatopathologist to consider the histologic features of the lesions in their native state, with out potentially confounding alterations. Lastly, the skin is a three-dimensional structure, and just like the cartographers who construct maps, there are particular descriptors used by dermatologists to describe the topography of particular person pores and skin lesions. Examples include flat-topped (lichenoid), dome-shaped, verrucous, umbilicated, filiform, and pedunculated3. Palpation and appreciation of textural adjustments Any discussion of morphology must embody textural change, and palpating a lesion typically provides necessary diagnostic clues. Firstly, it helps in making a distinction amongst major morphologies (see Table zero. Secondly, palpation might augment the examination and appreciation of a illness process for which visible modifications are absent, unimpressive, or nonspecific. For example, in morphea, an autoimmune connective tissue disease that results in sclerotic collagen inside the dermis, the skin feels indurated (very firm) whereas solely nonspecific hyperpigmentation may be evident with visual inspection. The identical is true for other fibrotic disease processes, similar to nephrogenic systemic fibrosis and systemic sclerosis. Lastly, purpura is often categorised as palpable or non-palpable, and this division implies different underlying etiologies. Examples of useful distinctions that can be gleaned through palpation are outlined in Table zero. Color the color of skin lesions can provide necessary clues as to the nature of the illness course of. For instance, whereas many dermatological processes appear red�purple in shade, you will need to verify whether this can be a blanchable erythema. Yet even inside racial and ethnic teams, gradations exist with regard to skin pigmentation. Sometimes the time period "pores and skin of color" is used to describe all pores and skin tones darker than those of white (Caucasian) skin4. It also refers to different shared characteristics, corresponding to hair colour, hair texture, and a tendency toward certain response patterns in the pores and skin as a response to an insult. The practice of dermatology requires a solid understanding of the variations in medical features. Variations in skin color are because of differences in the amount and distribution of melanin inside epidermal melanocytes and keratinocytes5, rather than the variety of melanocytes (see Ch. In addition, the ratio of eumelanin (brown�black) to pheomelanin (yellow�red) influences skin color, with pheomelanin the predominant pigment in those with freckles and purple hair. Exposure to ultraviolet radiation additionally considerably impacts melanin manufacturing (tanning). Pigmentation of the skin clearly influences the prevalence of certain cutaneous findings and issues. For example, individuals with darkly pigmented skin usually tend to develop multiple streaks of longitudinal melanonychia (see Ch. Whether postinflammatory hypopigmentation10 is more common or simply extra clinically obvious is a matter of debate. For example, the stratum corneum of black skin often retains extra layers and is extra compact and cohesive than that of white pores and skin. In addition, darker skin produces much less vitamin D3 in response to equal amounts of sunlight, and this is postulated to have been a driving force in the evolution of paler skin as early people migrated away from the equator11. Perhaps the most important level to keep in mind is that erythema (redness) could be tough to respect in darkly pigmented skin. Erythema is caused by vasodilation and/or elevated blood circulate throughout the dermis, and if the epidermis is deeply pigmented, the red hues of oxyhemoglobin are often less apparent. Diagnostic procedures that rely upon the event of erythema, such as patch testing for the evaluation of allergic contact dermatitis, can be tougher to interpret in dark skin. Lastly, cyanosis (blue hues indicative of poor oxygenation and a important scientific sign) can also be tougher to recognize when the skin is darkly pigmented. Configuration and Distribution After carefully contemplating the morphology and color of pores and skin lesions, the dermatologist must subsequent analyze two closely associated properties � configuration and distribution � so as to hone in on the proper prognosis. Configuration Appreciation of the configuration or arrangement of skin lesions can present important clues as to the prognosis. Addisondisease, hemochromatosis) � Pityriasisrubrapilaris Mycosisfungoides(sometimes) Pityriasisrubrapilaris withislandsofsparing Yellow Solarelastosis Carotenoderma � Xanthomas. In addition to these two patterns, a linear arrangement may result from a traumainduced Koebner phenomenon (an isomorphic response [Table 0. Linear lesions are regularly seen in acute allergic contact dermatitis as a result of crops. The long axis of oval lesions of pityriasis rosea18 and erythema dyschromicum perstans follows these cleavage strains, and this pattern is most obvious on the posterior trunk. A seborrheic distribution pattern contains the head and neck as well as the higher trunk, and it reflects areas wealthy in sebaceous glands; seborrheic dermatitis, acne vulgaris, and pityriasis versicolor are dermatoses that favor these websites. The time period "photodistribution" describes lesions which may be accentuated in areas exposed to ultraviolet irradiation, and photodermatoses embody polymorphic gentle eruption, phototoxic drug reactions. Of note, sometimes a disorder will display a mixture of distribution patterns; for instance, in dermatomyositis, lesions could be each photodistributed and involve extensor surfaces. In addition to differences in the shade of inflammatory lesions, individuals with darkly pigmented pores and skin also have an elevated frequency of a quantity of cutaneous disorders (see part on Color) and certain forms of reaction and distribution patterns19. Examples of those response patterns include papular eczema and a follicular accentuation of atopic dermatitis and pityriasis versicolor, in addition to an annular configuration of seborrheic dermatitis and facial secondary syphilis. An instance of a well-liked distribution sample is inverse pityriasis rosea by which lesions occur primarily in the axillae and groin rather than on the trunk. Sometimes the distribution is greatest defined by the phenomenon of locus minoris resistentiae by which certain anatomic sites are extra susceptible than others to a particular disease process20. Examples could be cutaneous infections within a lymphedematous limb and asteatotic eczema within a pores and skin graft web site. It is most commonly used to assist in the diagnosis of pigmentary issues and infectious ailments (Table 0. Temporal Course Central to any medical historical past, including that of cutaneous issues, is the temporal course. The affected person ought to be queried as to duration and relative change in intensity or distribution over time. For instance, there are some dermatoses that have a cephalocaudal progression over time, such as measles and pityriasis rubra pilaris. Of course, the time course is extra extended within the latter as in comparability with the former. With experience, Distribution Stepping again and observing the anatomic distribution pattern of pores and skin lesions can even show very useful. Examples of useful indicators include scale (not to be confused with crusts), which frequently reflects parakeratosis that requires 2 weeks to develop, and intact tense bullae, which are rarely more than every week old. Therefore, if lichenification is present, the lesion has not appeared acutely, regardless of what the patient could imagine. In an otherwise typically wholesome patient, there are a number of ailments whose cutaneous manifestations are often acute in nature, particularly urticaria, morbilliform drug eruption, viral exanthem, acute allergic or irritant contact dermatitis, and pityriasis rosea. This is to not point out that these diseases essentially require quick or emergent administration, however quite that they present to the dermatologist abruptly and are distinguished, notably from neoplasms or chronic dermatoses, by their temporal acuity. Of notice, sometimes a extra severe and doubtlessly life-threatening cutaneous disease could present with skin findings that may mimic a extra frequent and less serious dysfunction, especially early on. Finally, although emergencies are unusual in dermatology, there are a number of sicknesses, significantly those who present with a rash and fever, which are true emergencies and must be recognized promptly and treated appropriately. Examples embrace Stevens�Johnson syndrome, poisonous epidermal necrolysis, Kawasaki disease, meningococcemia (including purpura fulminans), Rocky Mountain spotted fever, necrotizing fasciitis, and endocarditis with cutaneous manifestations. The next two sections of this introductory chapter focus on the essential rules of dermatopathology and dermoscopy, respectively, and you will need to keep in mind that all the diagnostic strategies (unaided scientific examination, histological examination, dermatoscopic examination) discussed herein are complementary. In different phrases, synergistic energy and clinicopathologic correlation are achieved when the techniques are utilized in combination. As a corollary, using anyone approach, to the exclusion of the others, may be misleading and probably lead to misdiagnosis.
Therefore anxiety zig ziglar purchase cymbalta 20 mg line, to plot a vascular function curve in the standard method anxiety scale purchase 20 mg cymbalta mastercard, Pv ought to be scaled alongside the y-axis and cardiac output along the x-axis symptoms 0f anxiety cymbalta 30 mg order on-line. To plot the cardiac and vascular perform curves on the same set of axes requires a modification of the plotting convention for certainly one of these curves. The convention for the vascular operate curve is violated arbitrarily in this chapter. When the cardiovascular system is represented by a given pair of cardiac and vascular operate curves, the intersection of these two curves defines the equilibrium point of that system. Only transient deviations from such values of cardiac output and Pv are possible, so lengthy as the given cardiac and vascular perform curves characterize the system accurately. The tendency to operate about this equilibrium level might greatest be illustrated by the response to a sudden change. This change in Pv may be brought on by the fast injection, during ventricular diastole, of a given volume of blood on the venous vessels of the circuit and simultaneous withdrawal of an equal quantity from the arterial vessels of the circuit. The increased cardiac output would then trigger the switch of a web quantity of blood from the veins to the arteries of the circuit, with a consequent discount in Pv. In one heartbeat, the reduction in Pv could be small (from level B to point C) as a outcome of the guts would switch solely a fraction of the whole venous blood volume to the arteries. As a results of this discount in Pv, cardiac output during the very next beat diminishes (from level C to level D) by an amount dictated by the cardiac perform curve. Because point C is still above the intersection level, the guts pumps blood from the veins to the arteries at a fee higher than that at which blood flows across the peripheral resistance from arteries to veins. Only one specific combination of cardiac output and venous pressure-the equilibrium point, denoted by the coordinates of the point at which the curves intersect-satisfies the necessities of the cardiac and vascular perform curves concurrently. At the equilibrium point, cardiac output equals venous return, and the system is stable. Myocardial Contractility Combinations of cardiac and vascular perform curves additionally help explain the effects of alterations in ventricular contractility on cardiac output and Pv. When the consequences of such neural stimulation are restricted to the heart, the vascular function curve is unaffected. Cardiac sympathetic nerve stimulation abruptly raises cardiac output to point B because of the improved myocardial contractility. However, this excessive cardiac output causes a rise within the web transfer of blood from the veins to the arteries of the circuit, and as a consequence, Pv subsequently begins to fall (to level C). However, cardiac output remains to be sufficiently high to impact the net transfer of blood from the veins to the arteries of the circuit. Thus both Pv and cardiac output proceed to fall gradually till a new equilibrium point (point D) is reached. This equilibrium point is positioned on the intersection of the vascular operate curve and the model new cardiac operate curve. The biological response to enhancement of myocardial contractility is mimicked by the hypothetical change predicted by the model on this chapter. During neural stimulation, cardiac output (aortic flow) rises rapidly to a peak value after which falls progressively to a steady-state worth considerably larger than the control degree. The improve in aortic flow is accompanied by reductions in proper and left atrial pressures. Mechanistically, the change in ventricular filling stress (Pv) evoked by a given change in blood quantity alters cardiac output by changing the sensitivity of the contractile proteins to the prevailing concentration of intracellular Ca++ (see Chapter 18). For causes explained earlier, pure increases or decreases in venomotor tone elicit responses that are like those evoked by will increase or decreases, respectively, in total blood quantity. Peripheral Resistance Analysis of the effects of adjustments in peripheral resistance on cardiac output and Pv is complex as a outcome of both the cardiac and vascular perform curves shift. The direction of rotation differs as a end result of the axes for the vascular perform curves have been switched in these two figures, as explained earlier. Whether level B falls immediately beneath point A or lies barely to the best or left of it depends on the magnitude of the shift in every curve. The series arrangement requires that the move pumped by the two ventricles be nearly equal to one another over any substantial period; otherwise, all the blood would in the end accumulate in a single or the other of the vascular methods. A More Complete Theoretical Model: the Two-Pump System the preceding discussion shows that the interrelationships between cardiac output and Pv are advanced, even in an oversimplified circulation model that includes just one pump and simply the systemic circulation. In reality, the cardiovascular system includes the systemic and pulmonary circulations and two pumps: the left and proper ventricles. Thus the interrelationships amongst ventricular output, arterial stress, and atrial strain are far more complicated. To higher understand the relationships between the two ventricles and the two vascular beds, the proper ventricular operate is examined in more detail as follows. Normally, pulmonary vascular resistance is approximately 10% as great as systemic vascular resistance. Because the 2 resistances are in collection with one another, complete resistance can be 10% greater than systemic resistance alone (see Chapter 17). In a standard cardiovascular system, a 10% increase in systemic vascular resistance would enhance Pa (and hence left ventricular afterload) by roughly 10%. Under certain circumstances, nonetheless, this enhance in Pa may considerably alter the function of the cardiovascular system. If the 10% enhance in whole resistance is achieved by including a small degree of resistance. In the mannequin, the right and left ventricles generate cardiac outputs that vary directly with their respective filling pressures. Under control situations (when the best ventricle is functioning normally), the outputs of the left and proper ventricles are equal (5 L/ minute). The proper ventricular pumping action causes the strain within the pulmonary artery (not shown) to exceed the stress in the pulmonary veins (Ppv) by an quantity that forces fluid via the pulmonary vascular resistance at a fee of 5 L/minute. When the best ventricle ceases to transfer blood actively from the systemic veins to the pulmonary arteries, pulmonary arterial pressure (Ppa) decreases rapidly (not shown) and systemic venous pressure (Psv) rises quickly to a typical value (5 mm Hg). At this low stress, nevertheless, fluid flows from the pulmonary arteries to the pulmonary veins at a significantly reduced price. At the beginning of right ventricular arrest, the left ventricle is pumping fluid from the pulmonary veins to the systemic arteries at the control fee of 5 L/minute, which greatly exceeds the rate at which blood returns to the pulmonary veins as soon as the right ventricle ceases to function. Because pulmonary venous strain is the preload for the left ventricle, left ventricular (cardiac) output drops abruptly as well and attains a steady-state value of approximately 2. This effect in turn results in a rapid discount in systemic arterial strain (Psa). If fluid is added until pulmonary venous strain (left ventricular preload) is raised to its management value, cardiac output and systemic arterial stress are restored almost to regular, however systemic venous pressure is abnormally elevated. If left ventricular function is normal, adding a traditional left ventricular preload evokes regular left ventricular output. Hence, systemic venous pressure (Psv) must exceed pulmonary venous stress (Ppv) by this quantity. With this information, the principal function of the best ventricle could also be characterized as as follows. From the viewpoint of offering sufficient circulate of blood to all tissues within the body, the left ventricle alone can carry out this perform. The crucial operate of the right ventricle is to prevent the rise in systemic venous (and pulmonary arterial) strain that may be required to pressure the conventional cardiac output through the pulmonary vascular resistance. A regular proper ventricle, by preventing an abnormal rise in systemic venous pressure, prevents the development of intensive edema in dependent regions of the physique. Analysis of the control of cardiac output has so far been restricted to the control of stroke volume, and the function of coronary heart rate has not been considered. A rise in heart price would increase the online influx of Ca++ per minute into myocardial cells (see additionally Chapter 18), and this inflow would enhance myocardial contractility. The decrease in stroke quantity is caused by the lowered time for ventricular filling. For instance, as pacing frequency is increased from 50 to a hundred beats/minute, the rise in coronary heart price augments Qh. Hence, as pacing frequency is elevated, the lower in stroke volume have to be approximately equal to the increase in heart rate. In addition, generalized vascular autoregulation tends to keep tissue blood flow constant (see additionally Chapter 17). This adaptation results in changes in preload and afterload that additionally keep cardiac output almost constant. Therefore, the induced decrease in stroke volume should have exceeded the increase in coronary heart rate at this excessive vary of pacing frequencies. Although the connection of cardiac output to heart price is characteristically that of an inverted U within the common inhabitants, the relationship varies quantitatively amongst topics and amongst physiological states.
These fibers decussate in the midbrain anxiety and depression purchase cymbalta 60 mg amex, descend via the pons and medulla anxiety 8 months pregnant buy generic cymbalta 30 mg line, and then take up a position just ventral to the lateral corticospinal tract in the spinal wire anxiety symptoms guilt buy cymbalta 60 mg otc. They preferentially have an result on motor neurons controlling distal musculature, as do the corticospinal fibers. Red nucleus neurons receive enter from the cerebellum and from the motor cortex; thus making this an space of integration of exercise from these two motor systems. The Medial System the ventral corticospinal tract and much of the corticobulbar tract can be thought to be medial system pathways. These tracts end on the medial group of interneurons within the spinal twine and on equivalent neurons within the brainstem. These muscle tissue often contract bilaterally to provide postural help or some other bilateral operate, similar to swallowing or wrinkling of the brow. These embrace the pontine and medullary reticulospinal tracts, the lateral and medial vestibulospinal tracts, and the tectospinal tract. The Tectospinal Tract the tectospinal tract originates within the deep layers of the superior colliculus. The axons cross to the contralateral aspect, slightly below the periaqueductal grey matter. They then descend in the ventral funiculus of the spinal twine to terminate on the medial group of interneurons in the upper cervical spinal twine. The tectospinal tract regulates head motion in response to visual, auditory, and somatic stimuli. Monoaminergic Pathways In addition to the lateral and medial techniques, much less particularly organized methods descend from the brainstem to the spinal twine. These embrace a quantity of pathways by which monoamines function synaptic transmitters. With regard to motor operate, the ventral horn projection could enhance motor activity. In general, the monoaminergic pathways act to alter the responsiveness of spinal cord circuits, including the reflex arcs. In this manner, they induce widespread adjustments in excitability quite than discrete movements or specific adjustments in conduct. Motor Deficits Caused by Lesions of Descending Motor Pathways A widespread reason for motor impairment in people is interruption of the cerebral cortical efferent fibers in the internal capsule; such interruptions happen in capsular strokes. The ensuing dysfunction is usually termed a pyramidal tract syndrome, or higher motor neuron illness, though these names are misnomers. Motor adjustments attribute of this disorder embody (1) increased phasic and tonic stretch reflexes (spasticity); (2) weak spot, usually of the distal muscular tissues, particularly the finger muscle tissue; (3) pathological reflexes, together with the sign of Babinski (dorsiflexion of the large toe and fanning of the opposite toes when the only of the foot is stroked); and (4) a reduction in superficial reflexes, such because the belly and cremasteric reflexes. Of significance is that if solely the corticospinal tract is interrupted, as can happen with a lesion of the medullary pyramid, most of those indicators are a lot reduced or absent. In this situation, probably the most distinguished deficits are weakness of the distal muscle tissue, particularly those of the fingers, and a Babinski sign. Evidently, the presence of spasticity requires the disordered function of different pathways, such because the reticulospinal tracts, as would occur after loss of the descending cortical influence to the brainstem nuclei of origin of these tracts. The results of interruption of the medial system pathways are quite different from those produced by corticospinal tract lesions. The primary deficits related to medial system interruption are an preliminary reduction within the tone of postural muscles and loss of righting reflexes. With the intercollicular transection, some descending pathways, corresponding to those originating in the cerebral cortex, are interrupted, whereas others, corresponding to these originating within the brainstem, remain intact. However, do not forget that the corticospinal tract is just one part of the cortical descending fibers. Many different cortical fibers project to places throughout the brainstem, together with the nuclei of origin for the medial descending pathways. Loss of those cortical management techniques results in altered activity within the intact descending pathways. As a outcome, affected animals show hypertonia and suppression of some spinal reflexes, such because the flexion reflex, and exaggeration of others, such because the stretch reflex; this condition is called decerebrate rigidity. Human sufferers with brainstem injury may develop a decerebrate state that has most of the same reflex options as animal preparations. Loss of descending management on the reticular formation leads to increased activity in the pontine reticulospinal pathway and decreased activity within the medullary reticulospinal pathway. Such enhance and decrease in exercise, respectively, produces elevated excitation and decreased inhibition (disinhibition) of the motor neurons, which explains the noticed rigidity. Interestingly, this hypertonia can be relieved by slicing the dorsal roots, which indicates that the reticulospinal tracts have a serious effect on motor neurons. When vessel occlusion is used to generate the decerebrate state, the lateral vestibulospinal tract turns into hyperactive due to harm to Purkinje cells within the anterior vermis of the cerebellum, which offer the most important inhibitory projection to the lateral vestibular nucleus. This hypertonia is actually not misplaced after transection of the dorsal roots, which implies that the lateral vestibulospinal tract is appearing to a big extent immediately on motor neurons (either monosynaptically or through interneurons). The Decerebrate Preparation the decerebrate preparation has been helpful for experimentally investigating how numerous descending pathways interact with the spinal cord circuitry. Surgical decerebration is achieved both by transection of the midbrain, usually at an intercollicular level, or by occlusion of the blood vessels feeding this area. In the latter case, a lesion additionally occurs within the anterior vermis of the cerebellum, an important distinction. Brainstem Control of Posture and Movement the significance of motor management pathways that originate within the brainstem is evident from observations of the extensor hypertonus and increased phasic stretch reflexes that happen in decerebrate animals. Particular brainstem systems have been recognized as influencing posture and locomotion. Brainstem circuits are additionally critically concerned in the management of eye motion; these circuits are discussed in a separate part on the end of the chapter. There are three kinds of postural reflexes: vestibular reflexes, tonic neck reflexes, and righting reflexes. The sensory receptors answerable for these reflexes embody the vestibular apparatus (see Chapter 8), which is stimulated by head movement, and stretch receptors within the neck. Rotation of the top activates sensory receptors of the semicircular canals (see Chapter 8). In addition to producing eye motion, the sensory enter to the vestibular nuclei ends in postural changes. Such changes are mediated by instructions transmitted to the spinal cord through the lateral and medial vestibulospinal tracts and the reticulospinal tracts. The lateral vestibulospinal tract activates extensor muscles that assist posture. For instance, if the head is rotated to the left, postural assist is increased on the left side. This increased help prevents the particular person from falling to the left as the pinnacle rotation continues. A person who has any disease that eliminates labyrinthine function within the left ear tends to fall to the left. Conversely, a person with a disease that irritates (stimulates) the left labyrinth tends to fall to the right. The medial vestibulospinal tract causes contractions of neck muscles that oppose the induced movement (vestibulocollic reflex). Tilting the top additionally changes the linear acceleration on individual hair cells of the otolith organs of the vestibular equipment. The resulting modifications in hair cell activity can produce eye movement and postural adjustment. Conversely, if the quadruped tilts the head and body backward (without bending the neck), the forelimbs flex and the hind limbs extend. If an animal, such as a cat, is dropped, stimulation of the utricles results in extension of the forelimbs in preparation for landing. These muscle tissue contain the biggest focus of muscle spindles of any muscle in the body. If the neck is bent (without tilting of the head), the neck muscle spindles evoke tonic neck reflexes without interference from the vestibular system. Furthermore, if the neck is bent to the left, the extensor muscles in the limbs on the left contract more, and the flexor muscles within the limbs on the best side loosen up. These reflexes are probably to restore an altered place of the top and physique toward regular. The receptors answerable for righting reflexes embrace the vestibular apparatus, the neck stretch receptors, and mechanoreceptors of the physique wall. Brainstem Control of Locomotion the spinal twine contains neural circuits that serve as central sample turbines for locomotion, as mentioned earlier.
NaCl secretion or reabsorption temporarily establishes an osmotic gradient across the pseudostratified epithelium anxiety disorder key symptoms purchase 30 mg cymbalta with mastercard, which supplies the driving force for passive water movement anxiety hot flashes purchase cymbalta 20 mg free shipping. I n addition to their primary operate of gas change anxiety symptoms concentration cymbalta 30 mg buy without prescription, the lungs act as a primary barrier between the outside world and the inside of the body, with host protection features. They are also active organs within the metabolism of xenobiotic and endogenous compounds. Host Defense To cope with the inhalation of foreign substances, the respiratory system and, specifically, the conducting airways have developed distinctive structural options: the mucociliary clearance system and specialised adaptive and innate immune response mechanisms. Mucus Layer the mucus layer lies on prime of the periciliary fluid layer and consists of a posh mixture of macromolecules and electrolytes. Because the mucus layer is in direct contact with air, it entraps inhaled substances, including pathogens. The mucus layer is predominantly water (95% to 97%), 5 to 10 �m thick and exists as a discontinuous blanket. Mucus has low viscosity and high elasticity and is composed of glycoproteins with groups of oligosaccharides attached to a protein backbone. Healthy Mucociliary Clearance System the mucociliary clearance system protects the conducting airways by trapping and removing inhaled pathogenic viruses and micro organism, in addition to unhazardous and toxic particulates. Four cell sorts contribute to the quantity and composition of the mucus layer: goblet cells and Clara cells throughout the tracheobronchial epithelium, and mucous cells and serous cells throughout the tracheobronchial submucosal glands. Goblet cells, additionally referred to as surface secretory cells, represent approximately 15% to 20% of the tracheobronchial epithelium, and are found within the tracheobronchial tree as a lot as the 12th division. In many respiratory ailments, goblet cells appear additional down the tracheobronchial tree; thus the smaller airways are more susceptible to obstruction by mucus plugging. Goblet cells secrete impartial and acidic glycoproteins rich in sialic acid in response to chemical stimuli. In the presence of an infection or cigarette smoke or in sufferers with persistent bronchitis, goblet cells can increase in size and number, prolong above the 12th division of the tracheobronchial tree, and secrete copious quantities of mucus. Injury and infection increase the viscosity of the mucus secreted by goblet cells, which reduces mucociliary clearance of inhaled particles and pathogens. Although each mucous and serous cells secret mucus, their cellular construction and mucus composition are distinctly completely different (Table 26. In a number of lung ailments, including persistent bronchitis, the number and measurement of submucosal glands are increased, which leads to increases in mucus manufacturing, alterations in chemical composition of mucus. Mucus secretion from submucosal tracheobronchial glands is stimulated by parasympathetic (cholinergic) compounds such as acetylcholine and substance P and inhibited by sympathetic (adrenergic) compounds corresponding to norepinephrine and vasoactive intestinal polypeptide. Local inflammatory mediators similar to histamine and arachidonic acid metabolites additionally stimulate mucus manufacturing. Clara cells, situated within the epithelium of bronchioles, additionally contribute to the composition of mucus by way of secretion of a nonmucinous materials containing carbohydrates and proteins. These cells preserve the level of the periciliary fluid by which cilia and the mucociliary transport system operate. Mucus and inhaled particles are faraway from the airways by the rhythmic beating of the cilia. There are roughly 250 cilia per airway epithelial cell, and each is 2 to 5 �m in length. Cilia are composed of nine microtubular doublets that surround two central microtubules held together by dynein arms, nexin links, and spokes. Cilia beat with a coordinated oscillation in a characteristic, biphasic, and wave-like rhythm referred to as metachronism. They beat at roughly 1000 strokes per minute, with an influence ahead stroke and a slow return or restoration stroke. During their power forward stroke, the ideas of the cilia prolong upward into the viscous mucus layer and thereby transfer it and the entrapped particles. On the reverse beat, the cilia launch the mucus and withdraw utterly into the sol layer. The 4 major mechanisms for deposition are impaction, sedimentation, interception, and brownian motion. Particle traits and properties, which influence the mechanism of deposition, are listed in Table 26. Although most alveolar macrophages are adjoining to the epithelium of the alveolus, some are located within the terminal airways and interstitial area. In basic, the longer an inhaled materials remains in the airways, the larger is the likelihood that the material will cause lung damage. The comparatively gradual rate of particle clearance on this space, which is mediated by macrophages, renders it the most common location for a lot of occupational lung ailments. Mucosal Immune System: Adaptive and Innate Immunity Mucosal Immune System In nonmucosal tissues. These innate and distinctive adaptive responses can forestall or restrict responses to foreign nonpathological brokers while eliminating pathological agents/substances with little or no irritation. In addition, if this front-line defense system fails or is bypassed, the lungs do have a classical adaptive immune response system during which lymphatic drainage is by way of the mediastinal lymph node positioned within the upper region of the thoracic cavity adjacent to the primary left-right lung bifurcation. A distinctive feature of the mucosal immune system is that antigens are processed via lymphoid aggregates rather than via a true lymph node. Unlike a real lymph node, which has afferent and efferent lymph move, lymphoid aggregates have only afferent drainage of material into the aggregate without efferent flow. This may function a defense mechanism in limiting sensitization only to mucosal tissue. Another distinguished function is a diffuse submucosal and intraepithelial community of solitary lymphocytes and innate lymphoid cells scattered all through the respiratory tract. A,SecretoryIgAconsists of a minimum of two IgA molecules which would possibly be covalently linked via J chain and covalently associated with the secretorycomponent. The poly-Ig receptor aids in the pinocytosis of IgA into the epithelial cell and its eventual secretion into the airway lumen. During exocytosis of the IgA advanced, the poly-Ig is enzymatically cleaved, and a portion of it, the secretory piece, remains related to the complicated. The secretory piece stays connected to the IgA advanced within the airway and helps defend it from proteolytic cleavage. The IgA-antibody system could be very effective in binding particulates and viruses to type a large complicated, which promotes its removal via the mucociliary clearance system, earlier than they invade epithelial cells. Since most inhaled substances are nonpathogenic, the body has developed a specialized recognition system to determine harmful pathogenic substances and organisms. The quick response, and the shortage thereof for innocuous substances, are extremely advantageous within the mucosal tissues, that are common sites for parasitic invasion and poisonous chemical publicity. The alveolar macrophage additionally transports engulfed particles to ciliated areas of the mucociliary transport system for elimination and thus provides an essential link between the alveolar spaces, the postterminal bronchiole "Achilles heel" area, and the mucociliary clearance system. M-1 macrophages are additionally positioned in submucosal websites and characterize the classical "proinflammatory" phagocytic cell, with comparable killing capabilities as these of alveolar macrophages. The capability of these macrophage populations to show plasticity and eliminate overseas material quickly with either a proinflammatory or regulatory response significantly enhances the lung defense system and is a unique contributor to the general mucosal defense system. They are usually in a resting immature state during which they perform as sentinels to seize and process antigen, after which they mature and migrate to the native draining lymph node (mediastinal node for the lungs). Alveolar macrophages are found mostly in the alveolus adjoining to the epithelium and fewer frequently in the terminal airways and interstitial space. They migrate freely all through the alveolar areas and function a first line of defense within the terminal bronchioles and alveoli. They phagocytize international particles and substances, as well as surfactant and mobile debris from lifeless cells. The mechanism of killing is thru the discharge of granular enzymes (granzymes, perforins, and serine esterases), which create holes or pores throughout the goal cell membranes and thereby cause cell dying. These forms of cells are thought to be hyperlinks between innate and adaptive immunity. A critical side of the link is that these cells can reply should faster than cells of the classical adaptive immune response, limiting early damage till the adaptive response can mobilize a stronger defense. Histatins are present mainly in the oral cavity and are extra specific for pathogenic fungi.
Dang Gui (Angelica root) (Angelica). Cymbalta.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96304
Skin blood vessels dilate immediately and reflexively in response to warmth anxiety symptoms psychology buy generic cymbalta 40 mg line, and they constrict instantly and reflexively in response to chilly anxiety jitters purchase 60 mg cymbalta amex. Blood circulate in skeletal muscle is regulated centrally by sympathetic nerves and domestically by the release of vasodilator metabolites anxiety symptoms on one side of body buy 40 mg cymbalta free shipping. The elevated regional cerebral activity produced by stimuli such as touch, ache, hand motion, speaking, studying, reasoning, and drawback solving are associated with enhanced blood move within the activated area of the contralateral cerebral cortex. The neurovascular unit (microcirculation, pericytes, the extracellular matrix, astrocytes and neurons), a element of the blood-brain barrier, is believed to link brain activity with increased blood move and oxygenation. The microcirculation in intestinal villi constitutes a countercurrent exchange system for O2. Because of the presence of this countercurrent trade system, the villi are in jeopardy in states of low blood move. The splanchnic resistance and capacitance vessels are very aware of adjustments in sympathetic neural activity. The liver receives approximately 25% of cardiac output; roughly three fourths of this output is from the portal vein and roughly a fourth from the hepatic artery. When flow is diminished in both the portal or hepatic system, flow in the other system normally will increase, however not proportionately. The liver tends to maintain constant O2 consumption, partially as a result of its mechanism for extracting O2 from blood is so efficient. In the fetus, a big share of right atrial blood passes via the foramen ovale to the left atrium, and a big share of pulmonary arterial blood passes via the ductus arteriosus to the aorta. At start, the umbilical vessels, ductus venosus, and ductus arteriosus close by contraction of their muscle layers. The reduction in pulmonary vascular resistance caused by lung inflation is the main factor that reverses the strain gradient between the atria and thereby causes the foramen ovale to shut. Effects of disturbed circulate on vascular endothelium: pathophysiological basis and medical views. Endothelium-derived hyperpolarization elements and related pathways: a synopsis. Paradoxical vasoconstriction induced by acetylcholine in atherosclerotic coronary arteries. How do the parasympathetic and sympathetic nervous techniques regulate the features of heart and vasculature What components affect the differential sympathetic regulation of resistance and capacitance vessels How does the baroreceptor-mediated reflex mimic the operation of skeletal muscle proprioceptor reflex What are the 2 main mechanisms, intrinsic to coronary heart muscle, that regulate myocardial performance What is the myogenic mechanism of vascular easy muscle, and how does it participate in regulation of tissue blood flow What are the humoral factors that participate in regulation of blood move, and what are their actions All of these determinants are interdependent, inasmuch as a change in one determinant of cardiac output virtually invariably alters another. Nervous Control of the Heart Rate Although sure local components, corresponding to temperature changes and stretching of tissue, can affect the heart rate, the autonomic nervous system is the principal means by which the heart rate is controlled. It may enhance throughout emotional excitement, and during muscular train, it may improve to rates properly above one hundred fifty beats per minute. In well-trained athletes, the similar old resting rate is just approximately 50 beats per minute. The sympathetic nervous system enhances automaticity, whereas the parasympathetic nervous system inhibits it. Changes in coronary heart price usually involve a reciprocal action of these two divisions of the autonomic nervous system. Thus the guts fee ordinarily will increase with a mixed lower in parasympathetic exercise and enhance in sympathetic exercise; the heart fee decreases with the opposite adjustments in autonomic neural exercise. When a resting individual is given atropine, a muscarinic receptor antagonist that blocks parasympathetic results, the heart rate usually will increase substantially. When both divisions of the autonomic nervous system are blocked, the center fee of younger adults averages roughly a hundred beats per minute. The fee that prevails after complete autonomic blockade is called the intrinsic heart rate. Regulation of Heart Rate and Myocardial Performance Cardiac output is outlined as the amount of blood pumped by the heart each minute. Cardiac output could also be varied by a change within the coronary heart rate or the amount of blood ejected from both ventricle with each heartbeat; this volume is called the stroke quantity. Heart price is regulated by the exercise of the autonomic nervous system to modulate the intrinsic cardiac pacemaker. In half the trials, atropine was given first (top curve); within the different half, propranolol was given first(bottom curve). In people, centrifugal vagal fibers pass inferiorly through the neck near the common carotid arteries after which via the mediastinum to synapse with postganglionic vagal cells. These cells are positioned either on the epicardial floor or throughout the walls of the guts. The sympathetic nerves were stimulated at 0, 2, and 4Hz in the presence of vagal nerve stimulation (Vag) at zero, 4, and 8Hz. When the frequency of sympathetic stimulation increases from 0 to four Hz, the guts rate will increase by roughly eighty beats per minute in the absence of vagal nerve stimulation (0 Hz). However, when the vagus nerves are stimulated at eight Hz, rising the sympathetic stimulation frequency from 0 to 4 Hz has only a negligible affect on coronary heart rate. These fibers emerge from the spinal column via the white speaking branches and enter the paravertebral chains of ganglia. The preganglionic and postganglionic neurons synapse primarily in the stellate or center cervical ganglia, relying on the species. In the mediastinum, postganglionic sympathetic and preganglionic parasympathetic fibers be a part of to form a complicated plexus of blended efferent nerves to the center. The postganglionic cardiac sympathetic fibers on this plexus strategy the base of the guts alongside the adventitial surface of the good vessels. From the bottom of the heart, these fibers are distributed to the various chambers as an intensive epicardial plexus. Nerve terminals take as much as 70% of the norepinephrine launched throughout sympathetic stimulation; a lot of the remainder is carried away by the bloodstream. Furthermore, the facilitatory effects of sympathetic stimulation on the guts attain steady-state values far more slowly than do the inhibitory results of vagal stimulation. The onset of the cardiac response to sympathetic stimulation begins slowly for two major reasons. First, norepinephrine appears to be released slowly from the sympathetic nerve terminals. The hypothalamic facilities also provoke the cardiac response to alterations in environmental temperature. Experimentally induced temperature changes within the preoptic anterior hypothalamus alter the heart price and peripheral resistance. Stimulation of the parahypoglossal area of the medulla reciprocally activates cardiac sympathetic pathways and inhibits cardiac parasympathetic pathways. In sure dorsal regions of the medulla, distinct cardiac accelerator sites (increase the heart rate) and augmentor websites (increase cardiac contractility) have been detected in animals with transected vagus nerves. The accelerator regions are extra ample on the proper facet, whereas the augmentor websites are more prevalent on the left. Therefore, the sympathetic fibers mainly descend ipsilaterally by way of the brainstem. Baroreceptors positioned within the aortic arch and carotid sinuses are liable for this reflex (see the section "Arterial Baroreceptors"). The inverse relationship between coronary heart fee and arterial blood pressure is mostly most pronounced over an intermediate vary of arterial blood pressures. Below this intermediate range, the heart rate maintains a continuing, high worth; above this stress range, the heart price maintains a relentless, low value. Below this vary of carotid sinus strain, sympathetic activity is intense, and vagal activity is virtually absent.
In general anxiety meds for dogs order 40 mg cymbalta with visa, the despair is believed to mirror depletion of the number of releasable presynaptic vesicles anxiety 30000 safe cymbalta 30 mg. Thus anxiety lump in throat purchase cymbalta 60 mg with visa, short-term despair of synaptic transmission is most frequently and most easily seen at synapses by which the probability of release after a single stimulus is excessive and under conditions that favor release. A postsynaptically related reason for synaptic depression could be desensitization of the receptors in the postsynaptic membrane. So in general, the type of modulation noticed will depend upon which course of dominates. This in turn can mirror stimulus parameters, native ionic conditions, and the properties of the synapse. In particular, synapses have completely different baseline probabilities for releasing vesicles. Synapses with a high release probability shall be more more probably to present poststimulus depression, whereas those with low release probability are less more likely to deplete their vesicle retailer and thus may be facilitated more simply. For example, throughout a tetanic stimulus train a synapse could present a depressed response, but after the train the synapse can present posttetanic facilitation once the vesicles are recycled. Presynaptic Receptors Can Modulate Transmitter Release Just as the postsynaptic membrane incorporates receptors for neurotransmitters, so does the presynaptic membrane. When these presynaptic receptors bind neurotransmitter, they trigger occasions that can modulate subsequent launch of transmitter by the terminal. There are several sources of transmitter that bind to presynaptic receptors: it can be the transmitter released by the terminal itself. In the latter case, recall that their motion shall be comparatively gradual in onset and long in period and the impact will rely upon the particular second messenger cascades which are activated. Such cascades can finally regulate presynaptic voltage-gated Ca++ and K+ channels and other presynaptic proteins and thereby alter the chance of vesicle release. In distinction, activation of presynaptic ionotropic receptors will directly alter the electrical properties of the presynaptic terminal and cause rapid transient (millisecond time scale) modifications in the likelihood of vesicle release (although they can also have much longer lasting effects). Binding of an ionotropic receptor will open channels within the presynaptic terminal and thereby alter the quantity of transmitter launched by an motion potential. First, opening of channels decreases membrane resistance and creates a current shunt. The shunt acts to divert the present associated with the action potential from the lively zone membrane and thereby lessens the depolarization of the energetic zone, which results in less activation of Ca++ channels, much less Ca++ entry, and fewer release of transmitter. A second mechanism is the change in membrane potential attributable to the opening of presynaptic ionotropic channels. If a small depolarization is the end result, there shall be inactivation of voltage-gated Na+ channels and thereby lessening of the action potential�associated present and transmitter launch. However, within the presynaptic terminal, the [Cl-] gradient is such that Cl- flows out of the cell and generates a small depolarization. In reality, there are other receptors that management cation channels and create massive depolarizations, thereby increasing the release of transmitter. By allowing additional entry of Ca++, these receptors improve the discharge of transmitter from the terminal. Long-Term Changes in Synaptic Strength Repetitive stimulation of certain synapses in the mind can also produce more persistent adjustments in the efficacy of transmission at these synapses, a course of called long-term potentiation or long-term melancholy. Such changes can persist for days to weeks and are believed to be involved in the storage of memories. The elevated synaptic efficacy that occurs in long-term potentiation in all probability involves both presynaptic (greater transmitter release) and postsynaptic (greater sensitivity to transmitter) adjustments, in contrast to the short-term changes that involve changes solely in presynaptic operate. Entry of calcium into the postsynaptic region is an early step required for initiating the modifications that lead to long-term enhancement of the response of the postsynaptic cell to neurotransmitter. In the presence of excessive [Ca++], this kinase can phosphorylate itself and thereby turn out to be lively. After appropriate stimulation of a presynaptic pathway, the variety of dendritic spines and the variety of synapses on the dendrites of postsynaptic neurons might enhance quickly. Changes in the presynaptic nerve terminal can also contribute to long-term potentiation. The postsynaptic neuron may release a signal (nitric oxide has been suggested) that enhances launch of transmitter by the presynaptic nerve terminal. Cholinergic neurons from the basal forebrain areas project diffusely throughout the neocortex and to the hippocampus and amygdala, and so they have been implicated in memory features. Neurotransmitters Neurotransmitters are the substances that mediate chemical signaling between neurons. For a substance to be thought-about a neurotransmitter, it should meet a quantity of generally recognized criteria. First, the substance have to be demonstrated to be present within the presynaptic terminal, and the cell should have the power to synthesize the substance. This final criterion is definitely true for substances that act as synaptic transmitters, but when we want to be inclusive and embody substances that act over widespread territories rather than simply at a single synapse, the final criterion must be relaxed to include conditions by which receptors are situated at sites outside the synapse. Neurotransmission has been suggested as a general time period to describe both synaptic and nonsynaptic signaling between cells. These substances may be subdivided into three major categories: small-molecule transmitters, peptides, and gaseous transmitters. The small-molecule neurotransmitters may be additional subdivided into acetylcholine, amino acids, biogenic amines, and purines. The first three teams of small-molecule transmitters include what are considered the basic neurotransmitters. Remaining transmitters are substances that are newer additions to the record of neurotransmitters, though a lot of them have been generally known as biologically essential molecules in other contexts for a long time. Small-Molecule Neurotransmitters Acetylcholine In the peripheral nervous system, acetylcholine is the transmitter at neuromuscular junctions, at sympathetic and parasympathetic ganglia, and of the postganglionic fibers from all parasympathetic ganglia and some sympathetic ganglia. After release, the motion of acetylcholine is terminated by the enzyme acetylcholinesterase, which is highly concentrated in the synaptic cleft. The choline is then taken up by an Na+ symporter within the presynaptic membrane for the resynthesis of acetylcholine. The extracellular enzymatic degradation of acetylcholine is unusual for a neurotransmitter inasmuch because the synaptic motion of other classic neurotransmitters is terminated through reuptake by a sequence of specialized transporter proteins. When applied to cells, it causes depolarization and is launched from neurons, and specific receptors and transporters for it have been identified. In addition to being the principle excitatory neurotransmitter, glutamate is a potent neurotoxin at high concentrations. The most notable are the spiny neurons of the striatum and the Purkinje cells of the cerebellar cortex. The inhibitory nature of Purkinje cells was particularly surprising because they symbolize the whole output of the cerebellar cortex, and thus cerebellar cortical activity basically capabilities to suppress the exercise of its downstream targets (cerebellar and vestibular nuclei). Glycine features as an inhibitory neurotransmitter in a means more restricted territory. Glycinergic synapses are predominantly discovered within the spinal wire, where they symbolize approximately half of the inhibitory synapses. They are likewise current within the decrease brainstem, cerebellum, and retina in important numbers. Transport of the neurotransmitter into the cell is achieved by symport with two Na+ and one Cl- ion. In distinction, GlyT2 is situated on glycinergic nerve terminals and is largely restricted to the spinal wire, brainstem, and cerebellum. In noradrenergic neurons, another enzyme, dopamine -hydroxylase, converts dopamine to norepinephrine. Epinephrine is obtained by including a methyl group to norepinephrine via phenylethanolamineN-methyl transferase. In serotoninergic neurons, serotonin is synthesized from the important amino acid tryptophan. Tryptophan is first transformed to 5-hydroxytryptophan by tryptophan 5-hydroxylase, which is then converted to serotonin by aromatic L-amino acid decarboxylase. Finally, in histaminergic neurons the conversion of histidine to histamine is catalyzed by histidine decarboxylase. Removal of synaptically released biogenic amines is generally completed by reuptake into glia and neurons via transporters belonging to the Na+-Cl-�dependent transporter family. The catecholamines are then degraded by two enzymes, monoamine oxidase and catechol Omethyltransferase. Noradrenergic neurons are primarily found within the locus coeruleus and nucleus subcoeruleus, which are situated near each other within the dorsal part of the rostral pons.
Conversely anxiety hives buy cymbalta 40 mg with amex, a rise in extracellular [Ca++] enhances contractile drive anxiety in dogs symptoms purchase 30 mg cymbalta visa, and very excessive extracellular [Ca++] induces cardiac arrest in systole (rigor) anxiety meme purchase cymbalta 60 mg. The free intracellular [Ca++] is the factor principally liable for the contractile state of the myocardium. The course of by which the motion potential of the cardiac myocyte results in contraction is termed excitationcontraction coupling (see additionally Chapter 13). Cardiac muscle is worked up when a wave of excitation spreads quickly along the myocardial sarcolemma from cell to cell by way of gap junctions. Excitation additionally spreads into the inside of the cells through the T tubules, which invaginate the cardiac fibers at the Z traces. Electrical stimulation at the Z line or the application of Ca++ to the Z traces in a skinned cardiac fiber (whose sarcolemma is removed) elicits localized contraction of the adjacent myofibrils. During the plateau (phase 2) of the motion potential, permeability of the sarcolemma by Ca++ increases. Ca++ flows down its electrochemical gradient and enters the cell via calcium channels within the sarcolemma and in the T tubules. Ca++ leaves the sarcoplasmic reticulum via Ca++ launch channels, that are referred to as ryanodine receptors because the channel protein binds ryanodine avidly. This capability of the myocardium to resist stretch at high filling pressures in all probability resides in the noncontractile constituents of the center tissue (connective tissue), and it may serve as a security issue in opposition to overloading of the center in diastole. Usually, ventricular diastolic strain is approximately zero to 7 mm Hg, and the common diastolic sarcomere length is approximately 2. Gap junctions with excessive conductance are present in the intercalated disks between adjacent cells and facilitate conduction of the cardiac impulse from one cell to the following. Cardiac muscle should contract repetitively for a lifetime, and hence it requires a steady supply of O2. The Ca++�troponin C complicated interacts with tropomyosin to unblock energetic sites between the actin and myosin filaments. This unblocking initiates cross-bridge biking and hence contraction of the myofibrils. Mechanisms that elevate cytosolic [Ca++] enhance the drive developed, and those who lower cytosolic [Ca++] decrease the force developed. This in flip causes the release of extra Ca++ from the sarcoplasmic reticulum, and in consequence, contractile pressure increases. Increasing extracellular [Ca++] will increase the amount of Ca++ that enters the cell via the calcium channels and thereby increases contractile force as simply described. For instance, decreasing extracellular [Na+] causes much less Na+ to enter the cell in trade for Ca++, which ends up in an increase in intracellular [Ca++] and thus contractile drive. In reality, this is the mechanism by which cardiac glycosides increase contractile force. The elevated cytosolic [Na+] reverses the course of the 3Na+-Ca++ antiporter, and therefore less Ca++ is removed from the cell. Finally, contractile drive is diminished when intracellular [Ca++] is decreased by a reduction in extracellular [Ca++], by an increase in the Na+ gradient across the sarcolemma, or by the administration of a calcium channel antagonist that prevents Ca++ from coming into the myocardial cell. At the top of systole, the influx of Ca++ stops, and the sarcoplasmic reticulum is not stimulated to launch Ca++. As already described, it phosphorylates the calcium channel in the sarcolemma and causes increased entry of Ca++ into the cell, thus increasing the drive of contraction. In addition, protein kinase A phosphorylates different proteins that facilitate relaxation. However, when phospholamban is phosphorylated, its inhibitory action is reduced, and uptake of Ca++ into the sarcoplasmic reticulum is enhanced. Protein kinase A also phosphorylates troponin I, which in flip inhibits binding of Ca++ by troponin C. As a result, tropomyosin returns to its place of blocking the myosin-binding sites on the actin filaments, and leisure results. In the left ventricle, for instance, the blood filling and thus the stretching of the wall throughout diastole represents the preload. Again from the angle of the left ventricle, afterload is the stress in the aorta that should be overcome by the contracting left ventricular muscle to open the aortic valve and eject the blood. Preload could be increased by higher filling of the left ventricle during diastole. If diastolic filling continues beyond this level, the strain developed will now not increase. At very excessive filling pressures, peak stress development in systole is actually decreased. At a continuing preload, greater systolic pressure can be reached during ventricular contractions by an increase within the afterload. Incremental increases in afterload produce progressively higher peak systolic pressures. However, if the afterload continues to enhance, it turns into so great that the ventricle can no longer generate sufficient pressure to open the aortic valve. The maximal strain developed by the left ventricle underneath these conditions is the maximal isometric pressure that the ventricle is able to producing at a given preload. Preload and afterload rely upon certain characteristics of the vascular system and the behavior of the center. With regard to the vasculature, the diploma of venomotor tone and peripheral resistance influences preload and afterload. With regard to the heart, a change in price or stroke volume also can alter preload and afterload. Left ventricular pressure (mm Hg) vascular factors interact with each other to affect preload and afterload (see Chapter 19). Contractility determines the change in peak isometric force (isovolumic pressure) at a given initial fiber size (end-diastolic volume). Contractility could be augmented by medication, corresponding to norepinephrine or digitalis, or by an increase in contraction frequency (tachycardia). The enhance in contractility (positive inotropic effect) produced by these interventions is reflected by incremental will increase in the pressure developed and within the velocity of contraction. The slope of the ascending limb of the ventricular strain curve signifies the maximal rate of drive growth by the ventricle. At any given diploma of ventricular filling, the slope supplies an index of the preliminary contraction velocity and therefore an index of contractility. A(blue curve),control; B (dashed pink curve), hyperdynamic heart, as with administration of norepinephrine; C (green dashed curve), hypodynamic heart, as in cardiacfailure. In addition, the ejection fraction, which is the ratio of the amount of blood ejected from the left ventricle per beat (stroke volume) to the amount of blood in the left ventricle on the finish of diastole (end-diastolic volume), is extensively used clinically as an index of contractility. The ventricles comprise a continuum of muscle fibers originating from the fibrous skeleton on the base of the guts (chiefly across the aortic orifice). They cross towards the endocardium and steadily endure a 180-degree change in course to lie parallel to the epicardial fibers and to form the endocardium and papillary muscle tissue. At the apex of the guts, the fibers twist and turn inward to form papillary muscular tissues. Ventricular ejection can additionally be completed by a decrease within the longitudinal axis as the guts begins to slim towards the base. The early contraction of the apical part of the ventricles, coupled with the approximation of the ventricular partitions, propels the blood toward the ventricular outflow tracts. Movement of the valve leaflets is actually passive, and the orientation of the cardiac valves is liable for the unidirectional flow of blood via the guts. The tricuspid valve, located between the right atrium and the proper ventricle, is made up of three cusps, whereas the mitral valve, which lies between the left atrium and the left ventricle, has two cusps. Attached to the free edges of those valves are fantastic, sturdy ligaments (chordae tendineae cordis) that come up from the highly effective papillary muscle tissue of the respective ventricles. These ligaments prevent the valves from becoming everted during ventricular systole. In a traditional heart, the valve leaflets remain relatively close together throughout ventricular filling. The pulmonic and aortic valves are located between the right ventricle and the pulmonary artery and between the left ventricle and the aorta, respectively. At the top of the reduced ejection part of ventricular systole, blood flow Semilunar Valves briefly reverses toward the ventricles. This reversal of blood flow snaps the cusps collectively and prevents regurgitation of blood into the ventricles. In these sinuses, eddy currents develop, which are inclined to keep the valve cusps away from the vessel partitions.






