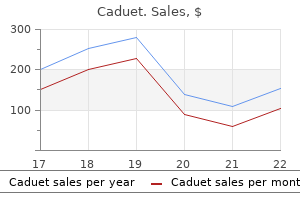
Caduet
Caduet
Caduet dosages: 5 mg
Caduet packs: 30 pills, 60 pills, 90 pills

Once resistance is met cholesterol levels in free range eggs buy generic caduet 5mg, the stentriever is recovered while sustaining steady aspiration on the catheter cholesterol lowering foods list caduet 5 mg cheap free shipping. Lesions that are refrac tory to aspiration or stentriever clot retrieval may require angioplasty or stent placement to obtain patency cholesterol test how accurate 5mg caduet with amex. Injury to the cervical or petrous vessel can happen while advanc ing the guide sheath or distal catheter, notably in sufferers with tortuous anatomy. If a dissection is suspected, an exchangelength microwire is delivered distally to keep access across the dissection before information catheter withdrawal. Distal clot embolization or emboli in new territories can even happen after an initial try of clot retrieval. If a vessel perforation occurs in the course of the proce dure, it might be necessary to inflate a balloon to obtain hemostasis. In uncommon instances, the father or mother vessel have to be sacrificed with coils or liquid embolic material. Once enough recanalization has been achieved, the blood pressure must be tightly regulated to keep away from reperfusion damage. Often using a fastacting calcium channel blocker, similar to nicardipine or clevidipine, is critical. Once hemostasis is achieved on the entry site, usually using a closure gadget, the patient is transported to the intensive care unit. Patients randomized to surgery underwent ipsilateral decompressive hemicraniectomy inside 30 hours of symptom onset. Although the research was stopped early because of sluggish recruitment, a big discount in mortality (52. Assessment of practical outcomes at 1 yr demonstrated that the surgical group had a non�statistically significant increase in modified Rankin scores of 3 or much less (50% versus 22%) and a non�statistically significant increase in scores of four or greater (25% versus 0%), suggesting that hemicraniectomy increases the number of survi vors with each good and poor practical outcomes. A 65-year-old girl with wake-up symptoms of right-sided weakness and language problem. C, Catheter-based angiography confirmed a center cerebral artery occlusion, which was retrieved with a single pass of stentriever-assisted guide aspiration thrombectomy (D). A, Computed tomography revealed no hemorrhage, and magnetic resonance imaging revealed right cerebellar infarcts and (B) raised concern for basilar occlusion on T1-weighted imaging and (C) gradientrecalled echo. D, Catheter-based angiography confirmed a basilar occlusion, which was retrieved with a single pass of guide aspiration thrombectomy (E). One hundred and twelve patients older than 60 years have been assigned to hemicraniectomy or conservative administration inside forty eight hours of symptom onset. A pooled analysis of these trials demonstrated that decompres sive hemicraniectomy led to a major reduction in mortality, a twofold increase in Rankin scores of three or much less, and a 10fold enhance in Rankin scores of four or less and not utilizing a important improve in sufferers with extreme incapacity. Schematic depicting fundamental concepts necessary to obtain good outcomes with endovascular remedy of enormous vessel occlusion. The incidence of hemorrhagic stroke continues to rise with rising use of anticoagulation remedy. Furthermore, in young adults (1855 years old), hemorrhagic stroke accounts for up to 50% of all stroke subtypes. Posterior Fossa Decompression for Cerebellar Stroke the benefit of surgical administration of cerebellar infarct has not been subjected to a randomized managed trial because of a scarcity of clinical equipoise. It is mostly beneficial that sufferers with cerebellar infarcts who deteriorate neurologically endure suboccipital craniectomy,fifty five and that decompression ought to occur as soon as clinical signs of brainstem compression occur. Further more, resection of infarcted tissue ought to be used if essential to ensure adequate decompression of the brainstem. Clinical outcomes following suboccipital decompression are better than in the case of supratentorial ischemia, with 40% to 50% of survivors living with gentle incapacity or higher. Endovascular therapy is a secure and efficient approach to revascularization in a subset patients with significant deficit in the setting of a small infarct core. Ongoing scientific trials will refine the subset of sufferers which would possibly be more than likely to benefit from this remedy. Huang and colleagues66 discovered that brain edema in rats was instigated by intracerebral injection of each hemoglobin and heme breakdown merchandise and attenuated by coadministration of heme oxygenase inhibitors and iron chela tors. This speculation remains conten tious, however, as a number of authors would recommend that the perfusion deficit outcomes from decreased oxygen demand of injured tissue somewhat than tissue at danger of ischemia. Patient outcomes have been reported as an intentiontotreat evaluation, however crossover occurred generally, as 26% of patients randomized to the medical man agement arm finally had surgery (85% craniotomy, common 60 hours between ictus and surgery). A prespecified subgroup analysis advised a functional consequence benefit to early surgical procedure for sufferers prede termined to have a poor prognosis given their age, presenting Glasgow Coma Scale score, and hematoma volume. DecompressiveCraniectomy Decompressive hemicraniectomy with out clot evacuation has additionally been reported as a surgical administration option for patients with supratentorial intracerebral hemorrhage. Historical Perspectives Hematoma evacuation has been contested since a randomized trial by McKissock and colleagues demonstrated no clinically important variations in end result between sufferers managed by craniotomy with clot evacuation versus these handled medically. Subgroup analysis demonstrated that hematoma dimension and location had been important elements in affected person outcomes. This research advised that sufferers with good neurological examination results and complete effacement of the fourth ventricle should bear clot evacuation earlier than decom pensation to maximize outcomes. Stereotactic imageguided catheter placement with clot aspi ration and intracavitary instillation of fibrinolytic brokers facilitate quicker clot decision than medical administration alone does. More recently, Miller and colleagues93 revealed a small collection of patients comparing endoscopic evacuation to maximal medical administration and located a major distinction in hematoma volume change (�80% versus +78%) and 90day mortality (20% versus 50%). In a small examine comparing endoscopic evacuation and stereotactic evacuation, endoscopic administration demonstrated smaller residual clot volumes, shorter intensive care unit stays, and higher useful outcomes at 6month followup. Renewed curiosity in minimally invasive therapies has come following disappointing results of hematoma evacuation via craniotomy in large, randomized trials. Further proof is important to set up optimum therapy tips in this patient population. Evolution of reperfusion therapies for acute brain and acute myocardial ischemia: a systematic, comparative evaluation. Good scientific consequence after ischemic stroke with successful revascularization is timedependent. Prognosis of untreated strokes because of anterior circulation proximal intracranial arterial occlusions detected by use of computed tomography angiography. Final infarct quantity is a stronger predictor of consequence than recanalization in sufferers with proximal center cerebral artery occlusion treated with endovascular therapy. Combined intravenous and intraarterial recanalization for acute ischemic stroke: the Interventional Man agement of Stroke Study. Validity and reliability of a quantitative computed tomography rating in predicting outcome of hyperacute stroke before thrombolytic remedy. The penumbra pivotal stroke trial: safety and effectiveness of a new technology of mechani cal devices for clot removing in intracranial giant vessel occlusive disease. Manual aspiration thrombectomy: adjunctive endovascular recanalization approach in acute stroke interventions. Advanced modality imaging evaluation in acute ischemic stroke could lead to delayed endovascular reperfusion remedy with out enchancment in clinical outcomes. Imagingbased endovascular remedy for acute ischemic stroke because of proximal intracranial anterior circulation occlusion handled past eight hours from time final seen properly: retro spective multicenter analysis of 237 consecutive patients. Timing of neurologic deterioration in large middle cerebral artery infarction: a multicenter evaluate. Early decompressive surgical procedure in malignant infarc tion of the center cerebral artery: a pooled evaluation of three ran domised managed trials. Hemicraniectomy for enormous center cerebral artery territory infarction: a scientific review. Decompressive hemicraniectomy, strokectomy, or each within the remedy of malignant middle cerebral artery syndrome. Neurological restoration after decompressive craniectomy for enormous ischemic stroke. Recommendations for the management of cerebral and cerebellar infarction with swelling: a statement for healthcare professionals from the American Heart Association/ American Stroke Association. Longterm end result after suboccipital decom pressive craniectomy for malignant cerebellar infarction. Surgical and medical handle ment of sufferers with huge cerebellar infarctions: results of the GermanAustrian Cerebellar Infarction Study. Longterm consequence after surgical therapy for spaceoccupying cerebellar infarction experience in 56 sufferers. Role of blood clot formation on early edema develop ment after experimental intracerebral hemorrhage. Combination of thrombin and matrix metalloproteinase9 exacerbates neurotoxicity in cell tradition and intracerebral hemorrhage in mice.
Similarly cholesterol and high blood pressure 5 mg caduet generic free shipping, in circumstances of foramen magnum obstruction or of spinal tethering as a result of a fatty filum cholesterol chart table cheap caduet 5mg line, suboccipital decompression or filum terminale sectioning must be considered prior to cholesterol medical term definition caduet 5mg purchase with visa consideration of any syrinx shunting process. A number of surgical choices can be found, but outcomes are modest, with many patients requiring a number of procedures and experiencing neurological deterioration regardless of treatment. Stabilization of signs and avoidance of additional worsening are the goals of surgical intervention. Treatment of syringomyelia associated with arachnoid scarring brought on by arachnoiditis or trauma. Prevalence of several neurological ailments within the central provinces of the Iberian Peninsula in eighteenyear-old males. Syrinx measurement and duration of symptoms predict the tempo of progressive myelopathy: retrospective analysis of 103 unoperated circumstances with craniocervical junction malformations and syringomyelia. Invited submission from the joint section assembly on disorders of the backbone and peripheral nerves, March 2005. Prospective study of the incidence fee of post-traumative cystic degeneration of the spinal cord using magnetic resonance imaging. Pathophysiology of syringomyelia related to Chiari I malformation of the cerebellar tonsils. Stenosis of central canal of spinal wire in man: incidence and pathological findings in 232 autopsy instances. Experimental speaking syringomyelia in canines after cisternal kaolin injection. Post-traumatic syringomyelia (cystic myelopathy): a prospective research of 449 sufferers with spinal twine harm. Cardiac-gated phase-contrast magnetic resonance imaging of cerebrospinal fluid circulate within the prognosis of idiopathic syringomyelia. Residual deformity of the spinal canal in patients with traumatic paraplegia and secondary adjustments of the spinal twine. Post-traumatic syringomyelia and post-traumatic spinal canal stenosis: a direct relationship: review of 75 patients with a spinal cord harm. A medical magnetic resonance imaging research of the traumatised spinal cord more than 20 years following injury. The "presyrinx" state: is there a reversible myelopathic situation which will precede syringomyelia Development of post-traumatic cysts in the spinal twine of rats subjected to severe spinal cord contusion. Review of the secondary harm principle of acute spinal cord trauma with emphasis on vascular mechanisms. Patterns of chronic adhesive arachnoiditis following Myodil myelography: the significance of spinal canal stenosis and previous surgery. High-resolution constructive interference in a steady state imaging of cervicothoracic adhesive arachnoiditis. Hyaluronidase as an adjuvant in the administration of tuberculous spinal arachnoiditis. Syringopleural shunt as a rescue process in patients with syringomyelia refractory to restoration of cerebrospinal fluid circulate. Long-term outcomes and problems of the syringopleural shunting for treatment of syringomyelia: a medical examine. Okonkwo the willpower of spinal stability is one of the most necessary duties within the evaluation and administration of the trauma patient. Recognition of the presence or absence of spinal stability is crucial for clinical determination making, not just for guiding operative intervention, but in addition for informing subacute therapeutic methods. Despite voluminous literature and evaluation algorithms addressing this matter, the assessment and classification of spinal instability remains a big problem, demanding integration of the clinical historical past, neurological examination, radiographic findings, and a fundamental understanding of how altered spinal biomechanics and biokinematics will in the end have an effect on the individual affected person. Anatomy A motion section, or functional spinal unit, represents the principal useful unit of the backbone that displays biomechanical traits similar to those of the entire spine. This could additionally be divided into an anterior construction, forming the vertebral column, and a fancy set of posterior structures. The habits of a movement section is dependent on the individual properties, interaction, and integrity of these elements. The spine should also be thought-about a structure composed of a number of practical items linked in sequence, and due to this fact its whole behavior is a composite of those individual items. The most generally accepted common clinical definition of spinal stability is that promulgated by White and Panjabi. Spinal stability is completed by way of the interplay of three subsystems: (1) the vertebrae providing an osseous structural frame; (2) intervertebral disks, apophyseal joints, and ligaments providing dynamic support; and (3) the coordination of muscle response via neural management. The backbone may be rendered unstable when enough anatomic disruption by trauma or disease severely disrupts any one or a combination of these techniques. From the earlier definition, it follows that significant analysis and categorization of spinal stability must tackle both the extent of structural harm in addition to performance under physiologic loads. Therefore, when assessing a patient with spinal harm, one should evaluate three key kinds of stability: � Immediate mechanical stability � Neurological stability � Potential for long-term stability An appreciation of the underlying anatomic and biomechanical elements of the conventional and injured spine is a prerequisite for the effective analysis of stability as a result of these are the foundations of damage interpretation, administration, and prognostication. Spinal injuries must be reliably categorised to facilitate communication amongst treating physicians and to guide administration. Vertebrae the twenty-five vertebrae of the spinal column present the principal support for compressive hundreds. The vertebrae are composed of extremely porous trabecular bone and a dense outer shell. The vertebral end plate provides even distribution and mechanical load switch in addition to prevention of disk extrusion into the porous vertebral physique. The significance of the vertebral finish plate for sustaining vertebral physique integrity increases with lowering bone density. Biomechanical analysis has demonstrated that beneath axial compression loading, the primary component to fail is the vertebral body due to fracture of the top plates. The posterior parts of the vertebrae embody the neural arch, spinous and transverse processes, and articular processes (superior and inferior facets). The neural arch consists of the pedicles and laminae that, along with the posterior wall of the vertebral physique, kind the borders of the spinal canal. The transverse and spinous processes present attachment points for the skeletal muscular tissues and ligaments that initiate backbone motion. The superior and inferior articular processes of the facet joints constrain intersegmental motion by limiting the extent of torsion and shear. The orientation of the articular processes modifications relying on spinal region, with resultant variations in operate. The side (and pars interarticularis) participates in load sharing with the anterior column; in upright, neutral position, 10% to 20% of compressive forces are transmitted through the side; nonetheless, in hyperextension, 30% of compressive loads are transmitted by way of the facet. Appreciating physiologic backbone biomechanics is essential to the administration of traumatic damage as a result of it explains the interplay of anatomy under applied forces and actions and predicts the consequences of that interaction. Presented is info useful in understanding the basic biomechanical operate of the spine to permit a systematic IntervertebralDisk Axial load is transferred and distributed by way of the anterior column through the intervertebral disk. The disk is composed of two components: an internal, gelatinous nucleus pulposus and an outer, fibrous anulus. The anulus fibrosus incorporates laminated, fiber bands of alternating instructions hooked up to the osseous tissue at the periphery and to the cartilaginous finish plates at the center. Tensile energy of the disk is greater at the anterior and posterior regions and increases beneath compression. As opposed to compressive loads, torsional loading results in disk failure, a finding exaggerated in degeneration. Flexion and lateral bending end in loading situations that cause a 50% increase in posterior anulus deformation and a substantial enhance in nuclear strain. The transverse portion of the cruciate ligament is the thickest, strongest ligament of the whole spine; the predominant function is restraining translation of the atlas on C2, whereas allowing axial rotation of the atlas about the dens. The alar ligaments play an essential function in restraining rotation and lateral bending between the occiput and atlas and the atlas and axis. These modifications are mirrored by the spinal cord, which additionally adjustments cross-sectional space (changing from rounder in flexion to extra oval on extension).
She reported full reduction of signs for 15 years; nevertheless cholesterol levels genetic factors buy caduet 5 mg cheap, she had complaints of axial neck pain and indicators of myelopathy 1 month after a traumatic head injury cholesterol medication triplex discount caduet 5mg. Spinal wire compression at C3-C4 and C4-C5 is demonstrated on the magnetic resonance image cholesterol reduction medication caduet 5 mg amex. Postoperative anteroposterior (D) and lateral (E) radiographs after C3-C5 anterior discectomies, fusion with autologous iliac crest graft, and screw-plate stabilization. Several threat elements for the development of spinal instability after posterior lumbar decompression have been established, including preoperative radiologic evidence of dynamic instability or anterior spondylolisthesis, preserved disk house peak, sagittally oriented aspect joints, multilevel decompression, and the extent of aspect joint complicated or pars resection. Overaggressive pars resection is more prone to occur at the cranial ranges, notably L3 and above, if the decompression follows a rectangular rather than a trapezoidal form. Injury to the facet joint from direct capsular cauterization may also contribute to facet joint denervation and glacial destabilization. The goals of this process are to present decompression of the neural components, reduction of the deformity, restoration of sagittal alignment, and 360-degree stabilization by way of one method. Indirect neural decompression may be achieved by way of the restoration of the intervertebral and the foraminal top, and correction of spinal alignment via a lateral transpsoas approach. Under basic anesthesia, the affected person is positioned on a radiolucent Jackson backbone desk in the prone position. It is crucial that the hips be extended absolutely to permit the lumbar backbone to achieve maximal lordosis. Any hip flexion can be associated with relative kyphotic angulation of the lumbar backbone and should predispose to the event of flat again syndrome. The operative publicity includes the normal bony anatomy above and under or lateral to the earlier operative area. A 46-year-old man sustained an L2 burst fracture 31 years previously and was handled by decompressive laminectomy of L2 and L3. He came to our establishment with a 2-year history of intractable decrease back pain and an externally visible thoracic spinal deformity. A, Lateral 36-inch standing radiograph demonstrating an L2 fracture and a 49-degree kyphotic deformity measured from the highest of T12 to the underside of L4. B, Postoperative lateral 36-inch standing radiograph after pedicle subtraction osteotomy at L2, inner discount, T12-L4 posterior fusion, and screw-rod stabilization. In sufferers with evidence of neural compression, sharp dissection is undertaken to cleanly dissect scar tissue from the bony margins of the previous laminectomy. The margins of the earlier laminectomy are extended with a Kerrison rongeur to allow publicity of normal dura. The previous bone decompression is prolonged by bilaterally eradicating the remaining laminae, pars interarticularis, and inferior sides at the levels to be operated. After bone decompression, careful identification and dissection of the neural parts away from the scar tissue is then carried out. Significant epidural scar tissue can be resected with sharp instruments such as a curet or scalpel or a sharp Kerrison rongeur, as described previously. After decompression, the thecal sac and the exiting and traversing nerve roots are extensively exposed. Care is taken to protect the ventral and lateral margins of the anulus to enable the graft materials, both structural and morselized, to be contained within the interbody house. Once this is accomplished, an interbody graft is placed bilaterally as a result of we consider that a single cage with unilateral fusion is associated with an elevated pseudarthrosis rate. The carbon fiber cages that we use have a lordotic sagittal contour with the ventral floor being 2 mm larger than the dorsal surface. In sufferers with significant loss of lumbar lordosis or a optimistic sagittal steadiness, correction of the deformity may be achieved with the utilization of lordotically shaped interbody grafts. For higher grades of spondylolisthesis, the interbody graft is placed after at least partial discount of the deformity has been completed. By resecting the medial aspects of the subjacent superior sides, manipulation of the thecal sac and nerve roots is stored to a minimum throughout placement of the interbody graft. After bilateral placement of the lateral fusion bone, the screws are connected to one another with both plates or rods. The plates or rods are contoured within the sagittal aircraft to obtain lumbar lordosis. In this maneuver, distraction gadgets are used to deliver the pedicle screws to the overcontoured rods or plates, with the quantity of lordosis being elevated to match that of the contoured rods or plates. If needed, compression of the screws posteriorly may be performed to enhance the extent of lordosis that can be achieved. However, such compression must be used only along side ventral interbody help. In circumstances of spondylolisthesis, significant reduction of the deformity is often achieved after connecting the pedicle screws to the contoured rods or plates. Two large-bore suction drains could be positioned, at the discretion of the operating surgeon, and normal wound closure is then performed in layers. The overall aim of lumbar pseudarthrosis revision surgical procedure is to optimize both mechanical fixation and the environment for bone therapeutic. Strict adherence to the basic methods that promote bone therapeutic, similar to correct graft placement and recipient mattress preparation, is critical for acquiring profitable fusion. In the lumbar backbone, biomechanical optimization can be achieved by restoring the sagittal stability of the backbone and by load sharing via the addition of internal fixation devices. The presence of a significantly optimistic sagittal stability places a substantially increased flexion moment on posterior instrumentation. Preoperative axial proton density magnetic resonance picture (A), anteroposterior radiograph (B), and lateral radiograph (C) of a 31-year-old woman who had undergone an attempted posterior lumbar interbody fusion 1 yr beforehand. She had complaints of intractable decrease back ache, right lower extremity weak spot, right lower extremity numbness, and issue urinating. Imaging demonstrated migration of the cage into the spinal canal with compression of neural components. A unilateral screw-rod construct is demonstrated with a laterally misplaced S1 pedicle screw. Bilateral posterolateral fusion with autologous iliac crest graft and bilateral pedicle screw-rod stabilization were performed. The affected person experienced full aid of her radicular signs and lower again pain after the revision operation. In certain circumstances with neurological compression at the level of the foramen, we might use a lateral transpsoas strategy above the L4 level, particularly if sagittal and coronal correction is needed as properly. In the absence of neural component compression, the choice of strategy is largely influenced by the character of the earlier operation. Supplementation with circumferential stabilization improves the chance of attaining profitable fusion and better medical outcomes. This opportunity often negates the need to carry out mixed anterior and posterior or lateral and posterior surgery. Thus the majority of instances of pseudarthrosis of the lumbar backbone may be managed efficiently via a single dorsal publicity. In instances by which an instrumented posterolateral fusion has failed, an interbody device may be implanted through the posterior method to provide ventral column help and load sharing with the posterior assemble. In cases of failure of a stand-alone ventral interbody fusion, the fusion may be revised via the anterior method. In the nice majority of circumstances of revision lumbar fusion surgery, using autologous graft is most popular given the established history of a failed spinal fusion and the increased danger for recurrent nonunion. Recurrent Lumbar Disk Herniation Recurrent lumbar disk herniation is usually outlined as ipsilateral or contralateral herniated disk materials at the same stage because the index operation that causes recurrent symptoms of radiculopathy after a postoperative symptom-free interval of no much less than 6 months. This phenomenon is more frequent on the L4-L5 degree, maybe due to its increased mobility relative to different lumbar spinal movement segments. Recurrent herniation may pose a diagnostic challenge as a outcome of imaging research will demonstrate important postoperative modifications within the epidural space at the operated degree, corresponding to epidural scar tissue, adhesions, and bony hypertrophy. The herniated disk fragment is usually continuous with the intervertebral parent disk until sequestration of a free fragment has occurred. Preoperative anteroposterior (A) and lateral (B and C) radiographs of a 38-year-old man who had undergone posterior L5-S1 fusion and stabilization 10 years earlier. Imaging studies demonstrate L4-L5 spondylolisthesis and a linear defect of the posterior fusion mass. Exploration of the L5-S1 fusion mass demonstrated nonunion and segmental instability. The L5-S1 fusion was revised by placement of bilateral interbody cages by way of a posterior strategy.
Impact loading is the extra frequent kind of dynamic loading and generally occurs because of motorcar accidents cholesterol reducing kerala foods caduet 5 mg buy discount on line, falls cholesterol levels webmd discount caduet 5 mg mastercard, or sports collisions cholesterol in shrimp how much 5mg caduet discount mastercard. Impact loading usually outcomes from a combination of contact forces and inertial (acceleration) forces. The head response to impression conditions depends on the item that strikes the head. In this example, contact-related injuries happen each near and distant from the purpose of impression. Contact phenomena effects vary with the dimensions of the impacting object, the magnitude of pressure delivered, and the pressure path. Factors contributing to pressure magnitude embody the mass, floor area, velocity, and hardness of the impacting object. For objects bigger than roughly 2 sq. inches, localized skull bending happens instantly beneath the impact level and peripheral to the impression websites. Penetration, perforation, or localized depressed cranium fracture is more doubtless if the item has a floor space of lower than 2 sq. inches. In addition, stress waves can journey by way of the cranium and parenchyma from the purpose of influence; throughout the mind, these stress waves could cause localized stresses, distortion, and injury within the form of small hemorrhages. Blast overpressure loading is a 3rd type of dynamic loading that has obtained considerably extra consideration for the rationale that early 2000s due to the emergence of traumatic mind damage because the "signature injury" in the Iraq and Afghanistan conflicts. The relative motion of the pinnacle because the atmospheric shock wave passes across the top is nearly unnoticeable, and therefore this kind of loading can happen independently of both impulsive or impact loading. However, blast-induced accidents are sometimes extremely advanced as the passing of a "shock front" is often immediately followed by a powerful overpressure-sometimes referred to as the blast wind (a pressured super-heated air flow)-that may load the subject impulsively (with possible impression deceleration upon hitting ground, wall, or different surface) or through direct impression with projected objects. Tissue Properties and Responses to Loading Across all these loading regimens, pressure (or deformation) is considered the proximal explanation for tissue damage. In general, pressure may be considered as the amount of deformation the tissue undergoes as a result of applied mechanical force. Compressive pressure is the amount of contraction brought on when the fabric is compressed. For occasion, if a stiff cylinder is positioned upright on a tabletop and a stack of books is placed on the highest round face of the cylinder, the cylinder would shorten in relation to its original, unloaded length. If the cylinder was initially 10 cm in size and have become eight cm when the books were positioned on top, the material is claimed to withstand a 20% compressive pressure. In comparison, tensile strain is the quantity of elongation that happens when the fabric is stretched. If the column 10 cm in length turns into eleven cm lengthy when stretched, it undergoes a 10% tensile pressure (stretched size minus authentic size, divided by original length). Dilational strain, also referred to as volumetric pressure, is the change in volume that occurs when stress is utilized to all exposed sides of a material. Most materials show unfavorable or positive dilational strains when constructive or negative pressures, respectively, are utilized to the material. Shear strain may be thought-about the amount of distortion that occurs in response to forces applied all along the surface of the fabric. A common illustration of shear pressure is the distortional change that happens in a neatly stacked deck of playing playing cards when one hand is moved across the highest of the deck. None of the playing cards are compressed or stretched on account of this motion, but the facet profile of the deck changes from a rectangle to a parallelogram. The quantity that the side profile varies from a normal rectangle signifies the state of shear strain. The pressure restrict of bony and soft tissue earlier than damage happens depends not solely on the drive. Materials similar to concrete are perfect for sustaining giant compressive masses, but they want reinforcement to sustain the same loads or deformation under rigidity. For biologic materials, bone is a prototype materials that reveals high compressive energy and is weaker in tension and shear. In comparability, rubber materials can often reach deformations two or thrice their authentic size earlier than breaking. Brain tissue is amongst the softest supplies within the body, and its mechanical behavior is often based on descriptions used for rubber-like supplies, simply reaching deformations of 20% to 50% before failing. Illustration of the various sorts of pressure associated with traumatic intracranial harm. The dashed traces symbolize the undeformed shapes; the shaded objects characterize the deformed configurations. Tearing of vessels is usually described when it comes to a tensile pressure restrict, in which the limit is described as a fraction (usually percentage) of the original vessel size. Bone tissue can sustain each tensile and compressive loading, and the failure restrict for each kind of loading is often distinct. Pressure (P) applied to all sides of a fabric causes a dilational (volumetric) pressure, which can be a mechanism to contemplate at very excessive loading rates. Arrows in every diagram indicate the drive path that causes the resulting deformation. If pulled slowly, Silly Putty can lengthen and deform substantially earlier than breaking. If, nevertheless, this material is pulled very quickly, the fabric breaks at a much shorter size. In addition to the material properties of the tissue, the mechanical tolerances of those tissues-which could be thought of as thresholds for irreversible damage-are the important determinant in the conditions that cause harm. Bone, for instance, is significantly stronger than either vascular or mind tissue; substantially more force is required to induce damaging levels of stress. The amount of pressure that bone can tolerate is actually less than that needed to injure mind tissue. The key distinction is the stiff mechanical properties of bone in comparison with both brain or vascular tissue: it takes considerable force to trigger 1% to 2% pressure in bone. Like vascular and brain tissue, bone additionally withstands compressive strain and shear strain, with a tensile power tolerance somewhere in between. Because brain tissue is virtually incompressible in vivo and it has a really low tolerance to tensile and shear pressure, each tensile and shear strains are usually the causes of brain harm. Whether vascular or brain tissue damage happens is decided by the precise properties and tolerances of these two tissue varieties. As discussed later, vascular tissue tends to fail under more quickly utilized masses than does mind tissue and, relying on the type of loading to the top, beneath certain circumstances, comparatively pure harm can occur with vascular parts rather than the neural elements within the head. During an impact (arrow in B), the scalp and underlying cranium endure deformation. With its stiff mechanical properties, bone bends inward, which creates localized stresses inside the bone and adjacent mind tissue (stress waves indicated as rounded traces emanating from the impression website in B). The stress throughout the bone is tensile on the inner table and compressive along the outer table. Most bony structures fail under pressure earlier than compression, and therefore the initial site of skull fracture occurs alongside the inside desk (C, arrow). In contact injuries, the pinnacle strikes an object or is struck, no matter whether the blow causes the head to move thereafter. Inertial injuries are sometimes called head movement or acceleration accidents because they result from violent head movement, no matter whether the pinnacle strikes due to a direct blow. In this scenario, the contact injury can be the skull fracture and underlying contusion that occurred from the impact pressure. Because most impacts additionally trigger head motion to some degree, contact accidents hardly ever happen alone clinically. Contact forces are of two types: local effects at or close to the impact website and effects distant from the area of impression. Local Contact Effects Examples of injuries from native contact results include most linear and depressed skull fractures, some basilar cranium fractures, epidural hematomas, and coup contusions. These accidents generally occur when an object transferring at a high velocity strikes the pinnacle: as an example, a baseball or a baseball bat. Penetrating accidents by overseas objects, corresponding to a bullet or shrapnel, also fit on this class. Additional elements embody the magnitude and course of impact and the scale of the impacted area. Bone, naturally resistant to compressive forces and strains, is less immune to the tensile forces on the inside cranium surface.
It ultimately depends on bony fusion to provide stability to the area and to hold the implants in place cholesterol ratio is 3.8 5 mg caduet generic otc. The techniques of fixation for atlantoaxial dislocation can be divided into midline procedures that involve the fixation of arch of the atlas with the lamina of axis and lateral mass fixation procedures cholesterol medication knee pain 5 mg caduet order with mastercard. OccipitocervicalFixation Occipitocervical fixation is often used as a therapy good cholesterol chart levels generic caduet 5 mg visa. The relative ease of the surgical process has made it a popular method of craniovertebral stabilization. Goel and Laheri23 have been among the many first to describe placement of occipital screws for occipitocervical stabilization. In their strategy of occipitocervical fixation, they fixed the occipital end of the plate with screws and the cervical end of the plate with C1 lateral mass and C2 pedicle screws. The use of occipital screws requires careful assessment of the thickness of the occipital bone and the placement of the dural venous sinuses. Generally, screws as a lot as 8 mm long may be inserted in the region of the superior nuchal line up to 2 cm laterally from the center of the exterior occipital protuberance, 1 cm from the midline at a level 1 cm inferior to the external occipital protuberance, and 0. The cervical end of the implant is fastened to one or more of the cervical vertebrae, more regularly to the posterior parts of the axis. However, wire fixation alone is inadequate to keep postoperative stability, and bony union relies upon primarily on inflexible postoperative external orthosis or prolonged mattress rest, or each. C1-C2 pedicle screws and C1-C2 transarticular screws had been used as the cervical anchor, and Y-shaped plates or rods were used to join these to the occipital screws. However, these constructs were biomechanically not equal to C1 lateral mass and C2 pedicle screw or C1-C2 transarticular fixation. As C2 screw placement requires expertise and may be technically demanding, alternative sites are getting used, corresponding to screws placed in the spinous strategy of C2 or on the spinolaminar junction as described by Goel25 and C2 lamina screws as described by Wright and colleagues. Recent studies have questioned the validity of inclusion of the occipital bone within the assemble. As the atlantoaxial joint is the positioning of pathology, besides in rare conditions, atlantoaxial stabilization is the aim of remedy. Atlantoaxial facetal fixation is possible, even in cases with assimilation of atlas. The massive dimension of the aspects of atlas, compared with the relatively skinny occipital squama, offers a powerful fixation level. To summarize, C1-C2 segmental fixation is the procedure of choice for atlantoaxial instability, however occipitocervical fixation can be an alternative form of fixation in case of technical difficulties. In an try and reduce an atlantoaxial dislocation surgically, Pilcher created an unintentional fusion by exposing the occiput and higher cervical spine. The main limitation of the wiring methods was the danger of dural and neurological injury and the requirement for intact posterior elements of the backbone to perform the procedure. To avoid these risks, facet-wiring methods have been also used to stabilize the craniovertebral junction. The Gallie fusion methodology of atlantoaxial stabilization was described by Gallie in 1930. The wire held within the midline a piece of bone autograft, which was notched to sit firmly over the spinous process of C2. Doubled 20-gauge wires are passed bilaterally underneath the laminae of the atlas and axis. Instead of the midline bone graft, two pieces of beveled bone graft are positioned posterolaterally in the interlaminar house bilaterally and held in place with the overlying wire. In the yr 1991, Dickman and colleagues described the use of C1-C2 wiring approach, which prevented use of sublaminar wires at C2. The loop of wire held between its ventral and dorsal side a bit of posterior iliac crest bone strut-graft. The bone graft was 4 cm lengthy and 1 cm broad and positioned horizontally between C1 and C2 such that the concave cortical margin lay against the dura. The graft was notched in the midline inferiorly to match the contour of the spinous means of C2. A notch was created on the spinolaminar junction of C2 bilaterally to allow the wire to fit appropriately into the slot thus created. The free ends of the wires had been then tightened to three turns per centimeter, thus holding the bone graft snugly in place. The remaining uncovered laminae of C1 and C2 have been decorticated, and items of cancellous bone graft were positioned over the region to enable fusion. Injury to the artery throughout surgical procedure can result in catastrophic intraoperative bleeding, and compromise to the blood circulate can lead to unpredictable neurological deficits, which will depend upon the adequacy of blood circulate from the opposite arteries of the brain. The twists and turns of the vertebral artery enable it a lot of movements in the area without getting stretched. The vertebral artery has a dynamic relationship within the region that adjustments upon neck actions. Extensive venous plexuses around the artery assist in the movements of the artery, and possibly empty on the contralateral aspect on neck turning. The artery has multiple loops and an intimate relationship with the atlas and axis bones. The shape, measurement, and placement of the vertebral artery groove on the inferior aspect of the superior articular aspect of the C2 and over the posterior arch of the atlas has wide variations. After a relatively linear ascent of the vertebral artery within the foramen transversarium of C6 to C3, the artery makes a loop medially toward an anteriorly positioned superior articular facet of the C2 vertebra, making a deep groove on its inferior surface. The distance of the artery from the midline of the vertebral body of C2, as would be observed during a transoral surgical procedure, averages 12 mm. The vertebral artery loops away from the midline underneath the superior articular side of the C2. Two giant superior articular facets of axis flank the dens or the odontoid course of. The superior aspect of the C2 vertebra differs from the facets of all other vertebrae in two essential traits. First, the superior facet of C2 is current in proximity to the body compared with different facets which might be positioned in proximity to the lamina. Second, the vertebral artery foramen is present partially or completely within the inferior side of the superior facet of C2, whereas in different cervical vertebrae, the vertebral artery foramen follows the same course as the transverse course of. The course of the vertebral artery relative to the inferior facet of the superior articular facet of the C2 makes it vulnerable to injury during transarticular and interfacetal screw implantation methods. The inferior side of the atlas is sort of round in many of the vertebrae, without any vital difference within the mean anteroposterior and transverse (15 mm) dimensions. The thickness of the inferior aspect under the posterior arch of the atlas averages 3. The thickness of the posterior arch of the atlas separating the vertebral artery groove from the inferior facet is roughly three. The rostral screw is positioned within the facet of C1 and the inferior screw is placed in the side of C2 via the pars/pedicle. The affected person is placed susceptible with the head finish of the table elevated to roughly 35 levels. Cervical traction stabilizes the top in an optimally lowered extension position and prevents any rotation. The traction additionally ensures that the weight of the head is directed superiorly toward the course of the traction and the pressure over the face or eyeball by the headrest is avoided. The head is in a "floating" position-that is, with headrest being positioned just for further or minimal assist. Elevation of the pinnacle finish of the desk, which acts as a countertraction, helps to scale back venous engorgement within the operative area. The suboccipital area and the higher cervical spine are exposed through an roughly 8-cm longitudinal midline pores and skin incision centered on the spinous process of the axis. The giant second cervical ganglion is closely related to the vertebral artery on its lateral aspect. After appropriate dissection, the ganglion could be retracted superiorly to expose the aspect of atlas. In some circumstances when the exposure of the side of atlas is inadequate, particularly in cases with basilar invagination, sectioning of the C2 ganglion can be accomplished to improve the publicity. Its part can provide a panoramic view of the region permitting the conduct of surgery underneath direct imaginative and prescient. Bleeding from the big venous sinuses within the region and in the extradural house may be troublesome. The joint capsule is minimize sharply, and the articular surfaces of the joint are uncovered.
Its proposed mechanisms of action embody protecting neuronal membranes cholesterol test fasting results order caduet 5 mg without prescription, lowering tumor necrosis factor- launch cholesterol juice fasting 5 mg caduet generic otc, enhancing spinal twine perfusion cholesterol webmd caduet 5mg cheap fast delivery, and lowering neuronal calcium inflow. At 6 months and 1 year follow-up, the 2 groups had related neurological outcomes, however the higher dose group had elevated wound an infection complication charges. Neuroprotective Agents Minocycline Minocycline is an artificial tetracycline antibiotic and metalloproteinase inhibitor with anti-inflammatory and antiapoptotic properties, appearing to suppress cytokine manufacturing, microglial activation, and neuronal death. Riluzole Riluzole is a benzothiazole sodium channel blocker believed to mitigate neurotoxic mechanisms by inhibiting presynaptic glutamate release and increasing high-affinity glutamate uptake, thereby reducing motor neuron degeneration. A part 1/2a trial evaluating the protection and pharmacokinetic profile of riluzole demonstrated efficacy with acceptable complication charges. It has been used historically as a hematopoietic growth factor for the treatment of neutropenia. Stem cells regulate gliosis and scar formation, stop cyst formation, and improve axon elongation. Laboratory investigations have demonstrated that hypothermia reduces cellular vitality necessities, slows enzymatic activity, and decreases cerebral metabolic price and glucose necessities. Recently completed, the study confirmed no enhance in complications related to hypothermia. This results in reduction of end-diastolic quantity and ventricular stroke quantity, which manifests as a lower in blood stress and signs of light-headedness, dizziness, fatigue, dyspnea, and syncope. Heavy meals also can exacerbate postprandial orthostatic hypotension by way of splanchnic blood pooling, insulin-induced vasodilation, and release of vasodilative gastrointestinal peptides. Other causes for enchancment may include vascular wall hypersensitivity and increased skeletal muscle tone. Even with persistence of hypotension relative to preinjury ranges, a tolerance to the symptoms might develop. Conservative administration of orthostatic hypotension consists of maintenance of euvolemia, compression stockings and belly binders to prevent peripheral pooling of blood, gradual tilt desk implementation, maintenance of head-up tilt throughout sleep, and use of a reclining wheelchair. Medications proven to be of benefit embrace midodrine, an oral 1-agonist, and fludrocortisone, a mineralocorticoid that protects intravascular fluid quantity by way of sodium retention. Caution must be taken in remedy of sufferers with preexisting congestive coronary heart failure and patients with persistent bradycardia, as a result of these conditions could be aggravated. During episodes of autonomic dysreflexia, upright positioning to evoke orthostatic hypotension, prompt survey for precipitating causes, frequent monitoring of blood strain, and administration of fast-acting antihypertensive drugs are key. This might end in impaired secretion clearance, atelectasis, and secondary an infection contributing to important morbidity and mortality. In the acute setting within the first 5 days of harm, atelectasis (36%), pneumonia (31%), and ventilatory failure (23%) are the most common issues. Once colonized, the endotracheal or tracheostomy tube may serve as a nidus for biofilm formation, exacerbating bacterial proliferation. The selection of specific antibiotics is dependent upon the previous cultures and native microbial resistance patterns. Manually assisted coughing by belly compression following a most insufflation capability maneuver, or a mechanical insufflation-exsufflation maneuver, has been shown to be simpler than normal suctioning at secretion clearance. This input is transmitted to the spinal wire by way of intact peripheral nerves, and evokes a reflex sympathetic surge inflicting vasoconstriction under the lesion. Peripheral arterial hypertension happens and is detected via intact carotid sinus and aortic arch baroreceptors. This offers the important mass of vascular volume to enable growth of systemic hypertension. Baroreceptors detect this hypertensive disaster, and respond with a massive inhibitory parasympathetic outflow in an attempt to attenuate the sympathetic response. Patients with autonomic dysreflexia current with acute hypertension, headache, profuse sweating, facial erythema, and blurred vision. Early chest physiotherapy must be incorporated to enhance respiratory effectivity, promote expansion of the lungs, strengthen respiratory muscle tissue, and mobilize secretions. This is most apparent when sufferers are positioned upright, which ends up in the diaphragm and belly contents being pulled down and ahead by gravity. The diaphragm becomes mechanically disadvantaged and generates decrease tidal volumes under maximal effort. Furthermore, identification and management of any underlying medical conditions and therapy of malnutrition and diabetes may contribute to optimal healing. Prophylaxis with histamine H2 antagonists for four weeks is recommended beginning on admission. For patients intolerant of enteral feedings, parenteral diet may be began in 7 days with vigilance for catheter-related and metabolic issues. Less than 1% of patients skilled full neurological restoration by the time of hospital discharge. A linear regression mannequin was created with the first end result modeled relative to scientific and imaging predictors obtained inside three days of damage, and a logistic mannequin was then created using the dichotomized secondary outcome and the same predictor variables. This prediction mannequin can be utilized to help the classification of sufferers inside clinical trials, and to support physicians in the prognostication of long-term consequence. Initial management ought to embrace fast assessment of concomitant injuries, early spinal immobilization, transfer to a specialised neurosurgical middle, and admission to an intensive care setting. Early identification and correction of these points can decrease hypoxemia and hemodynamic instability, both of which can exacerbate ongoing damage. The acute respiratory management of cervical spinal twine damage in the first 6 weeks after injury: a scientific evaluate. Cardiovascular complications after acute spinal wire injury: pathophysiology, diagnosis, and administration. A global map for traumatic spinal cord harm epidemiology: towards a dwelling data repository for harm prevention. Pathogenesis and pharmacological strategies for mitigating secondary damage in acute spinal twine damage. Molecular profile of reactive astrocytes- implications for their function in neurologic illness. Pressure ulcers from spinal immobilization in trauma sufferers: a systematic review. Effects of prehospital spinal immobilization: a scientific evaluate of randomized trials on wholesome subjects. The Injury Severity Score: a method for describing patients with multiple injuries and evaluating emergency care. International standards for neurological classification of spinal cord damage (revised 2011). Does the morphology of foramen transversarium fractures predict vertebral artery injuries The acute cardiopulmonary administration of patients with cervical spinal wire injuries. American Association of Neurological Surgeons and Congress of Neurologic Surgeons. Intubation after cervical spinal cord harm: to be accomplished selectively or routinely Cervical spine movement throughout flexible bronchoscopy in contrast with the Lo-Pro GlideScope. Altered cardiovascular responses to tracheal intubation in patients with complete spinal wire harm: relation to time course and affected stage. Cardiovascular abnormalities accompanying acute spinal twine damage in humans: incidence, time course and severity. Combined medical and surgical treatment after acute spinal cord harm: outcomes of a potential pilot examine to assess the merits of aggressive medical resuscitation and blood strain administration. Emerging approaches to the surgical administration of acute traumatic spinal wire harm. Agreement between orthopedic surgeons and neurosurgeons concerning a brand new algorithm for the remedy of thoracolumbar injuries: a multicenter reliability examine. Early versus late surgery for traumatic spinal cord damage: the outcomes of a potential Canadian cohort research. Results of the Third National Acute Spinal Cord Injury Randomized Controlled 303 2504. Neuroprotection by minocycline facilitates significant recovery from spinal twine damage in mice. A multi-center, randomized, placebo controlled, double-blinded, trial of efficacy and safety of riluzole in acute spinal twine injury.
Common impact points for producing basilar cranium fracture include the skull base estimating cholesterol ratio caduet 5 mg order mastercard, facial or mandibular bones cholesterol test home caduet 5mg discount mastercard, and distant cranium impact points cholesterol levels uk 5.4 generic 5 mg caduet otc. Focal Brain Injury EpiduralHematoma Epidural hematoma is generally a complication of linear skull fracture, though epidermal hematoma could happen without bone fracture. Typically, in the course of the fracture initiation or propagation interval, vessels within the underlying dural membrane are torn and bleeding ensues in the epidural area. These hemorrhages are generally arterial and, as such, may have grave consequences, including strain results, tissue dislocation, and herniation results. Alternatively, the local skull bending brought on by an influence could additionally be enough to tear dural vessels with out exceeding the failure restrict of the bone, which would result in subdural bleeding without skull fracture. Epidermal hematoma is an impact-based phenomenon; due to this fact, no head motion or inertial effects trigger an epidural hematoma. These phenomena, in flip, subject the underlying cortical and pial vascular community to strains that, if extreme, cause bleeding at or near the mind floor. Damage is prone to happen when the skull is "rebounding" from the impression and the vessels are experiencing tensile deformations. ContrecoupContusions Although world cranium deformation caused by impact could create tensile stresses and contusion injury distant from the positioning of impact, the predominant mechanism for contrecoup contusions is believed to be rotational acceleration. Indeed, two phenomena have historically been attributed to the pathogenesis of countercoup contusions: cavitation effects and inertial loading. Of the two, the extra probably mechanism of the contrecoup harm is inertial: translational or angular head motion. The concept of cavitation effects relies on the idea that on influence, the brain moves toward the impression website, and an area of unfavorable stress develops instantly reverse the point of loading. This unfavorable pressure might, in flip, trigger damage by exceeding the tensile power of neural tissue or, alternatively, by inflicting small gasoline bubbles to seem throughout the parenchyma. The return to regular or constructive pressures could then cause the small bubbles to collapse; that is termed cavitation. Similarly, the propagation of stress waves through the mind from blast overpressure may cause areas of brief unfavorable strain and cavitation, although direct experimental evidence at survivable overpressure ranges is necessary to support the relevance of this mechanism in blast-induced traumatic mind harm. Instead, it seems vascular disruption and cortical harm in contrecoup areas are primarily acceleration effects ensuing from both translation or angular head motions. Each head movement, significantly angular movement, is capable of producing shear and tensile strains throughout the mind. If the strain fields are larger than the vascular tolerance in a given region, contusion happens. The term contrecoup could also be somewhat deceptive: the crucial mechanism is most frequently acceleration and never instantly the contact effects from influence. Indeed, in situations by which the top undergoes impulsive loading, contrecoup contusions occur solely because of the strains generated in the cortical brain region in the course of the acceleration period. Strain concentrations could happen in particular regions of the brain because of geometric effects and are responsible, partially, for the high incidence of frontal and temporal lobe contusions observed clinically. Because of their macroscopic and simply identifiable nature, contusions are periodically used to characterize the biomechanical input to the top. However, several factors must be mentioned when contusions are used as a device on this method. The discussions in the previous paragraphs spotlight the importance of inertial loading in producing the pattern of contrecoup injury, in comparison to the position of native contact effects. Thus coup and contrecoup injuries, although differing solely slightly in name, come up from fundamentally completely different mechanisms. In fact, contusions of the temporal and frontal poles are contrecoup in nearly each occasion, regardless of the influence web site. Rather, the relative proportion of coup versus contrecoup contusions relies upon solely on the response of the top to loading. Because of the apparent pathogenesis, the acceleration of the top attributable to a concentrated blow has led to the proposal that acceleration causes coup contusions. However, a tough, small object that causes influence in these typical instances tends to produce focal cranium deformation with underlying coup contusion, and a big portion of the vitality is dissipated on the impression web site. In these cases, native skull deformation produces a noticeable coup contusion, and the dearth of considerable head movement produces slight or very limited contrecoup contusion. On the other hand, a softer or bigger impression object commonly causes a deceleration harm, which causes less native damage beneath the purpose of impression, inasmuch as a big proportion of the loading vitality is used to set the head into movement or stopping it from moving. In the latter case, the brain is believed to strike or be pulled away from the adjoining buildings, which results in compressive or tensile strains, respectively. Alternatively, intermediate contusions of the cingulate gyrus could be caused by interactions with the falx, and, similarly, those of the inferomedial temporal lobe may end up from involvement with the tentorium of the petrous ridge. IntracerebralHematoma Large traumatic intracerebral hematomas are unusual; most are related to in depth cortical contusions. They can be characterised as contusions during which bigger, deeper vessels have been disrupted. Intracerebral hematomas have been poorly studied but may symbolize a form of tissue tear hemorrhage that accompanies diffuse axonal injury. TissueTearHemorrhages Tissue tear hemorrhages are multiple areas of injury to blood vessels and axons occurring in combination with diffuse axonal injury. They are distinct from the intracerebral hematomas described previously and are actually a half of the pathologic state of affairs of a severe type of diffuse axonal injury that ends in quick prolonged coma. Tissue tear hemorrhages are typically quite a few, small, and positioned parasagittally and in the central portion of the brain. Their locations are characteristically in the superior medial frontoparietal white matter, corpus callosum, centrum semiovale, periventricular white and gray matter, internal capsule, and basal ganglia. In the brainstem, they seem in the dorsal space of the midbrain in the higher pons. Several elements contribute to these multiple foci of harm, together with the presence of intracranial partitioning membranes, the geometric irregularities of the skull, and the airplane of movement experienced by the top. Tissue tear hemorrhages represent areas of most accelerationinduced brain damage. The first sort of subdural hematoma is the most common type of vascular disruption; it involves tearing of parasagittal bridging veins located alongside the superior margin of the mind. Because of their superficial location, parasagittal bridging veins are vulnerable to harm throughout transient angular acceleration of the pinnacle. Common conditions in which this acceleration situation occurs include falls, when the pinnacle strikes a broad, hard surface, and in circumstances of assaults during which a majority of the impact energy is used to set the head in movement. Under these loading conditions, differential motion between the brain and dura cause concentrated shear strain fields alongside the outer margins where the parasagittal bridging veins reside. The other two forms of subdural hematoma are related to contusion and laceration and are sometimes referred to as difficult subdural hematomas. These end result from the contact or acceleration effects that triggered the first lesion. Across all these varieties, if vascular tolerances are surpassed, subdural bleeding happens, and mass effect from the hematoma might trigger brain compression. Because of its similar mechanism, subdural hematoma could coexist with underlying hemispheric brain damage, normally diffuse axonal injury (see subsequent section). This explains the frequency of cases in which the subdural hematoma is small however the underlying brain harm is bigger than anticipated. Diffuse Brain Injury CerebralConcussion Concussion is a transient, generally reversible neurological dysfunction brought on by trauma. All gradations of concussion are produced entirely by inertial loading and never from contact phenomena effects. However, like different accidents, concussion may be observed in combination with injuries arising from contact phenomena simply because the contact loading produces both contact effects and angular rotational acceleration of the head. Angular rotational head movement causes the deeper buildings within the brain to deform and causes the classical widespread disruption of mind function that underlies concussion. For a concussive harm, most of the strain is inadequate to cause structural damage. Instead, the harm to the structures may be both partially or fully reversible, relying on the severity of inertial loading. The exact location of the useful derangement of concussion continues to be debated. It stays unsettled whether angular acceleration affects principally the brainstem, the cerebral hemispheres, or many areas. However, diffuse axonal harm almost universally coincides with other forms of contact or inertial injuries. The quantity and placement of axonal damage as a consequence of rotational acceleration in all probability determines the severity (depth and duration) of damage and possibly has a robust influence on the quality of restoration.






