Levitra Soft
Levitra Soft
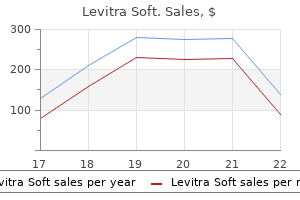
Levitra Soft dosages: 20 mg
Levitra Soft packs: 10 pills, 20 pills, 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Effect of ultrasonographically guided axillary nerve block mixed with suprascapular nerve block in arthroscopic rotator cuff repair: a randomized controlled trial erectile dysfunction watermelon levitra soft 20 mg generic visa. Ultrasound-guided infraclavicular brachial plexus block: an alternate technique to anatomical landmark-guided approaches erectile dysfunction 3 seconds 20 mg levitra soft generic with visa. The conjoint tendon of the latissimus dorsi and teres major: an important landmark for ultrasound-guided axillary block how young can erectile dysfunction start 20 mg levitra soft purchase visa. Radiological evaluate of intercostal artery: Anatomical considerations when performing procedures via intercostal space. Intercostal nerve block: a roentgenographic anatomic research of technique and absorption in people. Anatomic spread of India ink in the human intercostal area with radiographic correlation. Spectral evaluation of ultrasound radiofrequency backscatter for the detection of intercostal blood vessels. Intercostal nerve block in 4333 patients: indications, method, and issues. Ultrasound-guided blocks of the ilioinguinal and iliohypogastric nerve: accuracy of a selective new technique confirmed by anatomical dissection. Inadvertent extended femoral nerve palsy after area block with liposomal bupivacaine for inguinal herniorrhaphy. Comparison of the fascia iliaca compartment block with the 3-in-1 block in kids. Ultrasound-guided supra-inguinal fascia iliaca block: a cadaveric analysis of a novel approach. A longitudinal supra-inguinal fascia iliaca compartment block reduces morphine consumption after total hip arthroplasty. Adductor canal block versus femoral nerve block for analgesia after total knee arthroplasty: a randomized, double-blind study. Adductor canal block versus femoral nerve block for whole knee arthroplasty: a prospective, randomized, controlled trial. Prospective, doubleblind, randomized study to evaluate single-injection adductor canal nerve block versus femoral nerve block: postoperative functional outcomes after total knee arthroplasty. Fall-prevention methods and patient traits that impact fall charges after whole knee arthroplasty. Ultrasound-guided sciatic nerve block: description of a new approach at the subgluteal space. Gemelli-obturator complicated in the deep gluteal space: an anatomic and dynamic examine. Does the sciatic nerve method influence thigh tourniquet tolerance during below-knee surgery Preliminary results of a model new ultrasound-guided strategy to block the sacral plexus: the parasacral parallel shift. A prospective, randomized comparison between single- and multiple-injection methods for ultrasound-guided subgluteal sciatic nerve block. Ultrasound-guided anterior sciatic nerve block utilizing a longitudinal strategy: "expanding the view". Ultrasound-guided anterior approach to sciatic nerve block: a comparison with the posterior method. Ultrasound detection of arteria comitans: a novel approach to locate the sciatic nerve. Comparison of 2-chloroprocaine and prilocaine for intravenous regional anaesthesia of the arm: a medical examine. Comparison of ropivacaine and lidocaine for intravenous regional anesthesia in volunteers: a preliminary examine on anesthetic efficacy and blood degree. A modification of the method for intravenous regional blockade for hand surgery. Use of a temporary forearm tourniquet for intravenous regional anaesthesia: a randomised managed trial. Grand mal seizures after 2-chloroprocaine epidural anesthesia in a affected person with plasma cholinesterase deficiency. Lidocaine disposition following intravenous regional anesthesia with completely different tourniquet deflation technics. Adverse occasions related to intravenous regional anesthesia (Bier block): a scientific evaluation of complications. Electrical stimulation versus ultrasound guidance for popliteal-sciatic perineural catheter insertion: a randomized controlled trial. A novel method for assessing catheter position after ultrasound-guided placement of continuous interscalene block. A pilot in vitro analysis of the "air check" for perineural catheter tip localization by a novice regional anesthesiologist. Ultrasound-guided (needlein-plane) perineural catheter insertion: the effect of catheter-insertion distance on postoperative analgesia. The impact of fixation approach on steady interscalene nerve block catheter success: a randomized, double-blind trial. The effectiveness of making use of soft tissue bonding adhesive composed of 2-ethyl cyanoacrylate to epidural catheter fixations using movie dressings: an open-label, randomized, parallel-group comparative examine. Incidence of local anesthetic systemic toxicity and postoperative neurologic symptoms related to 12,668 ultrasound-guided nerve blocks: an evaluation from a prospective scientific registry. Regional anesthesia within the affected person receiving antithrombotic or thrombolytic therapy: American Society of Regional Anesthesia and Pain Medicine Evidence-Based Guidelines (fourth edition). Investigation of present infection-control practices for ultrasound coupling gel: a survey, microbiological evaluation, and examination of practice patterns. Infection related to ultrasound-guided single-injection peripheral nerve blockade: a decade of expertise at Toronto Western Hospital. The Third American Society of Regional Anesthesia and Pain Medicine Practice Advisory on local anesthetic systemic toxicity: government summary 2017. Lipid emulsion infusion: resuscitation for native anesthetic and other drug overdose. Inadvertent femoral nerve impalement and intraneural injection visualized by ultrasound. Case report: neurological deficit related to intraneural needle placement with out injection. A easy phantom for coaching in ultrasound-guided needle biopsy utilizing the freehand method. Characterizing novice habits related to learning ultrasound-guided peripheral regional anesthesia. Water makes up approximately 60% of complete body weight, various broadly with age and physique composition. The ratio between the water volume inside the intracellular and practical extracellular compartments is approximately 2:1. The endothelial glycocalyx types a protein-poor intravascular fluid layer at the vessel perimeter; it has been integrated right into a revised version of the Starling equation and updated mannequin of capillary fluid motion. Sodium is the dominant extracellular cation and is liable for much of extracellular fluid osmolality; dysnatremia is usually associated with disturbed extracellular fluid quantity. Potassium is the dominant intracellular cation with a key function in the upkeep of transmembrane potentials; dyskalemia may be accompanied by impaired operate of excitable tissues. Calcium is a key intracellular second messenger with roles in neuromuscular function, cell division, and oxidative pathways. Magnesium has a diverse range of physiologic results, underlined by the growing vary of therapeutic applications of supplemental magnesium within the perioperative setting. Acid-base steadiness is related to fluid remedy as a end result of fluids containing supraphysiologic levels of chloride could cause an iatrogenic acidosis; the clinical relevance of this acidosis is debated. Intravenous fluids have a variety of physiologic effects and ought to be considered medication with indications, dose ranges, cautions, and side effects. The physiologic insult of the perioperative interval could result in a broad variety of disturbances in fluid and electrolyte stability. A steadiness have to be found between inadequate fluid administration-allowing tissue hypoperfusion-and the opposed effects of excess intravenous fluids and toxicities associated to fluid constituents. No clear consensus exists on which intravenously administered fluid is related to one of the best scientific outcomes within the perioperative setting.
The hemodynamic response to unclamping is determined by many factors impotence hernia cheap 20 mg levitra soft with amex, together with the level of aortic occlusion vacuum pump for erectile dysfunction in pakistan buy generic levitra soft 20 mg on line, complete occlusion time erectile dysfunction my age is 24 20 mg levitra soft cheap visa, use of diverting assist, and intravascular quantity. Reactive hyperemia in tissues and organs distal to the clamp and the resultant relative central hypovolemia are the dominant mechanisms of the hypotension. AoX, Aortic cross-clamping; Cven, venous capacitance; R artwork, arterial resistance; Rpv, pulmonary vascular resistance. These humoral components and mediators, which may also play a role in organ dysfunction after aortic occlusion, embody lactic acid, renin-angiotensin, O2 free radicals, prostaglandins, neutrophils, activated complement, cytokines, and myocardial-depressant elements. It is important that correction of preoperative fluid deficits, upkeep of intraoperative fluid requirements, and substitute of blood loss be accomplished before unclamping. Vasodilators, if used, should be progressively reduced and discontinued earlier than unclamping. Moderate augmenting of intravascular quantity by administration of fluids (500 mL) during the instant prerelease period is indicated for infrarenal unclamping. More aggressive intravascular fluid administration is required in the interval immediately previous supraceliac unclamping. If significant hypotension outcomes, gradual launch of the aortic clamp and reapplication or digital compression are important measures in maintaining hemodynamic stability during unclamping. Although vasopressor requirements are minimal after release of the infrarenal clamp, vital support is often needed after the removal of supraceliac clamps. Caution must be observed when vasopressor help is used on this setting because profound proximal hypertension may occur if reapplication of the cross-clamp is required above the celiac axis. In addition, hypertension should be averted to stop damage to or bleeding from the vascular anastomoses. The selection of the type and the size of the central line may be selected a case-by-case basis. Placement of an arterial catheter must be routine in all patients undergoing aortic reconstruction. A noninvasive blood pressure cuff should be placed on the arm contralateral to the arterial catheter within the occasion of catheter malfunction. It ought to be reserved for patients with severely limited cardiopulmonary perform or advanced aortic reconstruction. The invasive monitoring catheters may be positioned earlier than or after induction of basic anesthesia. With selective use, accurate interpretation of knowledge, and rational treatment strategies, pulmonary artery catheter monitoring may be useful in high-risk patients present process complex aortic reconstruction. Yet the scientific value of pulmonary artery catheter monitoring in high-risk sufferers has not been established. The scientific usefulness of any monitoring technique ultimately is decided by affected person selection, correct interpretation of knowledge, and appropriate therapeutic intervention. The routine use of cell salvage during aortic surgical procedure is in all probability not cost-effective and thus it might greatest be reserved for a choose group of sufferers with an anticipated massive blood loss. A costeffective possibility is to use the cell salvage reservoir for blood collection and activate the full salvage course of only if massive blood loss happens. Cell Salvage Intraoperative cell salvage is a broadly used approach mixed with allogenic blood transfusion and in some facilities is considered routine. An early, nonrandomized study reported a 75% discount in the quantity Anesthetic Drugs and Techniques Various anesthetic strategies, including common anesthesia, regional (epidural) anesthesia, and mixed strategies, have been used efficiently for belly aortic reconstruction. Combined strategies most commonly use a lumbar or low thoracic epidural catheter along with common anesthetic. Local anesthetics, opioids, or, more generally, a combination of the two could additionally be administered by bolus or continuous epidural infusion. Maintenance of significant organ perfusion and function by the provision of stable perioperative hemodynamics is more important to overall end result than is the selection of anesthetic drug or approach. Given the frequent incidence of cardiac morbidity and mortality in patients present process aortic reconstruction, elements that influence ventricular work and myocardial perfusion are of prime importance. Induction of general anesthesia ought to ensure that steady hemodynamics are maintained throughout lack of consciousness, laryngoscopy and endotracheal intubation, and the quick postinduction interval. The addition of a short-acting, potent opioid similar to fentanyl or sufentanil often supplies steady hemodynamics during and after induction of anesthesia. Volatile anesthetics may be administered in low concentrations earlier than endotracheal intubation during assisted air flow as an adjunct to blunt the hyperdynamic response to laryngoscopy and endotracheal intubation. Esmolol 10 to 25 mg, sodium nitroprusside 5 to 25 g, nitroglycerin 50 to one hundred g, or clevidipine 100 mcg and phenylephrine 50 to 100 g must be out there for bolus administration throughout induction if needed to preserve appropriate hemodynamics. Maintenance of anesthesia could additionally be accomplished with a mixture of a potent opioid (fentanyl or sufentanil) and an inhaled anesthetic (sevoflurane, desflurane, or isoflurane). Patients with extreme left ventricular dysfunction may benefit from a pure opioid method, but a balanced anesthetic technique permits the clinician to benefit from probably the most desirable characteristics of potent opioids and inhaled volatile anesthetics whereas minimizing their undesirable unwanted effects. Nitrous oxide can be used to supplement both an opioid or an inhaled anesthetic. Various regional anesthetic and analgesic techniques have been used effectively throughout and after aortic reconstruction. For over 2 decades, interest has focused on the use of regional anesthetic and analgesic methods to reduce the incidence of perioperative morbidity in patients present process aortic reconstruction. The benefits of mixed fifty six � Anesthesia for Vascular Surgery 1839 common and epidural anesthesia intraoperatively, with or without epidural analgesia continued into the postoperative period, remain controversial. In a randomized trial utilizing epidural morphine in patients present process aortic surgical procedure, Breslow and associates72 found attenuation of the adrenergic response and a less frequent incidence of hypertension within the postoperative interval. A large randomized trial reported no discount in nonsurgical problems with using intrathecal opioid. Length of hospital keep might due to this fact be thought-about the result variable most instantly proportional to an built-in ultimate adverse impact of all important perioperative morbidity (excluding in-hospital death) and the variable more than likely to be altered by the anesthetic or analgesic technique. Norris and colleagues14 reported the results of a randomized clinical trial evaluating various combinations of intraoperative anesthesia. The research rigorously protocolized perioperative administration, standardized postoperative surgical care, and optimized postoperative pain management. The general incidence of postoperative problems in the trial was low and never totally different based mostly on anesthetic or analgesic method. Postoperative ache was well controlled overall, with related ache scores in both analgesic remedy groups. This design allows the inclusion of all 4 potential combinations on intraoperative anesthesia and postoperative analgesia and the power to separate the influences of time interval and technique. Data evaluation by treatment group, intraoperative treatment, postoperative therapy, and any epidural activation, as nicely as simultaneous consideration of each intraoperative and postoperative therapies in the identical mannequin (factorial analysis), is feasible and permits improvement in consequence to be attributed to the intraoperative anesthesia, postoperative analgesia, the mix of the 2, or to unrelated factors. The use of epidural native anesthetics in combination with general anesthesia during aortic reconstruction poses a number of issues, including hypotension on the time of aortic unclamping and the necessity for increased intravascular fluid and vasopressor necessities. Supraceliac aortic crossclamping could considerably exaggerate these disadvantages, and, as a result, some clinicians keep away from operating local anesthetics within the epidural across the period of aortic clamping and unclamping. Epidural opioids without local anesthetics can be used within the interim and native anesthetic could be given later, after aortic unclamping, when hemodynamics and intravascular volume have stabilized. Hypertension and tachycardia are aggressively managed during emergence by means of short-acting drugs similar to esmolol, nitroglycerin, clevidipine, or sodium nitroprusside. Emergence from anesthesia must be conducted after restoration of circulation and establishment of sufficient organ perfusion. Temperature Control Postoperative hypothermia is associated with many undesirable physiologic effects and may contribute to antagonistic outcomes (see also Chapter 80). If vital hypothermia occurs early in the procedure, normothermia is extremely difficult to achieve, and emergence and tracheal extubation could also be delayed. During surgery, all fluids and blood merchandise ought to be warmed before administration. Double-masked randomized trial evaluating alternate combos of intraoperative anesthesia and postoperative analgesia in belly aortic surgery. Surgical restore is required for a spectrum of illness, including degenerative aneurysm, acute and chronic dissection, intramural hematoma, mycotic aneurysm, pseudoaneurysm, penetrating aortic ulcer, coarctation, and traumatic aortic tear. These advances have led to significant reductions in operative mortality and perioperative issues. However, even in facilities where numerous procedures are carried out, morbidity and mortality are frequent, particularly in patients with dissecting or ruptured aneurysms. Intraoperative management requires a team effort with intimate cooperation amongst surgeons, anesthesiologists, perfusionists, nurses, and electrophysiologic monitoring staff.
Many strategies have been carried out to decrease the gap between the demand and provide impotence is a horrifying thing levitra soft 20 mg otc, including public consciousness campaigns and updates to the organ allocation system erectile dysfunction age 36 levitra soft 20 mg generic otc. Organ donation rates and the number of organs transplanted per donor differ considerably across geographic regions erectile dysfunction pills for diabetes buy 20 mg levitra soft mastercard. Per a hundred eligible deaths within the United States in 2016, the organ donation price was seventy two. Hyperglycemia 20 13 20 15 93 ninety five 97 ninety nine 01 03 05 07 09 19 11 Common living-related and living-unrelated donors is widespread in international locations with moral or legal objections to neurologic death and is a crucial worldwide donor supply. Organ transplantation is a complex process that requires close coordination amongst many specialized groups. Procurement organizations, transplant coordinators, social workers, nurses, surgeons, internists, intensivists, and anesthesiologists are involved in the process. To maximize the variety of organs transplanted and to preserve the very best function of donated organs, anesthesiologists must perceive the pathophysiologic derangements related to donation and ischemia-reperfusion injury. In addition, anesthesiologists should be conscious of the moral and legal points associated to the declaration of demise and organ donation. Although the standards for the declaration of neurologic dying had been based on moral rules established several decades in the past, the criteria stay valid right now. In reality, neurologic death has not reached a authorized status in some international locations, similar to China. The pathophysiologic mechanisms of neurologic demise have profound effects on the molecular, cellular, and tissue ranges. The scientific presentations related to neurologic demise may be complicated and vary from affected person to affected person. They can be additional difficult by prior pathologic abnormalities, illness, and therapy. The typical pathophysiologic modifications associated with neurologic death are additional described in Table 61. In 1968, a Harvard Ad Hoc Committee on Irreversible Coma established a set of criteria that has been extensively used for the determination of neurologic death. The first section is characterised by sympathetic discharge (catecholamine 61 � Anesthesia for Organ Procurement 1995 storm), which causes intense vasoconstriction or elevated systemic vascular resistance (hypertensive crisis), tachycardia, and a redistribution of blood volume with visceral ischemia. Acute myocardial injury can occur in neurologicdead donors without a historical past of coronary artery illness. After the sympathetic discharge of the primary section, the lack of sympathetic tone, decreased cardiac output, blunted hemostatic responses, and severe peripheral vasodilatation (vasoplegia) characterize the second section. Although the primary hypertensive section typically represents a transient period in the development to neurologic demise, the second hypotensive section is profound and sustained. Failure to right these cardiovascular derangements ends in poor organ perfusion and inadequate tissue oxygenation, which will threaten the viability of the donated organs. Thyroid hormonal deficiency may be just like the euthyroid sick syndrome commonly noticed in the non-neurologic injured patient with multisystem organ failure. Hyperglycemia is often encountered in neurologic-dead donors due to decreased insulin concentrations and elevated insulin resistance. Although hyperpyrexia might initially happen, hypothermia follows, which is attributable to a reduction in metabolic price and muscle exercise, together with peripheral vasodilation. Disseminated intravascular coagulation is current in up to one-third of isolated patients with head injuries and is believed to be brought on by the discharge of tissue thromboplastin from brain tissue. Kidney grafts accounted for over 95% of the organs transplanted from residing donors during this period. The resulting improve in hydrostatic strain in the pulmonary circulation causes pulmonary capillary leakage and pulmonary edema. Sympathetic exercise triggers a sterile systemic inflammatory response, initiating infiltration of neutrophils and rising pulmonary endothelial permeability, which further contributes to lung damage. Proinflammatory cytokines are launched at the alveoli and are related to early graft failure and mortality after lung transplantation. The inflammatory response in neurologic-dead donors is associated with the deterioration in cardiac perform and a shift to anaerobic metabolism. Hormonal instability can reduce alveolar fluid clearance, leading to significant accumulation of extravascular lung water. The growth of central diabetes insipidus ends in severe fluid and electrolyte derangements and could be noticed in up to 90% of neurologic-dead donors. The consideration of the withdrawal of life-sustaining therapies must be independent from any dialogue associated to transplantation. Drugs can be utilized to relieve pain and nervousness and to provide comfort for the patient throughout withdrawal. Therapies designed to improve graft quality, but with out benefit to the patient, are controversial; nonetheless, therapies with minimal influence on the affected person that improve organ survival are allowed in some protocols. Declaration of circulatory death should observe procedures proposed by national organizations and insurance policies adopted by the local institution. The length between cessation of cardiovascular activities and the declaration of circulatory death is normally 2 to 5 minutes to ensure irreversibility. The time elapsed from extubation to circulatory dying is a crucial issue for figuring out the suitability of organ donation. If spontaneous respiration and/or coronary heart function continues for a chronic period after life support withdrawal, then the organs may not be suitable for transplantation, significantly in donors with comorbidities. A low rating (8-12) signifies that breathing and/or cardiac operate will continue for some time. A uniform idea of dying, which mixes all earlier criteria for dying, is rising. Development of the University of Wisconsin Donation After Circulatory Death Evaluation Tool. As the numbers of patients waiting for transplant increase, many facilities have extended donor criteria to decrease waiting-list mortality. Many phrases, together with suboptimal donor, marginal donor, inferior donor, nonstandard donor, and high-risk donor, have been used. Maintaining adequate intravascular volume might be the most effective remedy for vasoplegia. No proof demonstrates that a particular crystalloid answer is superior to one other. Adequate resuscitation, as evidenced by a mean arterial strain of 60 to one hundred mm Hg, may decrease cytokine levels and enhance the number of organs out there for transplantation. If a large dose of dopamine is required, then a second vasoactive agent could be added. Dopamine and other catecholamines have useful antiinflammatory and immunomodulatory results. Vasopressin is recommended because the initial remedy of alternative for potential heart donors by the American College of Cardiology. For a possible coronary heart donor, cardiac perform ought to be assessed, with early interventions to improve the donor procurement rate. Echocardiography is helpful since it can determine both practical and structural abnormalities. Functional abnormalities identified in the early stage may be managed earlier than heart transplantation, whereas structural abnormalities might preclude transplantation. If not treated, these derangements can lead to graft deterioration, leading to organs unsuitable for transplantation. Myocardial damage caused by catecholamine storm could also be prevented or attenuated by controlling cardiovascular responses, which may enhance the variety of heart transplants. Fluid restriction will increase the number of lung grafts available for transplantation. The systemic inflammatory response associated with neurologic dying results in pulmonary infiltration of neutrophils and the elevation of interleukins. The systemic inflammatory response of the donor is associated with graft failure and recipient mortality. Methylprednisolone administration can moderate the inflammatory response and should improve oxygenation, scale back lung water, and improve lung yield.
The prevention of Ca++ influx inhibits the release of excitatory (pronociceptive) neurotransmitters erectile dysfunction protocol does it work 20 mg levitra soft with mastercard. A outstanding instance is the suppression of substance P release from primary sensory neurons erectile dysfunction over 60 20 mg levitra soft effective, each inside the spinal wire and from their peripheral terminals inside injured tissue erectile dysfunction oil treatment 20 mg levitra soft order otc. At the postsynaptic membrane, opioids produce hyperpolarization by opening K+ channels, thereby preventing excitation or propagation of motion potentials in second-order projection neurons. Endogenous opioid receptor ligands are derived from the precursors proopiomelanocortin (encoding -endorphin), proenkephalin (encoding Met-enkephalin and Leu-enkephalin), and prodynorphin (encoding dynorphins). These peptides include the widespread Tyr-Gly-GlyPhe-Met/Leu sequence at their amino terminals, often recognized as the opioid motif. Opioid peptides and receptors are expressed throughout the central and peripheral nervous system, in neuroendocrine tissues, and in immune cells. Both peptidases are expressed in the central nervous system, peripheral nerves, and leukocytes and, amongst opioids, enkephalins are thought-about their most popular substrates. Preventing the extracellular degradation of endogenous opioid peptides by peptidase inhibitors, each in central and peripheral compartments, has been proven to produce potent analgesic effects in many animal models and in some small human trials. Partial agonists must occupy a greater fraction of the available pool of practical receptors than full agonists to induce a response of equal magnitude. Mixed agonist/ antagonists (buprenorphine, butorphanol, nalbuphine, pentazocine) could act as agonists at low doses and as antagonists (at the identical or a different receptor type) at greater doses. Such compounds usually exhibit ceiling results for analgesia they usually might elicit an acute withdrawal syndrome when administered together with a pure agonist. Upper panel: Opioid ligands induce a conformational change at the receptor which permits coupling of G proteins to the receptor. In addition, the phospholipase C/phosphokinase C pathways can be activated (d) to modulate Ca++ channel activity within the plasma membrane (e). After arrestin binding, the receptor is in a desensitized state at the plasma membrane (a). Arrestin-bound receptors can then be internalized through a clathrin-dependent pathway, and both be recycled to the cell surface (b) or degraded in lysosomes (c). For example, tolerance to respiratory melancholy, sedation, and nausea typically develops faster than to constipation or miosis. However, many research have, actually, proven withdrawal-induced hyperalgesia, a extensively known phenomenon following the abrupt cessation of opioids. Systemically and spinally administered opioids can produce comparable side effects, relying on dosage and rostral/systemic redistribution. Adverse unwanted facet effects could be minimized by cautious dose titration and close patient monitoring, or could be treated by co-medication (antiemetics, laxatives) or opioid receptor antagonists. In addition, habit has been reported in excessive numbers of sufferers handled with opioids for continual ache, and overdoses, demise charges, and abuse of prescription opioids have become a public well being downside. Subsequently, nociceptors turn out to be much less aware of noxious stimuli and spinal neurotransmission is attenuated. Over-the-counter availability and self-medication have led to frequent abuse and toxicity. Within the dorsal horn of the spinal twine serotoninergic neurons contribute to endogenous ache inhibition. These mechanisms facilitate the era of impulses inside nociceptors and their transmission by way of the spinal wire to greater mind areas. Neuropathic syndromes have been attributed to ectopic activity in sensitized nociceptors from regenerating nerve sprouts, recruitment of previously "silent" nociceptors, or spontaneous neuronal exercise (or any mixture of these processes). These events could result in sensitization of primary afferents and subsequent sensitization of secondand third-order ascending neurons. Among one of the best studied mechanisms are the elevated expression and trafficking of ion channels. The mechanisms of action of antiepileptics embody neuronal membrane stabilization by blockage of pathologically active voltagesensitive Na+ channels. The most common adverse results are impaired mental (somnolence, dizziness, cognitive impairment, fatigue) and motor (ataxia) operate, which limit medical use, notably in elderly sufferers. Other severe unwanted effects have been reported, together with hepatotoxicity, thrombocytopenia, dermatologic and hematologic reactions. The reuptake block results in a stimulation of endogenous monoaminergic pain inhibition within the spinal twine and brain. Adverse events of antidepressants embrace sedation, nausea, dry mouth, constipation, dizziness, sleep disturbance, and blurred vision. This is perceived as a burning or itching sensation with a flare response and occurs in a excessive number of sufferers. Another potential mechanism is a direct toxic impact on smalldiameter sensory nerve fibers. Topical capsaicin was shown to provide pain relief in postherpetic neuralgia, postmastectomy syndrome, osteoarthritis, and quite lots of neuropathic syndromes. Blockade of Na+ channels reduces impulse generation each in normal and in damaged sensory neurons. Such neurons exhibit spontaneous and ectopic firing, presumably contributing to sure situations of persistent neuropathic pain. Under these circumstances the altered expression, distribution, and performance of ion channels alongside axons is associated with elevated sensitivity to local anesthetics. Thus, pain reduction may be achieved with local anesthetic concentrations lower than those who completely block impulse conduction. All of those mechanisms result in analgesia or antiinflammatory results (or both). Metaanalyses indicate that local anesthetics produce moderate analgesic effects of questionable clinical significance in neuropathic pain. Thus, like opioids, 2-agonists scale back neurotransmitter launch and reduce postsynaptic transmission, leading to an total inhibitory impact. Cannabinoids have been studied extensively and are at present within the focus of public curiosity. Animal and in vitro fashions have shown that derivatives of tetrahydrocannabinol produce antinociceptive results and that cannabinoid receptors and their endogenous ligands are expressed in pain-processing areas of the mind, spinal cord, and periphery. Psychotropic unwanted side effects, sedation, dizziness, cognitive impairment, nausea, dry mouth, and motor deficits are limiting factors in scientific apply. In some reviews it was discovered to exhibit analgesic effects in trigeminal neuralgia and central neuropathic ache. The commonest side effects are drowsiness, dizziness, and gastrointestinal misery. The use of botulinum toxin injections has produced inconsistent ends in headaches and was not efficient in myofascial set off points, orofacial, or neck pain. The synthetic peptide ziconotide blocks N-type voltagesensitive Ca++ channels and thereby inhibits release of excitatory neurotransmitters from central terminals of major afferent neurons within the spinal cord. It has been permitted for intrathecal utility however produces substantial unwanted aspect effects (dizziness, confusion, irregular gait, reminiscence impairment, nystagmus, hallucinations, vertigo, delirium, apnea, hypotension) and, thus, is suitable for only a small subset of sufferers with in any other case intractable ache. Antiemetics are used to deal with nausea, a frequent side effect of analgesics (particularly opioids) and a frequent grievance in cancer patients. For example, in cancer sufferers, etiologies aside from opioids have to be considered, similar to radiotherapy and chemotherapy, uremia, hypercalcemia, bowel obstruction, and increased intracranial pressure. Management tips for the therapy of nausea and vomiting can be found and the choice of antiemetics must be mechanism-based. Most suggestions for the selection of antiemetic medicine embrace gastrointestinal prokinetics (metoclopramide), phenothiazines. Risk components for constipation embody opioid medication, older age, superior most cancers, hypokalemia, immobilization, as properly as remedy with tricyclics, phenothiazines, anticonvulsants, diuretics, and iron supplements. Opioid-related constipation is mediated through intestinal and (partially) through central -receptors. Ample fluid consumption, fiber-rich nutrition, and mobilization are nonpharmacologic approaches to prophylaxis, but suggestions are principally derived from anecdotal proof. Recommendations usually embody lactulose, senna, or polyethylene glycol fifty one � Management of the Patient With Chronic Pain 1615 as a primary choice. If insufficient, the drugs of first choice could additionally be combined with paraffin or anthraglycosides (bisacodyl). Rectal sorbitol or contrast medium are the choices for the next more intensified step.
Do not attempt to erectile dysfunction treatment brisbane cheap levitra soft 20 mg mastercard clear up a chronic ache downside in the instant postoperative period erectile dysfunction pills wiki levitra soft 20 mg trusted. Use non-pharmacological strategies (distraction erectile dysfunction doctor in kolkata levitra soft 20 mg purchase line, relaxation) the place appropriate and provide counselling within the pain unit after postoperative restoration. Pain: moving from symptom management towards mechanism-specific pharmacologic management. Opioids from immunocytes work together with receptors on sensory nerves to inhibit nociception in inflammation. Modulation of peripheral sensory neurons by the immune system: implications for ache therapy. Mycobacteria attenuate nociceptive responses by formyl peptide receptor triggered opioid peptide launch from neutrophils. Beta-endorphin, Metenkephalin and corresponding opioid receptors within synovium of sufferers with joint trauma, osteoarthritis and rheumatoid arthritis. Involvement of intraarticular corticotropin-releasing hormone in postoperative ache modulation. Arthritic inflammation in rats as a mannequin of persistent pain: role of opioid systems. Brain imaging exams for chronic ache: medical, authorized and moral points and recommendations. Codeine and opioid metabolism: implications and alternatives for pediatric ache administration. Analgesia and opioids: a pharmacogenetics shortlist for implementation in medical practice. Practice pointers for continual ache management: an updated report by the American Society of Anesthesiologists task drive on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine. Chronic illnesses in the European Union: the prevalence and health cost implications of persistent pain. Multimodal pain remedy in persistent noncancer pain-gold commonplace or want for further clarification The position of the medical health insurance trade in perpetuating suboptimal ache administration. Evidence-based scientific information documenting the therapy and cost-effectiveness of complete pain programs for continual nonmalignant pain. Beyond the needle: increasing the function of anesthesiologists within the management of persistent non-malignant ache. Acceptance and values-based motion in continual ache: a three-year follow-up evaluation of treatment effectiveness and process. Systematic review to determine which validated measurement instruments can be utilized to assess risk of problematic analgesic use in patients with chronic ache. Multidisciplinary biopsychosocial rehabilitation for continual low again pain: Cochrane systematic review and meta-analysis. Improved high quality of life, working capability, and patient satisfaction after a pretreatment multimodal assessment method in sufferers with combined chronic muscular pain: a randomized-controlled study. Physical conditioning packages for enhancing work outcomes in workers with again pain. Placebo analgesia and beyond: a melting pot of concepts and ideas for neuroscience. Regulation of mu-opioid receptors: desensitization, phosphorylation, internalization, and tolerance. Inhibiting the breakdown of endogenous opioids and cannabinoids to alleviate pain. Pain inhibition by blocking leukocytic and neuronal opioid peptidases in peripheral inflamed tissue. Progress in understanding mechanisms of opioid-induced gastrointestinal antagonistic effects and respiratory despair. Opioid unwanted side effects and their therapy in sufferers with persistent most cancers and noncancer ache. Immunosuppressive elements of analgesics and sedatives used in mechanically ventilated sufferers: an underappreciated danger issue for the development of ventilator-associated pneumonia in critically sick sufferers. Precipitated opioid withdrawal across acute physical dependence induction strategies. Perioperative and intraoperative pain and anesthetic care of the continual pain and cancer pain patient receiving persistent opioid remedy. MorphiDex (morphine sulfate/dextromethorphan hydrobromide combination) in the therapy of persistent pain: three multicenter, randomized, doubleblind, controlled scientific trials fail to reveal enhanced opioid analgesia or reduction in tolerance. Defining clinical points around tolerance, hyperalgesia, and habit: a quantitative and qualitative outcome examine of long-term opioid dosing in a persistent pain apply. Opioid withdrawal will increase transient receptor potential vanilloid 1 activity in a protein kinase A-dependent method. Gradual withdrawal of remifentanil infusion may forestall opioidinduced hyperalgesia. Strategies for making analgesia safer: the position of comparative effectiveness research. Side results associated with present and prospective antimigraine pharmacotherapies. Pharmacotherapy for neuropathic ache in adults: a scientific evaluation and meta-analysis. Topical analgesics for acute and chronic ache in adults - an overview of Cochrane Reviews. How are topical opioids used to handle painful cutaneous lesions in palliative care Inflammation of the rat paw enhances axonal transport of opioid receptors within the sciatic nerve and will increase their density in the inflamed tissue. Painful inflammation-induced enhance in mu-opioid receptor binding and G-protein coupling in main afferent neurons. Modulation of tight junction proteins in the perineurium to facilitate peripheral opioid analgesia. Analgesic efficacy of peripheral opioids (all except intra-articular): a qualitative systematic evaluate of randomised managed trials. Leukocyte opioid receptors mediate analgesia through Ca(2+)-regulated release of opioid peptides. Increased numbers of opioid expressing inflammatory cells do not affect intra-articular morphine analgesia. Single-dose intra-articular morphine after arthroscopic knee surgical procedure: a meta-analysis of randomized placebo-controlled studies. Arthroscopy: the journal of arthroscopic & associated surgery official publication of the Arthroscopy Association of North America and the International Arthroscopy Association. Botulinum toxin intramuscular injections for neck pain: a systematic evaluate and metaanalysis. Efficacy of remedies for opioid-induced constipation: a scientific review and meta-analysis. A nontoxic pain killer designed by modeling of pathological receptor conformations. Pathogenesis, prognosis, and remedy of lumbar zygapophysial (facet) joint pain. A systematic analysis of the therapeutic effectiveness of sacroiliac joint interventions. Diagnostic accuracy of thoracic facet joint nerve blocks: an replace of the evaluation of evidence. Interventional therapy of cancer pain: the fourth step in the World Health Organization analgesic ladder Phenol saddle blocks for intractable ache at end of life: report of 4 circumstances and literature evaluate. A new catheter technique for thoracic subarachnoid neurolysis in superior lung most cancers patients. A systematic evaluation of therapeutic side joint interventions in chronic spinal ache. The role of thoracic medial branch blocks in managing continual mid and upper back pain: a randomized, double-blind, active-control trial with a 2-year followup. Systematic review of the effectiveness of cervical epidurals in the administration of persistent neck ache.
Cambogia gummi-guta (Garcinia). Levitra Soft.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96794
Intractable ache mixed with analgesic tolerance erectile dysfunction doctors minneapolis levitra soft 20 mg discount visa, steroid use inflicting centripetal obesity erectile dysfunction treatment atlanta ga levitra soft 20 mg buy without prescription, and the unwanted facet effects of other chemotherapeutic brokers may be complicating components erectile dysfunction treatment new drugs 20 mg levitra soft order. Blood strain might lower abruptly when the ventricle is first cannulated (as brainstem stress is relieved). Unlike the vast majority of neurosurgical patients, shunt patients are often nursed flat after their procedures in an try to prevent an excessively speedy collapse of the ventricular system. The related electrophysiologic monitoring techniques are described in Chapter 39. This arises most frequently within the setting of cervical spinal stenosis and should be assumed to be present with fracture dislocation of the spinal column. For these sufferers, we place arterial catheters and assist blood pressure carefully. Blood strain assist is much less important when the issue is nerve root quite than spinal wire compression. The presence of spinal stenosis and continual wire compression is frequently, however not invariably, related to lower extremity hyperreflexia and ankle clonus. Cerebral blood quantity is increased in canines during administration of nitrous oxide or isoflurane. Defasciculation with metocurine prevents succinylcholine-induced will increase in intracranial strain. High-dose barbiturate management of elevated intracranial stress in patients with severe head harm. Metabolic acidosis, rhabdomyolysis, and cardiovascular collapse after prolonged propofol infusion. Efficacy of hyperventilation, blood pressure elevation, and metabolic suppression therapy in controlling intracranial stress after head injury. Cerebral carbohydrate metabolism of man throughout respiratory and etabolic alkalosis. Alterations in cerebral blood flow and oxygen consumption throughout prolonged hypocarbia. The electroencephalogram of awake man throughout hyperventilation: results of oxygen at three atmospheres (absolute) strain. Effect of hyperventilation on cerebral blood move in traumatic head damage: clinical relevance and monitoring correlates*. Hyperventilation following head damage: impact on ischemic burden and cerebral oxidative metabolism*. Characterization of cerebral hemodynamic phases following extreme head trauma: hypoperfusion, hyperemia, and vasospasm. Serial transcranial Doppler measurements in traumatic brain injury with particular give attention to the early posttraumatic period. Does acute hyperventilation provoke cerebral oligaemia in comatose patients after acute head harm Cerebral circulation and metabolism after severe traumatic mind damage: the elusive position of ischemia. A critique of the intraoperative use of jugular venous bulb catheters during neurosurgical procedures. Retraction mind ischaemia: cerebral blood circulate, evoked potentials, hypotension and hyperventilation in a new animal model. Local adjustments in cerebral vitality metabolism as a end result of mind retraction throughout routine neurosurgical procedures. Effect of steroids on iopamidol blood-brain transfer constant and plasma quantity in brain tumors measured with X-ray computed tomography. Dexamethasone and enhancing solitary cerebral mass lesions: alterations in perfusion and blood-tumor barrier kinetics proven by magnetic resonance imaging. Effects of mannitol and steroid therapy on intracranial volume-pressure relationships in sufferers. Furosemide- and mannitol-induced modifications in intracranial stress and serum osmolality and electrolytes. A prospective randomized trial of the optimum dose of mannitol for intraoperative mind relaxation in sufferers undergoing craniotomy for supratentorial mind tumor resection. Pharmacokinetics and results of mannitol on hemodynamics, blood and cerebrospinal fluid electrolytes, and osmolality during intracranial surgery. Use of hypertonic saline solutions in therapy of cerebral edema and intracranial hypertension. Equimolar doses of mannitol and hypertonic saline within the remedy of elevated intracranial pressure*. Use of hypertonic saline in the treatment of extreme refractory posttraumatic intracranial hypertension in pediatric traumatic brain injury. Hypertonic saline answer for management of elevated intracranial stress in patients with exhausted response to mannitol and barbiturates. Hyperosmolar brokers in neurosurgical follow: the evolving position of hypertonic saline. Hypertonic saline, not mannitol, should be thought of gold-standard medical remedy for intracranial hypertension. Hypertonic saline for treating raised intracranial stress: literature evaluate with meta-analysis. Treatment of vasogenic mind edema with the novel Cl- transport inhibitor torasemide. Contribution of anion transporters to the acidosis-induced swelling and intracellular acidification of glial cells. Characterization of perioperative seizures and epilepsy following aneurysmal subarachnoid hemorrhage. Reduced threat of venous thromboembolism with using intermittent pneumatic compression after craniotomy: a randomized managed potential research. Venous air embolism during lumbar laminectomy within the inclined place: report of three instances. Cardiac arrest during surgery and air flow within the inclined position: a case report and systematic review. Venous air embolism in sitting and supine sufferers present process vestibular schwannoma resection. Cardiovascular responses within the seated position-impact of four anesthetic methods. Hypothesis: the etiology of midcervical quadriplegia after operation with the affected person within the sitting place. Nitrous oxide withdrawal reduces intracranial pressure within the presence of pneumocephalus. Tension pneumocephalus after posterior fossa craniotomy: report of 4 additional cases and review of postoperative pneumocephalus. Tension pneumocephalus following transsphenoid surgical procedure for pituitary adenoma-report of two cases. Evaluation of an ultrasonic system (Doppler) for the prognosis of venous air embolism. Use of a pulmonary-artery catheter for detection and treatment of venous air embolism. Sitting position for neurosurgery: experience with preoperative distinction echocardiography in 301 patients. Venous air embolism during endoscopic strip craniectomy for restore of craniosynostosis in infants. Venous air embolism throughout awake craniotomy for deep mind stimulation electrode implantation. Precordial Doppler probe placement for optimal detection of venous air embolism throughout craniotomy. A comparability of the sensitivity of pulmonary artery strain, end-tidal carbon dioxide, and end-tidal nitrogen in the detection of venous air embolism within the dog. Placement of a proper atrial air aspiration catheter guided by transesophageal echocardiography. Incidence and measurement of patent foramen ovale during the first 10 many years of life: an post-mortem examine of 965 normal hearts. Incidence of venous and paradoxical air embolism in neurosurgical sufferers in the sitting place: detection by transesophageal echocardiography. Neurosurgical operations with the patient in sitting place: analysis of risk factors utilizing transcranial Doppler sonography. Transesophageal echocardiography as a information for patient positioning before neurosurgical procedures in semi-sitting place.
Syndromes
Despite deep vein thrombosis prophylaxis therapy in the perioperative interval erectile dysfunction doctor manila levitra soft 20 mg generic on line, sufferers can even present postoperatively with deep vein thrombosis or pulmonary embolism and require an anesthetic for placement of an inferior vena cava filter gadget erectile dysfunction increases with age purchase levitra soft 20 mg visa. As mentioned earlier impotence age 45 levitra soft 20 mg buy overnight delivery, prophylactic filters are often placed prior to bariatric surgery. Specific attention should be paid to the documentation of affected person place and technique employed for airway administration in the prior anesthetic. Patients may be hypovolemic from blood loss, insufficient hydration, vasodilatation, and insensible fluid losses related to fever and infection. It is especially important to contemplate further or new dangers of aspiration of gastric contents. Decompression of the gastric pouch in sufferers going for surgical procedure to relieve a small bowel obstruction could be achieved with careful introduction of a nasogastric or orogastric tube simply prior to induction of general anesthesia. Although this may increase the chance of violating a recent, competent anastomotic suture line, communication between anesthesiologist and surgeon could be pursued to decide the risks and advantages of performing this maneuver. During the following laparotomy, any perforation of a recent suture line resulting from the attempt to decompress the gastrointestinal tract can be repaired immediately and the nasogastric or orogastric tube can subsequently be left in place for continued postoperative drainage. Depending on the extent of reoperation, requirement for volume resuscitation, blood transfusion, degree of peritonitis with anastomotic leak, presence of sepsis, or other important continued risks to health, patients present process reoperation may require prolonged postoperative ventilation. Requirements for postoperative pain management may also be significantly completely different than those related to the preliminary bariatric procedure. This is particularly useful in overweight patients undergoing laparotomy, as is described elsewhere on this chapter. There are also a quantity of potential main complications requiring surgical intervention weeks, months, or even years after a bariatric surgical operation has been carried out. Patients could develop anastomotic strictures or ulcers, ventral hernias, gastrogastric fistulae, and severe reflux problems requiring additional surgery. The anesthetic concerns for such patients ought to include a evaluation of the prior anesthetic record to glean info regarding airway and ache administration. The nutritional and metabolic issues of bariatric surgical procedure also include protein and protein-calorie malnutrition. Patients could have extreme weight loss occurring both too rapidly or past the predetermined targets, steatorrhea or extreme diarrhea, hypoalbuminemia, marasmus, edema, and hyperphagia. Surgical revision may be required to appropriate excessive weight loss and hypoalbuminemia. Under such circumstances, an anesthetic regimen accounting for decreased drug binding results of a low serum albumin must be considered. Considerations for Management of the Obese Patient Presenting for Nonbariatric Surgery Few research have evaluated the significance of morbidity when performing common nonbariatric surgical fifty eight � Anesthesia for Bariatric Surgery 1927 procedures on the overweight affected person. They discovered no variations in the kind of postoperative problems in overweight and nonobese teams. This examine supplies knowledge to decrease the prejudice that sufferers with weight problems are implied to have the next incidence of postoperative complications. This preconception might pertain extra to the perception of the medical team on account of technical difficulties on the anesthetic and surgical finish. Surgeries may last longer, about 25% extra time for laparoscopic than for open cholecystectomy within the morbidly overweight. Significantly, the wound infection price was much better after laparoscopic than after open surgical procedure, which supports the follow of performing laparoscopic surgery in overweight patients somewhat than the choice. Prevalence of overweight, weight problems, and extreme obesity amongst adults aged 20 and over: United States, 1960� 1962 Through 2011�2014. Prevalence of Overweight and Obesity Among Children and Adolescents Aged 2�19 Years: United States, 1963�1965 Through 2013�2014. Prevalence of overweight, obesity, and excessive weight problems among adults aged 20 and over: United States, 1960�1962 Through 2011�2014. Trends in weight problems prevalence amongst kids and adolescents in the United States, 19881994 through 2013-2014. Mechanisms of restoration from type 2 diabetes after malabsorptive bariatric surgery. Predictors of weight reduction and reversal of comorbidities in malabsorptive bariatric surgical procedure. Prevalence of metabolic syndrome among adults 20 years of age and over, by sex, age, race and ethnicity, and body mass index: United States, 2003-2006. Metabolic syndrome: a extra in-depth take a look at the rising epidemic and its associated pathologies. Anesthetic administration of a affected person with obstructive sleep apnea syndrome and troublesome airway entry. Relationship between body mass index, age and upper airway measurements in snorers and sleep apnoea sufferers. Obstructive sleep apnea in the adult obese patient: implications for airway management. Obesity and inflammation: change in cdiponectin, C-reactive protein, tumour necrosis factor-Alpha and Interleukin-6 after bariatric surgical procedure. Ghrelin and obestatin levels in severely overweight women before and after weight loss after Roux-en-Y gastric bypass surgical procedure. An herbal supplement containing ma huang-guarana for weight reduction: a randomized, double-blind trial. Herbal ephedra/caffeine for weight loss: a 6-month randomized safety and efficacy trial. The effect and safety of an ephedrine/caffeine compound in comparability with ephedrine, caffeine and placebo in overweight subjects on an energy restricted diet. Adverse cardiovascular and central nervous system events related to dietary dietary supplements containing ephedra alkaloids. Long-term follow-up of gastric stimulation for obesity: the Mestre 8-year expertise. Updates on gastric electrical stimulation to treat obesity: systematic review and future views. Prevalence of chubby and weight problems among children and adolescents aged 2�19 years: United States, 1963�1965 by way of 2013�2014. Prevalence and trends of chubby amongst preschool kids in creating nations. Bariatric surgery in adolescents: latest nationwide developments in use and in-hospital end result. Surgery decreases longterm mortality, morbidity, and well being care use in morbidly overweight sufferers. Insulin resistance in nondiabetic morbidly obese patients: effect of bariatric surgery. Bariatric surgical procedure for morbid weight problems: health implications for patients, well being professionals, and thirdparty payers. Bariatric surgical procedure: a promising resolution for nonalcoholic steatohepatitis in the very obese. Laparoscopic gastric bypass is superior to laparoscopic gastric banding for therapy of morbid obesity. Laparoscopic adjustable gastric band versus laparoscopic Roux-en-Y gastric bypass: ends justify the means Effect of Roux-en-Y gastric bypass vs sleeve gastrectomy on glucose and intestine hormones: a prospective randomised trial. Preliminary surgical results of single-incision transumbilical laparoscopic bariatric surgical procedure. Intragastric balloon for treatmentresistant weight problems: safety, tolerance, and efficacy of 1-year balloon treatment adopted by a 1-year balloon-free follow-up. Balancing danger and reward: a critical evaluate of the intragastric balloon for weight loss. Percutaneous gastrostomy gadget for the treatment of class ii and sophistication iii obesity: outcomes of a randomized controlled trial. Bariatric surgical procedure for the therapy of morbid weight problems: a meta-analysis of weight reduction outcomes for laparoscopic adjustable gastric banding and laparoscopic gastric bypass. A evaluate of studies comparing three laparoscopic procedures in bariatric surgical procedure: sleeve gastrectomy, Roux-en-Y gastric bypass and adjustable gastric banding.
Perioperative microembolization is more common in women and patients with symptomatic carotid disease erectile dysfunction age 55 20 mg levitra soft generic fast delivery. Additionally erectile dysfunction meds at gnc 20 mg levitra soft cheap mastercard, the high rate of technical failures considerably limits the clinical utility of this monitoring modality erectile dysfunction pills from china levitra soft 20 mg buy line. Such monitoring permits willpower of the arterial-jugular venous O2 content material distinction and jugular venous O2 saturation and due to this fact provides information on world cerebral O2 metabolism. Jugular venous samples are obtained from a catheter inserted into the jugular bulb ipsilateral to the surgical site. Significant technical and methodologic shortcomings have restricted the clinical software of this monitoring during carotid endarterectomy. Near-infrared spectrophotometry is a noninvasive technique that permits continuous monitoring of regional cerebral O2 saturation via the scalp and cranium. Similar to pulse oximetry, cerebral oximetry is based on the different absorption characteristics of the near-infrared spectrum of oxygenated and deoxygenated hemoglobin. However, unlike pulse oximeters, cerebral oximeters measure the O2 saturation of hemoglobin in the entire tissue bed. A commercially obtainable cerebral oximetry sensor is applied to the brow skin ipsilateral to the surgical website, and regional cerebral O2 saturation from a small pattern of the frontal cortex below the sensor is supplied. To date, broad patient-to-patient variability in baseline cerebral O2 saturation and the shortage of a clinical threshold of a lower in cerebral O2 saturation predictive of the need for shunt placement have impeded the widespread use of this novel monitoring modality. It is mostly accepted that the majority neurologic problems are associated to surgical method. Thromboembolic (rather than hemodynamic) elements appear to be the major mechanism of perioperative neurologic issues and most happen within the postoperative interval. Neurologic problems attributable to carotid artery thrombosis could occur with an incidence as frequent as 3. Other necessary, but less widespread neurologic complications include intracerebral hemorrhage and cerebral hyperperfusion. The reported incidence of intracerebral hemorrhage after carotid endarterectomy ranges from 0. Most intracerebral hemorrhages happen 1 to 5 days after the operation and are associated with significant morbidity and mortality. Not surprisingly, patients with poorly controlled preoperative hypertension typically have severe hypertension postoperatively. Because neurologic and cardiac problems could also be related to postoperative hypertension, blood strain must be aggressively controlled to close to preoperative values after surgery. Postoperative cerebral hyperperfusion syndrome is an abrupt enhance in blood flow with loss of autoregulation in the surgically reperfused brain and is manifested as headache, seizure, focal neurologic indicators, mind edema, and probably intracerebral hemorrhage. Unfortunately, little is definitely known about the cause and administration of this syndrome. Patients with severe postoperative hypertension and severe preoperative inner carotid artery stenosis are believed to be at increased threat for this syndrome. Carotid sinus baroreceptor hypersensitivity or reactivation most likely plays an necessary function. To avoid cerebral and myocardial ischemia, hypotension must be corrected promptly. Cardiac output is frequently normal or elevated and systemic vascular resistance lowered in hypotensive sufferers after carotid endarterectomy. Intensive surveillance for proof of myocardial and cerebral ischemia and even handed use of fluids and vasopressors are really helpful for postoperative hypotension. Cranial and cervical nerve dysfunction after carotid endarterectomy is properly documented in the literature. Although most injuries are transient, permanent injuries can result in vital disability. Patients must be examined for harm to the recurrent laryngeal, superior laryngeal, hypoglossal, and marginal mandibular nerves shortly after extubation. Unilateral recurrent laryngeal nerve injury may lead to ipsilateral true vocal twine paralysis within the paramedian position. Although most sufferers have hoarseness and an impaired cough mechanism, the damage is usually well tolerated. However, bilateral recurrent laryngeal nerve damage and resultant bilateral vocal wire paralysis can result in lifethreatening upper airway obstruction. Carotid body denervation might happen after carotid endarterectomy as a result of surgical manipulation. In this example, the central chemoreceptors are the primary sensors for maintaining ventilation, and critical respiratory melancholy might outcome from opioid administration. Fortunately, most patients require little more than acetaminophen or ketorolac for postoperative pain. Most instances are the outcomes of venous oozing and require little more than exterior compression for five to 10 minutes. Expanding hematomas require immediate evaluation on the bedside and immediate evacuation if airway compromise is evident. Aggressive postoperative blood pressure control might help cut back the incidence of hematoma. I suppose all sufferers ought to be monitored in an intensive care setting for a minimal of 8 hours after carotid endarterectomy, because most occasions requiring intervention happen inside this timeframe. Significant procedural advancements embrace using twin antiplatelet remedy, self-expanding stents, and emboli protection units. Over the last decade, main randomized clinical trials evaluating carotid endarterectomy with carotid artery stenting have been printed. A latest systematic review of randomized trials (16 trials involving 7572 patients) discovered that endovascular remedy (including balloon angioplasty or stenting) was associated with an elevated threat for periprocedural stroke or dying compared with endarterectomy. The fee of ipsilateral stroke after the periprocedural period was not different between treatment groups. Updated tips provide specific recommendations for revascularization of symptomatic and asymptomatic sufferers. The femoral artery method is considered standard, but brachial artery and high radial artery access have been reported with excessive procedural success. Embolic safety units are considered mandatory and include distal safety within the form of a filter or occlusion balloon and proximal protection in the form of move interruption or flow reversal. Cardiologists and radiologists currently carry out a large share of those procedures in specialized endovascular suites. In addition to routine displays, an arterial line is positioned for steady blood pressure monitoring. Some degree of hemodynamic instability is frequent in patients throughout and after carotid artery stenting. Bradycardia and hypotension occur rather more incessantly after carotid artery stenting with balloon angioplasty than without angioplasty. The administration of prophylactic atropine earlier than balloon inflation decreases the incidence of intraoperative bradycardia and cardiac morbidity in major carotid stenting sufferers. It is assumed that 30% of sufferers could also be pharmacogenetically proof against clopidogrel. While common anesthesia is normally used for open peripheral revascularization surgical procedures, regional and neuraxial anesthesia could additionally be employed. What is totally different in these instances is that the percutaneous access could presumably be affected by the disease process, for instance, frequent femoral stenosis, which can want an open cutdown or even a combined widespread femoral endarterectomy before stenting the distal arteries. If this is the cases the alternatives for anesthesia will be restricted to either common anesthesia or neuraxial anesthesia. Norris for contributing a chapter on this subject to the prior edition of this work. The prevalence and prognosis of unrecognized myocardial infarction and silent myocardial ischemia in patients undergoing major vascular surgical procedure. The prevalence of treatable left ventricular systolic dysfunction in patients who present with noncardiac vascular episodes: a case-control examine. Frequency and significance of early postoperative silent myocardial ischemia in patients having peripheral vascular surgery. Long-term prognosis of myocardial ischemia detected by Holter monitoring in peripheral vascular disease. Cardiac end result after peripheral vascular surgery: comparability of basic and regional anesthesia. The worth of silent myocardial ischemia monitoring in the prediction of perioperative myocardial infarction in sufferers undergoing peripheral vascular surgical procedure.
Appropriate length of epidural catheter within the epidural area for postoperative analgesia: evaluation by epidurography erectile dysfunction drugs in pakistan 20 mg levitra soft discount visa. The optimum distance that a multiorifice epidural catheter must be threaded into the epidural house erectile dysfunction needle injection generic levitra soft 20 mg on line. The effect of the Lockit epidural catheter clamp on epidural migration: a controlled trial erectile dysfunction at the age of 21 levitra soft 20 mg generic on-line. Subcutaneous tunnelling of epidural catheters for postoperative analgesia to stop accidental dislodgement: a randomized controlled trial. Combined spinal-epidural anesthesia utilizing epidural quantity extension leads to quicker motor recovery after elective cesarean delivery: a prospective, randomized, double-blind research. Low dose of intrathecal hyperbaric bupivacaine mixed with epidural lidocaine for cesarean section� a steadiness block technique. Paraesthesiae throughout needle-throughneedle combined spinal epidural versus single-shot spinal for elective caesarean section. A scientific comparison between needle-through-needle and double-segment methods for combined spinal and epidural anesthesia. Ultrasound evaluation of cranial spread throughout caudal blockade in youngsters: the impact of different volumes of native anaesthetics. Neurological issues after regional anesthesia: contemporary estimates of threat. Paraplegia from spinal twine damage after thoracic epidural catheterization performed under basic anesthesia. Spinal cord harm in a toddler brought on by an accidental dural puncture with a single-shot thoracic epidural needle. Anterior spinal artery syndrome after epidural anesthesia in a pregnant diabetic patient with scleroderma. Anterior spinal artery syndrome following total hip arthroplasty beneath epidural anaesthesia. Cauda equina syndrome following a single spinal administration of 5% hyperbaric lidocaine through a 25-gauge Whitacre needle. Persistent sacral sensory deficit induced by intrathecal native anesthetic infusion within the rat. Continuous spinal microcatheter (28 gauge) approach for arterial bypass surgery of the lower extremities and comparability of ropivacaine with or with out morphine for postoperative analgesia. Severe neurological problems after central neuraxial blockades in Sweden 1990�1999. Incidence of epidural hematoma, infection, and neurologic harm in obstetric patients with epidural analgesia/anesthesia. Small danger of significant neurologic problems related to lumbar epidural catheter placement in anesthetized patients. Serious complications related to regional anesthesia: outcomes of a potential survey in France. Incidence of neurologic issues related to thoracic epidural catheterization. Severe complications associated with epidural and spinal anaesthesias in Finland 1987-1993, A study based mostly on affected person insurance claims [see comment]. Serious complications associated with epidural/spinal blockade in obstetrics: a two-year prospective research. Injuries associated with regional anesthesia in the Eighties and Nineteen Nineties: a closed claims evaluation. Long-term follow-up of sufferers who obtained 10,098 spinal anesthetics; syndrome of decreased intracranial pressure (headache and ocular and auditory difficulties). Postspinal headache and relationship of needle bevel to longitudinal dural fibers. Effects of the serotoninreceptor agonist sumatriptan on postdural puncture headache: report of six instances. Effectiveness of epidural blood patch in the administration of post-dural puncture headache. Efficacy of a prophylactic epidural blood patch in stopping submit dural puncture headache in parturients after inadvertent dural puncture. Epidural blood patch: evaluation of the quantity and unfold of blood injected into the epidural house. Magnetic resonance imaging of extradural blood patches: appearances from 30 min to 18 h. Transient radicular irritation after spinal anaesthesia with hyperbaric 5% lignocaine. Transient neurological symptoms after spinal anaesthesia with levobupivacaine 5 mg/ml or lidocaine 20 mg/ml. Transient neurological symptoms after isobaric subarachnoid anesthesia with 2% lidocaine: the influence of needle kind. The incidence and danger factors for hypotension after spinal anesthesia induction: an evaluation with automated knowledge collection. Fluid and vasopressor management for cesarean delivery under spinal anesthesia: continuing professional development. Severe bradycardia throughout spinal and epidural anesthesia recorded by an anesthesia info management system. Bradycardia and asystole during spinal anesthesia: a report of three instances without morbidity. Practice tips for the perioperative management of patients with obstructive sleep apnea: a report by the American Society of Anesthesiologists Task Force on Perioperative Management of Patients with Obstructive Sleep Apnea. Practice pointers for the prevention, detection, and administration of respiratory despair related to neuraxial opioid administration. Incidence of spinal epidural abscess after epidural analgesia: a national 1-year survey. Infectious risks of persistent pain remedies: injection therapy, surgical implants, and intradiscal methods. The impression of intrapartum analgesia on labour and supply outcomes in nulliparous girls. The results of spinal anesthesia with lidocaine and sufentanil on lower urinary tract capabilities. Parameters affecting urologic complications after major joint alternative surgery. Thermoregulatory effects of spinal and epidural anesthesia throughout cesarean supply. Hemodynamic responses to intravascular injection of epinephrinecontaining epidural check doses in adults throughout basic anesthesia. The effects of single and fractionated doses of mepivacaine on the extent of thoracic epidural block. The dorsomedian connective tissue band in the lumbar epidural area of humans: an anatomical examine utilizing epiduroscopy in post-mortem circumstances. The lumbar subdural extraarachnoid space of people: an anatomical research using spinaloscopy in post-mortem instances. Neuraxial and combined neuraxial/general anesthesia in comparison with common anesthesia for major truncal and decrease limb surgical procedure: a scientific review and metaanalysis. Anesthesia technique and mortality after complete hip or knee arthroplasty: a retrospective, propensity score-matched cohort examine. Epidural analgesia improves end result in cardiac surgical procedure: a meta-analysis of randomized controlled trials. Protective results of epidural analgesia on pulmonary issues after abdominal and thoracic surgical procedure: a meta-analysis. Effect of postoperative epidural analgesia on morbidity and mortality after lung resection in Medicare sufferers. Comparative perioperative outcomes associated with neuraxial versus common anesthesia for simultaneous bilateral whole knee arthroplasty. Cancer recurrence after surgery: direct and indirect results of anesthetic brokers. Anesthetic method for radical prostatectomy surgical procedure affects most cancers recurrence: a retrospective evaluation. Potential affect of the anesthetic method used throughout open radical prostatectomy on prostate cancer-related end result: a retrospective study. Reduction in mortality after epidural anaesthesia and analgesia in sufferers present process rectal however not colonic most cancers surgery: a retrospective analysis of knowledge from 655 patients in central Sweden.






