Ciloxan
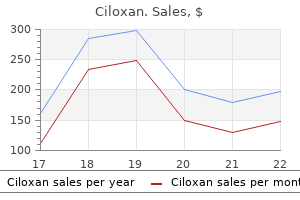
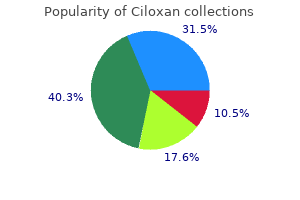
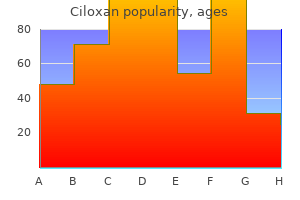
Ciloxan
Ciloxan dosages: 1000 mg, 750 mg, 500 mg, 250 mg
Ciloxan packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

As long as 4�6 years after therapy antibiotic h49 purchase ciloxan 250 mg with visa, about 8�13% of the teeth should appear therapeutic (�rstavik 1996; Farzaneh et al virus coxsackie cheap ciloxan 250 mg free shipping. Considering the somewhat prolonged timecourse of therapeutic treatment for uti breastfeeding 1000 mg ciloxan buy otc, studies with brief follow-up durations underestimate the potential prognosis of the treated sample. Infrequently after nonsurgical therapy, very in depth lesions can heal with out total resolution of the radiolucency, when fibrous tissue occupies the periapical house (apical scar) (Penick 1961; Bhaskar 1966; Bystr� m et al. Histologic examination of the dissected bundle confirmed it to be fibrous (scar) tissue. Reversal of the therapeutic process is unusual (�rstavik 1996; Kvist and Reit 1999), suggesting that prolonged follow-up of tooth that demonstrate signs of healing after 1 yr could also be pointless (�rstavik 1996). Nevertheless, root-filled enamel remain constantly vulnerable to recurrent infection in the lengthy term. For instance, over 1% of enamel observed to be healed 10�17 years after remedy reverted to illness a decade later (Molven et al. To address this long-term danger, periodic follow-up of root-filled enamel is advocated. Although comparable outcomes for adequate and defective/missing restorations are reported elsewhere (Ricucci et al. It is possible that healing within the immune-compromised sufferers requires an extended time than the 2-year observation in these studies. Better prognosis in tooth with small lesions (5 mm in diameter) than larger lesions has been reported in two current finest proof studies (Weiger et al. Note that based mostly on a cohort research, the proof supporting this predictor is weak. Poorer prognosis (about 67% healed) has been reported in three studies (Sj� gren et al. Although comparable outcomes for enough and extruded root fillings have been reported in two different research (Weiger et al. Prognosis of Healing in Treated Teeth with Endodontic Infections 359 Flareup (intraoperative). Two research have advised no association between the vertically and laterally compacted root fillings and prognosis (Peters et al. Their discovering notwithstanding, the authors emphasize the requirement to validate this variable in a randomized controlled trial (de Chevigny et al. Bacteriologic root canal samples displaying no growth before root filling have been related to better prognosis in a single study (Sj� gren et al. Nevertheless, the restricted aptio tude of root canal bacterial sampling techniques and tradition (Paquette et al. Perforation, file breakage, and massive extrusion of filling supplies have all been instructed to impair healing (Sj� gren et al. However, when they occur, endodontists presently may successfully manage complications related to perforation (Main et al. Thus, the adverse affect of mid-treatment issues on the prognosis could also be mitigated by current administration methods. Falling below the vary reported within the different research, the reported 62% (Sj� gren et al. The variability of the results may be attributed to the same elements as these suggested above for initial therapy. In addition to the healed tooth, progressive healing has been reported in 6% of the teeth (de Chevigny et al. Thus, the potential of enamel with persistent apical periodontitis to heal within 2�4 years after orthograde retreatment is 74�84%, whereas additional 5�6% should be therapeutic presently interval. The late therapeutic was primarily attribute of tooth with surplus root-filling materials (Fristad et al. Also, particularly for retreatment, characteristics of the earlier root canal therapy history have to be considered, together with the previous root filling, a perforation which may be present in a minority of retreated enamel, and the time elapsed since preliminary remedy. Previous root filling quality was not associated with the prognosis in another study (Ng et al. Collectively, these current techniques, often referred to as "apical microsurgery" (Setzer et al. In this regard, these systematic critiques have usually overestimated the prognosis of apical surgical procedure and their conclusions are the topic of controversy (Friedman 2011). The 1-year observation in lots of research reporting on the outcome of apical microsurgery (Table 15. As results of such longterm regression, the healed rates in given populations declined from 84% to 76% at 5 years (von Arx et al. By relying primarily on short-term studies, the recent systematic reviews (Tsesis et al. The majority of studies on the prognosis of apical microsurgery seem to classify outcomes based on wellestablished standards (Rud et al. According to the traditional criteria, each "full" and "incomplete" healing characterize a positive outcome or success, whereas "uncertain" and "unsatisfactory" therapeutic represent unfavorable consequence or failure. Instead, it has been erroneously assigned to teeth displaying reduced radiolucency (Gagliani et al. In particular studies, outcomes can be properly interpreted when both full and incomplete therapeutic categories are specified (Chong et al. The prognosis has been further inflated by a selected analysis 364 Endodontic Microbiology group, incessantly reporting on the prognosis of apical microsurgery, who embody teeth with "unsure therapeutic" within the favorable outcome or success tally (Taschieri et al. In several research incessantly cited for the prognosis of apical microsurgery, the whole cohort (Zuolo et al. In these enamel, apical periodontitis could have been sustained by bacteria colonizing apical root canal ramifications or extraradicular an infection (see part 15. Similarly to the research on nonsurgical therapy, some differences in case selection and composition of study materials exist among the three selected current studies on apical surgery (Barone et al. Unlike the very low incidence of therapeutic regression after nonsurgical remedy, recurrent infection in the lengthy term after apical microsurgery has been reported in 6�10% of healed tooth (Rubinstein and Kim 2002; Wesson and Gale 2003; Song et al. One research according to the current finest evidence reported better prognosis in enamel the place the measured distance between the interproximal bone stage and the cementoenamel junction was 3 mm (78% healed) in comparison with >3 mm (53% healed) (von Arx et al. This finding supported earlier observations in a somewhat giant number of nonselected studies (Rud et al. Taken together, each higher and lower level proof suggests that the prognosis may be compromised by considerable attachment lack of the treated tooth. Studies primarily based on an in vivo mannequin developed to simulate medical situations (Friedman et al. The reported outcomes may have diversified somewhat due to differences in proportions of beforehand retreated tooth and in remedy procedures. Beyond the evaluation of healing, some 85�95% of the tooth might remain symptom-free and practical (Barone et al. Note that based on cohort research, the evidence supporting this predictor is weak. Note that this finding was not correlated with preoperative radiolucency dimension in the identical examine and this variable has not been addressed in the other current finest proof research. Note that incomplete therapeutic by scar tissue happens more regularly in maxillary lateral incisors than in other tooth (Molven et al. Note that healing by scar tissue incessantly happens in very giant lesions (>10 mm in diameter) (Molven et al. Note that modified case choice standards and strategies have been suggested to improve the finish result of second-time surgery (Wang et al. Note that efficient hemostasis is critical for high quality root-end filling (Carr 1998) and bonding of Retroplast apical caps (Jensen et al. Note that with the use of typical ultrasonic ideas, root-end cavities can vary in depth from 1 to three mm Prognosis of Healing in Treated Teeth with Endodontic Infections 367 (a) healing, have to be thought-about as a threat when mandibular molars are handled. Paresthesia was reported in 20% of patients after apical surgery in mandibular molars; it was transient in 19% of patients however lingered for 2 years in 1% of sufferers (Wesson and Gale 2003). A root-end filling is placed to set up an effective barrier in opposition to interaction of intracanal micro organism with the periapical tissues (Friedman 1991). Many nonselected research have reported better outcomes with root-end fillings than without (Friedman et al. Collectively, these low-evidence research suggest that placement of a root-end filling to curtail persistent root canal an infection improves the prognosis.
Viruses in Endodontic Pathosis 181 Current hypotheses on the pathogenesis of periapical pathosis embrace each bacterial and host elements antibiotic eye ointment for dogs ciloxan 250 mg purchase without prescription, however the pathogenic occasions that set off the conversion of a steady antibiotics zantac ciloxan 500 mg online buy cheap, asymptomatic endodontic lesion to a progressive or a symptomatic lesion stay obscure bacteria that cause disease ciloxan 250 mg safe. The pathogenic events that trigger the conversion of a stable, asymptomatic endodontic lesion to a progressive or a symptomatic lesion stay obscure. However, hypothetically a mixed viral�bacterial an infection could explain the major options related to the disease (Slots 2005). Viral affiliation with bacteria and apical illness is in preserving with pathologic position of both infectious brokers. Acute exacerbation of periapical disease may be caused from a mixture of herpesviral and bacterial causes. This chance is according to the majority of research that have observed presence of lively herpesvirus infections in symptomatic periapical lesions and the proinflammatory potential of herpesviruses (Mogensen and Paludan 2001). Human herpesviruses are categorized into three groups (,) based mostly upon details of tissue tropism, pathogenicity, and behavior in the laboratory (Table 8. In most people, main infection by herpesviruses happens early in life and exhibits few or no overt illness symptoms. Herpesviruses remain in contaminated hosts for a lifetime in a prolonged state of latency but retain their capability for renewed or episodic Table 8. Reactivation of latent herpesviruses is involved in driving the pathologic means of some forms of symptomatic periapical disease. Physical trauma, stress, immunosuppression, immune dysfunction, and radiotherapy can trigger herpesvirus activation. Herpesviral replication takes place within the nucleus of the host cell and includes the expression of immediate-early, early, and late classes of genes. Late (structural) genes are expressed through the productive (lytic) section of herpesviral infections. After primary publicity, herpesviruses set up latency in numerous host cell reservoirs, from which they may reactivate periodically (Sissons et al. Herpesvirus transmission occurs by intimate contact with contaminated secretions together with saliva, blood, and genital secretion (Gautheret-Dejean et al. Acquisition of herpesviruses takes place from an early age and sometimes in the uterus. Clinical manifestations of herpesvirus infections are extremely various and vary from gentle or subclinical illness in most wholesome individuals to encephalitis, pneumonia, and different potentially lethal infections, and numerous forms of cancer including lymphoma, sarcoma, and carcinoma in immunocompromised hosts. Infected patients expertise an initial main an infection followed with a period of latency. Patients with latent herpes simplex an infection develop episodes of recurrent oral herpes labialis characterized by the incidence of a cluster of vesicles and shallow ulcers localized to the lateral elements of the lips. Symptoms of this disease included fever, lymphadenopathy, malaise, and sore throat. Oral lesions embrace vesicles on the lips, and the exhausting and soft palates (Millar and Troulis 1994; Miller 1996). It entails the trigeminal nerve and forms ulcerated lesions with outstanding pink borders, resembling aphthous ulcers. Lesions are unilaterally distributed along the contaminated nerve (Millar and Troulis 1994; Miller 1996). It has also been reported to infect a wide variety of cell types (Ablashi 184 Endodontic Microbiology et al. Viruses in Endodontic Pathosis 187 Herpes simplex virus an infection demonstrated no relationship to periapical disease. Acute exacerbation of periapical illness may be brought on by distinctive constellations of pathogenic bacteria or, alternatively, might end result from a combination of herpesviral and bacterial causes. The latter chance is consistent with the observed uniform presence of lively herpesvirus infections in most symptomatic periapical lesions and the proinflammatory potential of herpesviruses (Mogensen and Paludan 2001). Herpesviruses possess a quantity of virulence factors of potential significance for periapical pathosis, including the flexibility to induce immune impairment (Michelson 1999; Boeckh and Nichols 2003), and subsequent overgrowth of pathogenic microorganisms (Kimberlin 1998). Herpesviruses appear also to cooperate with pathogenic micro organism in producing a variety of medical ailments, including inflammatory bowel illness, enterocolitis, esophagitis, pulmonary infections, sinusitis, acute otitis media, dermal abscesses, and pelvic inflammatory illness (Brogden and Guthmiller 2003). Additionally, herpesviruses could give rise to periapical pathosis by inducing cytokine and chemokine release from inflammatory and noninflammatory host cells (Mogensen and Paludan 2001). Periapical sites having inadequate antiviral immune response could additionally be notably prone to tissue breakdown (Sabeti et al. The presence of cytomegalovirus in symptomatic periapical pathosis is according to the notion that inflammatory cells are the source of the virus. Indeed, latent cytomegalovirus resides in numerous myeloid progenitor cell types and in more differentiated hematopoietic cell lineages, and cytomegalovirus translocation within the physique occurs in monocyte� macrophages and dendritic cells (Mocarski et al. Also, cytomegalovirus in marginal periodontitis lesions exists in macrophages and T lymphocytes (Contreras et al. The Fas/Fas ligand system, which is a crucial mobile pathway mediating apoptosis (Chaudhuri et al. In reality, our findings are in agreement with different present studies that reveal there are various but not particular bacterial types, which indiscriminately were actively present in normal, asymptomatic, in addition to symptomatic periapical lesions. On this basis, bacterial infection could serve as cofactor in lymphoid transvascular migration, and cytokine expression be concerned within the pathogenesis of periapical lesions. The inhibition of apoptosis might additional end in continuous irritation and cytokine manufacturing and the establishment of a chronic inflammatory stage. The impact of which may be a failure of the host to management or remove the viral infection, and subsequently the bacterial infection. In conclusion, the current move cytometric evaluation and former histopathologic and polymerase chain reaction-based findings have recognized cytomegalovirus as a frequent inhabitant of symptomatic periapical lesions. As an lively cytomegalovirus an infection induces a multiplicity of interconnected immune reactions, incorporating cytomegalovirus and different herpesviruses into studies on infectious causes and causal mechanisms of periapical pathosis might provide essential new insights into the pathogenesis of the illness. Herpesvirusmediated pathogenicity takes place by way of several mechanisms, working alone or together, and involving both cellular and humoral host responses (2000 (Table 8. Herpesviruses may cause direct cytopathic effects on periapical fibroblasts, endothelial cells, and bone cells, the results of that are impaired tissue turnover and restore, and in the end lack of tissue. Impairment of host defense cells can predispose to overgrowth of endodontic pathogenic bacteria. Herpesvirus activation can induce significant immunosuppressive and immunomodulatory results in periapical websites. Herpesviruses can set off an array of host responses that embody dysregulation of macrophages and lymphocytes and downregulate the antiviral host immune response (Boeckh and Nichols 2003). Herpesvirus infections elicit proinflammatory cytokine and chemokine release from inflammatory cells. These inflammatory mediators, that are more than likely produced regionally by periapical macrophages (Miyauchi et al. Previous research a have focused on lipopolysaccharide as an inducer of macrophage cytokine production (Page et al. Cytokines and chemokines have important roles in the first line of protection against human herpesvirus infections and contribute considerably to regulation of acquired immune responses. However, by a various array of strategies, herpesviruses are in a place to interfere with cytokine manufacturing or divert potent antiviral cytokine responses, which allow the viruses to survive all through the lifetime of the host (Alcami and Koszinowski 2000; Tortorella et al. Proinflammatory actions usually serve a constructive biologic objective by aiming to overcome an infection or invasion by infectious agents, however can also exert detrimental effects when a problem becomes overwhelming or with a chronic pathophysiologic stimulus. Also, viruses show nice uniqueness in phrases of diverting the potent antiviral cytokine responses to their benefit (Tortorella et al. Herpesviruses can produce periapical tissue damage as results of immunopathologic responses. Th1 cells, which predominate in periapical lesions (Brogden and Guthmiller 2003), are mediators of delayed type hypersensitivity (Seymour et al. Control of herpesviral replication and prevention of pathosis rely upon both innate and adaptive immune mechanisms. Antiviral antibodies might help management infectious virions and cytotoxic T lymphocytes have an important position in limiting the proliferation of herpesvirus-infected cells. Herpesvirus infection of periapical sites could also be essential in a multistage pathogenesis by altering native host defenses.
These projection neurons ascend through the contralateral trigeminothalamic tract and synapse with greater order neurons in the thalamus with last neuronal projections into the sensory cerebral cortex (Penfield and Ramussen 1950) virus yole ciloxan 750 mg discount with amex. Although the dental construction is among the most closely innervated tissues in the physique with pain-sensing neurons (nociceptors) bacteria viruses cheap ciloxan 250 mg online, not all neurons within the dental pulp and periodontal ligament are nociceptors bacteria with flagella list 500 mg ciloxan. There are postganglionic sympathetic fibers from the cervical sympathetic ganglia and different afferent low threshold (A-) trigeminal fibers liable for detecting nonnoxious tactile info (Hargreaves and Goodis 2002). There are vital differences between Cfiber and A- nociceptors concerning anatomy (neuronal morphology and distribution) and conduction velocity. Electrophysiologic research measuring the conduction velocity of sensory neurons kind the basis of widely used nomenclature of these fibers. The C-fibers have a slower conduction velocity (<2 m/s) than A- fibers (2 m/s conduction velocity). Anatomically, C-fibers are unmyelinated and originate from small neurons and, in contrast, A- fibers are lightly myelinated and originate from small to medium diameter Endodontic Infections and Pain 253 cell bodies in one of the three divisions of the trigeminal ganglion. Myelination provides axonal insulation permitting action potentials to propagate quicker in A- fibers. Although trigeminal neurons project their central terminals to different brainstem nuclei (the nuclei interpolaris, oralis, and caudalis), much of the nociceptive input is assumed to be situated within the outer layers of the nucleus caudalis (Dubner and Bennett 1983; Hargreaves and Milam 2001; Sessle 2005). Central sensitization was verified by the rise within the mechanoreceptive area within the mice orofacial region and a decrease in mechanical activation threshold (mechanical allodynia) (Park et al. The detection of serious long-lasting central sensitization following noxious stimulation of the dental pulp suggests that this sturdy activation of major afferent neurons within the dental pulp is capable of causing central modifications leading to allodynia in areas other that the tooth itself. Importantly, on this research, microinjections of a synaptic inhibitor into the nucleus caudalis completely abolished central sensitization, whereas injections into the other nuclei (oralis and interpolaris) had no impact. Thus, the dental pulp is richly innervated by nociceptors that project and connect with second order neurons in the nucleus caudalis the place neuronal plasticity and central sensitization might take place (discussed below). In the dental pulp, the greatest density of innervation is discovered within the coronal side at the stage of the pulpal horns (Byers 1984). At these areas, nociceptors are introduced as intertwined ramified free nerve endings forming a plexus construction (Luthman et al. A- fibers are recognized to traverse the odontoblastic layer, lose their myelination, and project roughly zero. The innervation of the dentinal tubules by A- nociceptive fibers agrees qualitatively with the sharp and transient ache normally originated when the dentin is stimulated. According to the hydrodynamic concept, this pain is the results of fluid transferring in the dentinal tubules because of thermal (cold drinks or 1,1,1,2 tetraflouroethane [Endo Ice] application during pulp vitality examination), drilling (during cavity preparation), or hypertonic (sweets) stimuli (Brannstrom and Johnson 1978). This theory has been substantiated by several studies exhibiting that the motion of fluid within the tubules generates discharges in nociceptors and that closing of the dentinal tubules confers resistance to these noxious dentinal stimuli (Ahlquist et al. Besides the motion of fluid via the dentinal tubules and subsequent activation of mechanosensitive fibers, transdentinal cooling or heating could doubtlessly activate C-fibers positioned deeper in the dental pulp. In order for this to occur in uninjured tissue, the temperature gradient needs to diffuse from the mineralized tissues and attain C-fibers at a noxious ranges adequate for activating these high threshold fibers. Indeed, in an experimental setting, heating of the tooth generated a pointy pain that subsided (consistent with A- fiber activation) adopted by a ache characterized by a sluggish, burning pain (consistent with C-fiber activation) (Jyvasjarvi and Kniffki 1987). Although Cfiber nociceptors doubtless encode this deep pulpal thermal nociception, maybe their most essential position is detection of inflammatory ache. There is growing recognition that odontoblasts are doubtless concerned in nociception (Allard et al. These extremely specialised cells have features that stretch far past their best function as dentin secreting cells. They have been discovered to specific a posh array of receptors and inflammatory mediators primarily present in cells of the innate immune response. Importantly, odontoblasts additionally categorical ionotropic channels primarily present in nociceptors such as transient receptor potential channels (discussed later) and voltage gated sodium channels. In addition, these odontoblast are selectively activated by agonist recognized to activate nociceptors. Therefore, despite increased gained knowledge in odontoblast physiology, their direct function in nociception remains elusive. Several members of this ionotropic family have been immediately implicated in nociception when expressed in sensory neurons (Julius 2013). This thermosensitive channel is activated by noxious warmth (temperature >43 C) via the just lately discovered launch of endogenous oxidized metabolites of linoleic acid. These inflammatory mediators are usually released in a cascade that contains an "inflammatory soup"(Julius and Basbaum 2001; Cunha et al. Whenever the focus of any given mediator is sufficient to bind and activate its receptors in the nociceptors, intracellular signaling pathways are triggered. Many intracellular signaling pathways are recognized to sensitize or activate nociceptors. For instance, local elevation of prostaglandin E2 prompts protein kinase A resulting in nociceptor sensitization, whereas elevated tissue quantities of bradykinin prompts phospholipase C and protein kinase C, leading to nociceptor activation. Thus, allodynia can be produced by inflammatory mediators that sensitize nociceptors. Interestingly, the dull, throbbing pain sensation sometimes associated with activation of C nociceptors is often reported by patients with irreversible pulpitis. The process generally known as central sensitization happens when the first afferent signal is amplified at this central terminal. Central sensitization represents a major element in inflammatory hyperalgesia and allodynia (Woolf 1996). Interventions at this receptor within the central terminals induce either reduction or enhancement of central sensitization generated by repeated C-fiber discharge. Clinically, central sensitization may be observed in patients complaining of persistent pain even after the elimination of inflamed peripheral tissue with endodontic and restorative procedures or in allodynia felt in enamel and tissue surrounding an offending tooth. Studies have proven that the presence of preoperative ache increases the chance of postoperative pain (Torabinejad et al. Furthermore, preemptive analgesia during surgical procedures is associated with reduced postoperative ache in many conditions (Woolf and Chong 1993; Reuben 2007). This means that patients who seek endodontic help at the first signal of symptoms, and who receive remedy beneath enough profound anesthesia, have higher postoperative prognosis because of the decreased probability of creating central sensitization. Despite these significant technical advances, ache might persist following enough therapy, with a reported frequency of 5. Although an endodontic therapy could also be deemed sufficient when evaluating periapical radiographs, ache might persist for longer than 6 months. The evaluation of periapical radiographs has been historically used as an consequence measure of endodontic success. Despite efforts to set up standardized standards such because the periapical index (�rstavik et al. Therefore, persistent postendodontic pain of odontogenic origin may be associated with symptomatic apical periodontitis not detected with standard radiographic imaging methods. From this attitude, persistent ache might end result from the failure to utterly eliminate the original etiologic elements. While nonodontogenic pain circumstances have to be thought-about within the differential diagnosis of persistent postendodontic ache, these findings point out that certain circumstances of posttreatment pain may outcome from persistent symptomatic apical periodontitis. There are many components that predispose patients to persistent post-treatment apical periodontitis. These embrace host factors such as systemic diseases that modulate the immune system. In addition, each cytokines are additionally known to sensitize nociceptors, being essential gamers in inflammatory thermal hyperalgesia and mechanical allodynia (Ferreira et al. The frequency of nonodontogenic ache lasting longer than 6 months following root canal remedy has been discovered to be about 3% of cases (Nixdorf et al. This means that, a minimal of partially, some enamel could have been misdiagnosed as being the supply of the ache and have been erroneously endodontically handled. Another examine found that approximately half of the instances with diagnosis of nonodontogenic pain following root canal therapy have been associated to referred pain from temporomandibular problems (Nixdorf et al. Importantly, the bulk (63%) of the patients reporting persistent ache following root canal therapy also reported a history of continual pain elsewhere within the body.
The reason for that is the rise in the floor vitality of the foundation dentinal wall freed from the smear layer [15] antibiotics for dogs ear infection 750 mg ciloxan safe. GuttaFlow 2 Fast (Colt�ne/Whaledent antibiotic for bacterial vaginosis trusted ciloxan 750 mg, Altst�tten antibiotics for dogs harmful 500 mg ciloxan cheap otc, Switzerland), is a complicated next-generation product of GuttaFlow using gutta-percha powder with particle size of lower than 30 nm. GuttaFlow Bioseal has been launched with the natural repair mechanism of regeneration by forming hydroxyapatite crystals. The introduction of a premixed sealer eliminates the potential for heterogeneous consistency during mixing. When the sealer is positioned within the root canal, the fabric absorbs water from the dentin tubules, causing a hydration response of the dicalcium silicate and tricalcium silicate. Calcium phosphate reacts with calcium hydroxide on the identical time to precipitate hydroxyapatite and water. This water continues to be used for the hydration of the calcium silicates and leads to the formation of a composite community of gel-like calcium silicate hydrate, which mixes with the hydroxyapatite bioceramics and types a hermetic seal inside the basis canal. This hydroxyapatite has the power to broaden and harden contained in the canal, which helps to create an ideal seal with the walls. It produces calcium hydroxide, which is released in resolution and produces an interstitial layer that resembles hydroxyapatite constructions in simulated body fluids. Being an entirely inorganic material, Portland cement undergoes chemical shrinkage following hydration. Its function as a sealer where it adheres nicely to dentin and obturating materials, its cohesive power, wetting properties, low viscosity, cytotoxicity, and biocompatibility were later in comparability with other sealers. Most experiments are laboratory based mostly or in animal fashions, which can differ from a scientific state of affairs. This has been vastly recommended for pulp capping, pulpotomy, forming an apical barrier, repairing root perforation, and root canal Pro-Root Endo Sealer (Dentsply Tulsa) ProRoot Endo Sealer is a calcium silicate�based endodontic sealer used in both lateral heat vertical or carrier-based obturation methods. The main components are tricalcium silicate and dicalcium silicate, with inclusion of calcium sulfate as setting retardant, bismuth oxide as a radiopacifier, and a small amount of tricalcium aluminate. Tricalcium aluminate is important for the preliminary hydration response of the cement. The liquid part consists of viscous aqueous answer of a water-soluble polymer to enhance the workability and flow. The powder consists of fine hydrophilic particles that kind a gel within the presence of moisture. The main constituents are tricalcium silicate, tricalcium oxide, and tricalcium aluminate. The most important difference is the presence of huge amounts of calcium carbonate, which is intended to enhance the discharge of the calcium ions and enhance the adhesion to the dentinal walls with adequate circulate and biocompatibility. It delivers easily and exhibits excellent handling characteristics and an improved setting time. Salicylate resin is tissue friendly and therefore a better choice over epoxy-based resins. The two pastes combine in a homogeneous mix to form a rigid however semipermeable construction. It displays an alkaline pH, has a good circulate price, has a perfect working time of 35 minutes, is antimicrobial, and has a low movie thickness to simply penetrate into the accent canals. The greater solubility may end up in 116 Current therapy in endodontics larger cytotoxicity as the fabric continues to leak and irritate the neighboring tissue [30�33]. This sealer demonstrated secure leakage values at 15 and 30 days and good sealing capacity. However, at 60 days, the fabric exhibited a considerable improve in leakage and low move rate. This helped in increasing the sealing ability of the sealer due to greater expansion achieved. Fluoride ions can penetrate into the dentin and improve the mineralization of the dentin. The setting response entails the continuous formation of hydration merchandise that contribute in decreasing the microchannels within the sealer. The pH is increased up to 12 and will play a protective position in stopping bacterial recontamination of a filled root canal. There are two conditions for the monoblock to operate as a mechanically homogeneous unit. First, the materials that represent the monoblock ought to have the ability to bond strongly and mutually to one another, as well as to the substrate that the monoblock is meant to reinforce. Monoblocks in the root canal spaces may be categorized as primary, secondary, or tertiary depending on the number of interfaces current between the bonding substrate and the majority material core. A traditional instance of major monoblock can be obturating the foundation canals with gutta-percha without utilizing the sealer. The lack of sufficient energy and stiffness is the main drawback, and this led to the development of secondary monoblocks. The combined use of a sealer and a core materials introduces further interfaces right into a monoblock during obturations. Secondary monoblocks have two circumferential interfaces, one between the cement and dentin and another between cement and the core materials. A traditional instance is the use of sealer for obturation, whereby one interface is between the gutta-percha point and sealer and the second one is between the sealer and the foundation canal wall. Their bondability to the radicular dentin and root canal materials is also superior in comparability with different cements. However, the monoblock idea is explained first for higher understanding of their setting response. Monoblock concept the time period monoblock, which means a single unit, has been employed in dentistry for the reason that flip of the century. The concept was to create a root canal monoblock to obtain a complete bond and a complete seal of the foundation canal house, which prevented by the shortage of chemical union between the gutta-percha and the resin-based or glass ionomer�based sealer. Tertiary monoblock A third circumferential interface is introduced between the bonding substrate and the abutment materials by coating the nonbondable gutta-percha with supplies that make them bondable to the sealers, thus creating tertiary monoblocks. Because the tertiary interface exists as an exterior coating on the surface of the gutta-percha, such methods are designed to be used with both a single-cone technique or placement of accent cones with out lateral compaction, to keep away from disrupting the exterior coatings. Fiber posts that contain an exterior silicate coating or nonpolymerized resin composite for lining root canals which are oval or not perfectly round or broad so that the fiber post may be fitted correctly are thought-about a tertiary monoblock. Challenges with monoblocks Although the idea of making a mechanically homogeneous unit with root dentin is superb in principle, carrying out these perfect monoblocks within the root canal space is challenging, as a outcome of bonding to dentin is compromised by volumetric modifications that happen in resin-based materials during polymerization. There seems to be no adhesive root canal materials that can perfectly obturate the canal area with a tight seal that consists of various interfaces, simultaneously improving the fracture resistance of the tooth. Even when the impact of dentin permeability in endodontically treated enamel is minimal, entrapment of residual moisture inside the root canal can lead to the permeation of this unbound water through hydrophilic adhesive layers [37, 38]. This can work as stress raisers and promote crack progress and propagation throughout loading alongside the interface. The extremely unfavorable and sophisticated geometry of the substrate, particularly root canal house, also proves to be detrimental to the polymerization of the resin cements or sealers. However, continued research and growth is carried out and is likely to result in improvements. First-generation methacrylate resin�based sealers Hydron (Hydron applied sciences,Inc. Though it demonstrated ease of application, antibacterial properties, and flexibility to the canal wall, adverse inflammatory reactions and leakage issues had been additionally observed [39, 40]. The technology of an endodontic seal relies on the penetration of the hydrophilic sealer into the dentinal tubules and lateral canals following elimination of the smear layer. This types a hybrid layer by creating resin tags with the collagen community [41�43]. The sealer has hydrophilic qualities and hence can be used in root canals that pose a challenge of moist setting. In this technique, no dentin adhesive is employed and an accelerator is used together with the resin-coated gutta-percha cones to provide rapid remedy process and likewise to promote higher bonding between the gutta-percha cone and the sealer, which in flip bonds properly to the canal wall to set up a complete monoblock seal [46]. This sort of resin-coated cone is recommended for use with the EndoReZ system (explained later). Third-generation methacrylate resin�based sealers As the resin era improved, a 3rd era of self-etching sealers was introduced, which contained self-etching primer together with dual-cured resin sealer for root canal obturation procedures. This introduces the idea of incorporating the smear layer within the sealer�dentin interface. The sealer can be used with gutta-percha or with resin-coated gutta-percha, the latter with the objective of forming a monoblock. The apical part of the obturator is gutta-percha, and the coronal two-thirds consists of a resin and a glass fiber publish for adhesive bonding.
As the hematoma retracts antibiotic lawsuit order 250 mg ciloxan free shipping, serum leaks out of the capillaries and causes perihematomal edema virus new york discount ciloxan 750 mg visa. Blood launched from the capillaries prompts the coagulation cascade non prescription antibiotics for acne 500 mg ciloxan discount amex, and thrombin is released. The lysis of red blood cells releases hemoglobin and different neurotoxic inflammatory mediators and contributes to secondary brain damage. Dilation of the left frontal horn is the results of obstructive hydrocephalus, a consequence of compression of the third ventricle. Within the hemotoma, the precise focus of contrast extravasation, referred to as the "spot signal" when seen on computed tomography angiography, is predictive of additional hemorrhagic enlargement. In certain circumstances, fast consultation with a neurosurgeon and transfer to an applicable facility supply the best chance for survival. Laboratory studies ought to embrace a complete blood rely, prothrombin and partial thromboplastin time measurements, liver and renal perform checks, serum glucose measurements, and a toxicology screen. Complications such as problem dealing with secretions or swallowing, hyperventilation, and hypoventilation warrant instant intubation. A fast neurological examination must be performed to gauge responsiveness to vocal or painful stimuli. Etomidate is an effective induction agent because it has a rapid onset of motion, has minimal hemodynamic effects, and permits a fast restoration. It is essential to rigorously titrate propofol to avoid its major facet effect, hypotension. Continued sedation with this agent requires attentive monitoring for 628 the signs of propofol infusion syndrome: extreme metabolic acidosis, rhabdomyolysis, hyperkalemia, and renal failure along with hypertriglyceridemia and arrhythmias. Blood pressure control and its administration are critical determinants of end result, however the target range stays controversial. All treatment efforts are geared toward sustaining this delicate stability and homeostasis. The preliminary reduction of blood strain should be no more than 15% within the first hour as a end result of many patients have acclimated to greater ranges and fast reductions might worsen ischemia. Clinicians can scale back the danger of hematoma enlargement and improve outcomes by avoiding overshoots and fluctuations in pressure. It is important to do not forget that no scientific guideline recommends allowing the blood strain to remain extraordinarily elevated without remedy. They offer the benefit of sustaining homeostasis by exerting little osmotic impact on surrounding tissues. These options can also contribute to hyperglycemia, which can be detrimental to stroke sufferers. These newer brokers are well-liked because of their rapid time to peak motion and broad therapeutic window, which obviate the necessity for frequent therapeutic monitoring. In sufferers with life-threatening intracerebral hemorrhage, the drug can be given as a 5-mg bolus or infusion (Table 19-7). Protamine sulfate is given by slow intravenous injection, not to exceed 5 mg/min, with a complete dose to not exceed 50 mg. Importantly, protamine sulfate can cause hypotension, nausea, vomiting, and anaphylaxis. Any reversal should be evaluated with normal coagulation research performed 30 minutes after infusions, with the goal being the normalization of laboratory markers. Patient administration begins with elevation of the pinnacle of the mattress, fluid resuscitation, and sedation and analgesia. Hypertonic saline is more and more being used in varied settings as an different selection to mannitol for the therapy of cerebral edema. Theoretically, hypertonic saline is advantageous over mannitol as a outcome of the blood-brain barrier is less permeable and it 634 might be a simpler osmotic agent. It is administered as boluses of 3% to 23% each 3 to 4 hours or as a continuous infusion. Although this therapy might help minimize reflex vasodilation and increase blood move, the danger of cerebral ischemia and hypoxia remains. Ventriculostomy is often carried out by a neurosurgeon; the choice to insert an intraventricular catheter should be made by an experienced neurosurgical group that can monitor the device and augment treatment as essential. These devices use microtransducers and fiberoptic transducers, which are simpler to insert than normal ventriculostomy catheters. A burr hole also could be made within the cranium, permitting needle aspiration of the hematoma and insertion of a 3- to 4-mm microsilicone catheter. Because the consistency of each clot is unpredictable, it could be tough to aspirate blood through a catheter without direct visualization. The technique provides a detailed set of coordinates 637 focusing on precise sites within the brain that require drainage. The neuroendoscopic method uses direct visualization and ultrasound guidance with a dual-channel drain. Despite the truth that the lesion was operatively approachable, it resided near eloquent (essential) areas of the brain. The neurosurgeon and household selected initial conservative administration adopted by admission and observation; sadly, the affected person died. Large Intraparenchymal Intracerebral Hemorrhage 639 For contained deeper thalamic and putamen intracerebral intraparenchymal hemorrhage, mortality charges are considerably lower (20%�40%). This moderately sized, right-sided intracerebral hemorrhagic stroke (*) occurred in a 40-year-old man who was awake but confused; there was no midline shift, no intraventricular extension, no hydrocephalus, and no scientific weak point. This bleed in the easily accessible frontal area of the brain in an awake affected person was evacuated and treated by commonplace craniotomy with out problem by the neurosurgeon. Cerebellar hemorrhages bigger than 3 cm that cause brainstem compression or hydrocephalus are nearly universally fatal without surgical intervention. Patients with smaller cerebellar hemorrhages without brainstem compression may be managed medically and do reasonably well. Prognosis will be related to well timed access to an operating room and an skilled neurosurgeon. Hematoma* has prolonged extraaxially (arrow) and into fourth ventricle (arrowhead). With this method, which appears to cut back the danger of perihematoma edema, the clot undergoes lysis after which may be removed shortly and safely. Although no specific goal vary has been established, glucose ranges must be kept under one hundred eighty mg/dL and hypoglycemia must be prevented. Aggressive fever control with acetaminophen and mechanical cooling can reduce the danger of mortality and improve outcomes. The effect of this complication on outcomes is unclear, however those with clinically significant seizures must be handled with anticonvulsants. The objective of fluid resuscitation should be to keep the patient euvolemic and regular to hyperosmolar. The emergency 645 physician should contemplate a number of therapeutic strategies in such situations and consult with neurology, neurosurgery, and interventional radiology groups. Guidelines for the administration of spontaneous intracerebral hemorrhage in adults: 2007 replace: a tenet from the American Heart Association/American Stroke Association Stroke Council, High Blood Pressure Research Council, and the Quality of Care and Outcomes in Research Interdisciplinary Working Group. Treatment of warfarinassociated intracerebral hemorrhage: literature review and expert opinion. Evidence-based management of anticoagulant therapy: antithrombotic remedy and prevention of thrombosis, ninth ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Hematoma progress and outcome in handled neurocritical care sufferers with intracerebral hemorrhage associated to oral anticoagulant therapy: comparability of acute remedy methods utilizing vitamin K, fresh 647 frozen plasma, and prothrombin complex concentrates. A device for predicting end result after spontaneous supratentorial intracerebral hemorrhage [abstract]. Minimally invasive surgery plus recombinant tissue-type plasminogen activator for intracerebral hemorrhage evacuation decreases perihematomal edema. Approximately 12% to 15% of patients die before reaching the hospital and 50% of survivors suffer from persistent neurological deficits; nevertheless, probably lifesaving interventions throughout early resuscitation are available. Therefore, those with or at risk for hydrocephalus ought to be assessed for airway safety, particularly if transport to another facility is deliberate. Pretreatment with fentanyl can attenuate the effect on the reflex sympathetic response. Breathing Hypoxia, outlined as an arterial partial pressure of oxygen (PaO2) lower than 60 mm Hg or an oxygen saturation less than 90%, is related to elevated morbidity and mortality in sufferers with mind accidents. Cerebral hypoxia can occur regardless of "regular" systemic oxygenation and perfusion in response to microvascular and mobile metabolic dysfunction; nonetheless, excessive oxygen can potentiate secondary mind damage and is related to worse outcomes.
The declining incidence of the illness is believed to be secondary to the sooner identification of renal disease and improved hemodialysis; nevertheless virus protection software 750 mg ciloxan order with visa, the precise etiology of uremic pericarditis stays unclear infection minecraft server generic ciloxan 750 mg without prescription. Despite regular compliance with medical therapy and dialysis antimicrobial kinetic sand purchase 1000 mg ciloxan, numerous these sufferers nonetheless go on to develop uremic pericarditis with out the classic signs and signs (eg, chest ache, fever, and electrocardiographic changes). Signs and Symptoms Other than traumatic pericardial effusions, the presentation of tamponade could be refined; symptoms are neither particular nor sensitive and are easily mistaken for other clinical entities. If overt indicators and symptoms are readily observed, the clinician ought to anticipate deterioration and circulatory collapse. The detection of the Beck triad (muffled heart sounds, jugular venous distension, and hypotension) is taken into account pathognomonic for cardiac tamponade. However, this description relies on traumatic pericardial hemorrhage and is often not evident in other types of the disease. Tachypnea, jugular venous distension, and pulsus paradoxus are also notable findings in many patients. This complication, known as pulsus paradoxus, could be detected utilizing a stethoscope and manual sphygmomanometer. Clinical examination findings that ought to raise concern for imminent deterioration embody a decline in psychological standing or agitation, worsening tachypnea (reflecting acidosis), decline in tachycardia (circulatory fatigue), decreased urine output, and pallor with poor extremity perfusion. This signal is a late discovering and infrequently not seen till arrest is imminent due to pure compensatory mechanisms such as sympathetic tone and catecholamine response. Clear lungs sounds and an absence of cephalization might help differentiate tamponade from decompensated congestive coronary heart failure. Water-Bottle Heart Sign 357 the American Society of Echocardiography/American Heart Association/American College of Cardiology recommends that any suspected pericardial situation, especially tamponade (class I), ought to be evaluated initially by echocardiography. Vital to the care of each critically unwell affected person with suspected pericardial tamponade, the imaging modality offers essential physiological data that may alter medical therapy and outcomes. The prognosis for patients with penetrating accidents is best than for people who have sustained blunt (decelerating) trauma, which frequently causes 359 aortic dissection. The single most necessary issue for survival is the presence of vital signs upon arrival on the therapy facility. In these eventualities, time is of the essence - immediate intervention is required if any indicators of life are present. Stabilization may be tried with pericardiocentesis, allowing the controlled drainage of very small amounts of the hemopericardium, and switch to a quaternary care institution the place subspecialists are readily available. Another option is thoracotomy, adopted by opening of the pericardial layers to permit evacuation of the tamponade and restore of any lacerations or crossclamping of the aorta for definitive restore. These instances require resuscitation and continuous cardiac monitoring to thwart impending circulatory failure. These are merely temporary measures until extra definitive therapy could be initiated. Management ought to start with mild quantity challenges using crystalloids since many patients are intravascularly hypovolemic. Conversely, the administration of extreme quantities of fluid can show deleterious and worsen the intracardiac pressures, at which level fluids must be discontinued promptly. Patients with extra briskly deteriorating hemodynamics despite fluid administration require further pharmacological adjuncts till pericardiocentesis could be performed. Several studies have listed isoprenaline, dopamine, and dobutamine as suitable and appropriate first-line agents for increasing cardiac output in instances of tamponade. Some researchers theorize 360 that vasopressors (eg, norepinephrine) improve blood pressure more than inotrope, but also notice their lack of optimistic effect on cardiac index. Any agents that blunt the endogenous sympathetic and catecholamine surge (eg, beta- and alpha-blockers, anesthetics, or aggressive analgesics) can result in detrimental hemodynamic effects. The initiation of positive-pressure ventilation will additional enhance intrathoracic stress and worsen venous return, often leading to catastrophic circulatory collapse. Hemodynamically Unstable Tamponade Hemodynamically unstable sufferers require instant pericardiocentesis or operative repair because of their potentially speedy development to death. Large-volume pericardiocentesis causes abrupt fluid shifts resulting in pulmonary edema and fast respiratory decompensation. Pericardial fluid may be removed using any of a number of strategies, together with blind percutaneous drainage, ultrasound-guided percutaneous drainage, percutaneous balloon pericardiotomy, and the surgical creation of a pericardial window. For steady sufferers whose tamponade is insidious, recurrent, or traumatic, a semielective procedure carried out at the side of a cardiologist or cardiothoracic 361 surgeon is recommended. The materials wanted to perform pericardiocentesis can be found in a kit, similar to a central venous catheter equipment, which can be used in its stead. Major issues of the process include cardiac chamber perforation, coronary laceration, pneumothorax, intraabdominal laceration, and hole viscous harm. A pericardiocentesis package should be used if out there; a central venous catheter equipment additionally could be utilized. If neither is on the market, any 16- or 18gauge spinal needle attached to a 20-mL Luer lock syringe is enough. Insert the needle on the left xiphocostal angle, aiming it towards the left shoulder at a 30- to 45-degree angle. Once a small quantity of fluid may be aspirated easily, the hemodynamics should improve dramatically. Then, utilizing a Seldinger technique, insert an indwelling pigtail catheter, which can allow further fluid removal ought to hemodynamics weaken. Pericardiocentesis Blind Subxiphoid Approach 363 Ultrasound-Guided Approach If ultrasound is available, it may be utilized in certainly one of two methods to carry out pericardiocentesis. With this method, imaging is used to establish the biggest pocket of fluid and its approximate depth (but not through the aspiration of the effusion). As with static steering, the biggest fluid pocket is identified and the aspiration is visualized in realtime all through the complete process. Unlike in the blind method - for which solely subxiphoid entry is beneficial - with ultrasound guidance, apical or parasternal approaches also can be taken. Dynamic ultrasound is associated with a decrease incidence of sequelae than pericardiocentesis without visualization. As with any thoracic procedure, the inferior rib margin ought to be avoided to forestall neurovascular damage. Aspirate the place the fluid collection appears to be the most important and closest to the skin/ultrasound transducer. Based on the mixing of scientific signs, indicators, and echocardiographic findings, the system can be used to establish sufferers who want instant pericardiocentesis. Triage technique for pressing management of cardiac tamponade: a place statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Rapidly growing accumulations (as seen in traumatic tamponade) usually cause profound hypotension and precipitous dying; nevertheless, the slow accrual of quantity (as seen in non-traumatic forms) allow pericardial distension, transforming, and gradual transformations with out drastic 366 2. Pulsus paradoxus could be seen in patients with several conditions: obstructive pulmonary illness, bronchial asthma, pulmonary embolism, and right ventricular infarction with shock. It can be absent in certain populations with tamponade: pulmonary hypertension, aortic regurgitation, right coronary heart or regional tamponade, and low-pressure tamponade. In this scenario, sufferers will have obscure signs much like those of lowpressure tamponade; a excessive degree of suspicion is needed. Pericardiocentesis should be the primary process carried out in any affected person with waning hemodynamics. Tamponade patients ought to endure pericardiocentesis prior to mechanical air flow. Conclusion Cardiac tamponade is a fragile clinical entity that turns into a ticking time bomb if not identified and handled. With the appearance of bedside ultrasound, even novice users can quickly and easily determine an effusion. After tamponade physiology has been identified, close cardiac monitoring is warranted, quantity resuscitation should be approached carefully, and adjunctive pharmacological brokers must be administered if needed. Ultimately, 367 lives are saved when a skilled clinician can quickly establish tamponade, carry out immediate pericardiocentesis in unstable sufferers, and facilitate stabilization and disposition for definitive therapy. Sensitivity and specificity of echocardiographic proof of tamponade: implications for ventricular interdependence and pulsus paradoxus. Echocardiographyguided pericardiocentesis with probe-mounted needle: report of fifty three instances.
Furthermore virus 68 sintomas ciloxan 250 mg purchase without prescription, the patient usually felt ache because of rubella virus purchase 500 mg ciloxan overnight delivery high currents in the machines [45] treatment for sinus infection natural ciloxan 250 mg generic amex. It also gave inaccurate readings in obstructed canals, in enamel with caries or faulty restorations, and in cases of perforations. Impedance-based (second-generation) apex locators Impedance-based apex locators, also recognized as singlefrequency impedance apex locators, measure opposition to the move of alternating present or impedance as an alternative of resistance. Impedance-based locators have been introduced to overcome the problems of the primary era. This property was used to measure distance in different canal situations by utilizing totally different frequencies. The change in frequency methodology of measuring was developed by Inoue in 1971 and launched within the Sono-Explorer (Hayashi Dental Supply, Tokyo, Japan), which calibrated on the periodontal pocket of every tooth. This measures two impedances and identifies the canal terminus when the readings method each other. The frequency of this impedance is directed to a speaker that produces an auditory tone generated by the use of low-frequency oscillation. The most important disadvantage of this device was the need for particular person calibration. This consisted of an insulated file that was launched within the gingival crevice, and the sound produced was named the "gingival crevice sound. To decrease the variable capacitance feature of the circuit, a high-frequency (400 kHz) wave-measuring system, the Endocater (Yamaura Seisokushu, Tokyo, Japan), was launched by Hasegawa and colleagues (1986). The sheath, nevertheless, brought on issues as a end result of it would not enter narrow canals, could presumably be rubbed off, and was affected by autoclaving. Furthermore, the device gave inaccurate readings when used in canals containing electrolytes [38, 47]. A variety of second-generation apex locators were designed and marketed, however all suffered similar problems of incorrect readings with electrolytes in the canals and in addition in dry canals. These devices regulate their sensitivity to compensate for the intracanal setting and indicate on the display when the gadget should be switched from a "wet" to a "dry" mode or vice versa. This system at all times duplicated the canal length as determined by visualizing the tip of a file on the foramen of extracted teeth (Czerw et al. It uses an alternating present and measures impedance to measure the space of the file tip to the apex; it has also had variable results in phrases of accuracy. Some of the opposite apex locators on this technology include Dentometer (Dahlin Electromedicine, Copenhagen, Denmark) and Endo Radar (Elettronica Liarre, Imola, Italy). The main drawback of second-generation digital apex locators is that the foundation canal has to be moderately freed from electroconductive supplies to get hold of correct readings. The presence of tissue and electroconductive irrigants in the canal changes the electrical characteristics and results in inaccurate, normally shorter measurements [49]. Third-generation devices work by monitoring adjustments in impedance of the tooth at completely different frequencies: a high one at 8 kHz and a low one at 400 Hz. In the coronal portion of the canal, the impedance distinction between the frequencies is fixed. As the file is advanced through apical constriction, the difference within the impedance value increases and reaches a maximum worth at the apical space [38, 50]. All apex locators are outfitted with a display display or some indicators and a kind of alarm that visually and audibly point out each the proximity and the location of the apical foramen. Because the magnitude of impedance depends on the measurement of the frequency, the use of two frequencies gives the chance of observing the difference between the 2 results as the needle advances in the root canal. Therefore, this is a comparativeimpedance technique as a outcome of it measures the impedance distinction, which could be converted into size information. Because the impedance of a given circuit may be substantially influenced by the frequency of the present flow, these gadgets are also referred to as frequency-dependent apex locators. These gadgets have more powerful microprocessors and are in a position to course of the mathematical quotient and algorithm calculations required to give accurate readings. They have also demonstrated practical reliability with no statistically important distinction in measurements between teeth with necrotic or vital pulpal diagnoses [51]. Morita, Tokyo, Japan) is an example of a self-calibrating third-generation apex locator primarily based on the ratio methodology. The ratio method works on the principle that two electrical currents with different wave frequencies could have measurable impedances that could be measured and compared as a ratio no matter the kind of electrolyte in the canal. Since its introduction in 1992, it has turn into the benchmark to which different apex locators are compared. The quotient of the impedances is displayed on a liquid crystal show meter panel and represents the place of the instrument tip within the canal. This system has the advantage of not having to be calibrated for every patient and makes it one of the efficient and versatile to use. The unit is self-calibrating and can measure with electrolytes current in the canal. The precept behind this device, nonetheless, is much like the impedance ratio-based devices. It detects the canal terminus by figuring out a sudden change within the dominant characteristic (capacitive or resistive) of the impedance. It is the successor to the Sono Explorer line of apex locators and makes use of a selection of frequencies to sample the canal, using the best two for its reading. The unit is mounted with a root canal graphic displaying the file place and has an audible signal. Fourth-generation apex locators Fourth-generation gadgets measure and compare the advanced electrical attribute options of the root canal at two or more frequencies of electrical impulses [7, 36]. There can be different combinations of values of capacitance and resistance that determine the same impedance (and thus the identical apical constriction reading). In addition, the gadget named Elements makes use of a lookup matrix quite than making any inside calculations. The producers claim that by doing this and by then calculating the standard deviation of the variations between the 2 frequencies, they increase the accuracy of the device [7]. The fourth-generation apex locators are marketed by Sybron Endo and embody the Apex Locator and the Elements Diagnostic Unit. Both are ratio-type apex locators that decide the impedance at 5 frequencies, and Chapter four: Determination of working length a hundred and one both have built-in digital pulp testers. The Ray-Pex 4 and 5 (Forum Engineering Technologies, Rishon Lezion, Israel) are also examples of this era. The signals go through a digital-to-analog converter to be converted into an analog signal, which is then amplified and passed to the patient circuit mannequin, which is assumed to be a resistor and capacitor in parallel. A significant disadvantage of this era is that they should perform in comparatively dry or in partially dried canals [49]. When utilizing the Elements Diagnostic Unit, the clinician ought to withdraw the file to the 0. The system is supplied by a diagnostic desk that features the statistics of the values at completely different positions to establish the position of the file. Devices employing this method experience appreciable difficulties while working in dry canals; due to this fact, additional insertion of irrigants or lubricants are required [68]. During medical work it was noticed that the accuracy of electronic root canal length measurement varies with the pulp and periapical condition [69]. Thus, pulp condition and periapical ailments must be considered to consider the accuracy of apex locators. Sixth-generation digital apex locators So far, five generations of instruments have been created that continually evolve and are being improved. The objective is to adapt to the manner of measuring in accordance with the precise characteristic options of the environment to measure [69]. The adaptive apex locator constantly defines humidity of the canal and immediately adapts to dry or moist canal. This method it can be utilized in dry and in wetted canals, in canals with blood or exudates, and in canals in which the pulp has not yet been extirpated. Depending on the continuously measured moistness, and completely by itself, the system adapts the measuring technique for either a dry or a wet canal. Other uses of apex locators All fashionable apex locators are able to detect root perforations to clinically acceptable limits and are equally able to distinguish between large and small perforations [70]. Suspected periodontal or pulpal perforation during pinhole preparation can be confirmed by all apex locators, as a result of a patent perforation will cause the instrument to complete a circuit and indicate the instrument is beyond the apex [11]. Furcation perforations may be detected if "Apex" is registered immediately upon file insertion into a would-be canal.
While the basis canal isolate was essentially the most delicate strain within the first examine antibiotics medicine ciloxan 250 mg purchase with mastercard, there was no distinction among the same strains in a follow-up research antibiotic resistance the last resort cheap 750 mg ciloxan with visa. It was concluded that the type of antimicrobial susceptibility take a look at would possibly affect the outcomes of the studies when evaluating the antifungal capacity of the brokers or resistance of the strains antibiotics for uti levaquin ciloxan 750 mg discount. The incidence of yeasts in major, secondary, or persistent endodontic infections has been reported to be within the vary of zero. However, it should be stored in thoughts that all of those studies have been completed in systemically healthy dental subjects. Considering that the presence of yeasts in oral and dental tissues of immunocompromised patients is relatively larger than that of the healthy inhabitants, it could be proposed that their incidence may even be greater within the root canals of these patients. At this level, we ought to always proceed looking for new remedies not only against micro organism, but also against fungi in endodontics. Cultivable microbiological flora associated with persistent periapical illnesses and coronal leakage after root canal treatment: a preliminary examine. The impact of antifungal brokers on floor properties of poly(methyl methacrylate) and its relation toadherence of Candida albicans. Chelator-induced dispersal and killing of Pseudomonas aeruginosa cells in a biofilm. Effects of low concentrations of zinc on the growth and dimorphism of Candida albicans: evidence for zinc-resistant and -sensitive pathways for mycelium formation. Associations between salivary ranges of mutans streptococci, lactobacilli, yeasts and black-pigmented Bacteroides spp. Comparison of chosen microflora of plaque and underlying carious dentine associated with primary root caries lesions. Modification of adherence to plastic and to human buccal cells of Candida albicans and Candida dubliniensis by a subinhibitory focus of itraconazole. Action of chlorhexidine on budding Candida albicans: scanning and transmission electron microscopic research. Association of the microtubule cytoskeleton with the thigmotropic sign for appressorium formation in Uromyces. The affect of Streptococcus mutans on adhesion of Candida albicans to acrylic surfaces in vitro. Interrelations of oral microorganisms, immunoglobulins, and dental caries following radiotherapy. Comparison of the plaque microflora in immunodeficient and immunocompetent dental sufferers. Quantitative relationship between yeast and micro organism in dentureinduced stomatitis. Oral pathoses attributable to Candida albicans during chemotherapy: replace on growth mechanisms. Adhesion of u Candida albicans to varied dental implant surfaces and the affect of salivary pellicle proteins. Adherence of Candida albicans to human salivary parts adsorbed to hydroxylapatite. The impact of sodium hypochlorite and chlorhexidine on cultured human periodontal ligament cells. Microbial flora of root canaltreated teeth associated with asymptomatic periapical radiolucent lesions. Inhibition by sugars of Candida albicans adherence to human buccal mucosal cells and corneocytes in vitro. Biofilms and their position in the resistance of pathogenic Candida to antifungal agents. Microbiology and therapy of dental abscesses and periodontal-endodontic lesions. Mixed salivary glucose ranges and candidal carriage in sufferers with diabetes mellitus. Observation of Saccharomyces cerevisia in blood of patient present process root canal treatment. The effect of chlorhexidine gluconate irrigation on the basis canal flora of freshly extracted necrotic enamel. The N-terminal part of Als1 protein from Candida albicans particularly binds fucose-containing glycans. Comparative analysis of endodontic irrigants in opposition to Enterococcus faecalis biofilms. Prevalence of yeasts in saliva and root canals of enamel associated with apical periodontitis. In vitro assessment of u the effectiveness of chlorhexidine gel and calcium hydroxide paste with chlorhexidine in opposition to Enterococcus faecalis and Candida albicans. Effect of vancomycin hydrochloride on Staphylococcus epidermidis biofilm associated with silicone elastomer. Effectiveness of intracanal irrigants and medicines in opposition to the yeast Candida albicans. Effect of endodontic procedures on enterococci, enteric bacteria and yeasts in major endodontic infections. Candida colonization on the floor of orthodontic brackets and the adhesion of these strains to buccal epithelial cells. Effectiveness of 2% chlorhexidine gel and calcium hydroxide towards Enterococcus faecalis in bovine root dentine in vitro. In vitro analysis of the antimicrobial activity of calcium hydroxide combined with Fungi in Endodontic Infections 223 chlorhexidine gel used as intracanal medicament. Yeasts in juvea nile periodontitis: preliminary observations by scanning electron microscopy. Investigation of touchsensitive responses by hyphae of the human pathogenic fungus Candida albicans. Interactions of ethylenediamine tetraacetic acid with sodium hypochlorite in aqueous solutions. Colonization of the oral cavity by Candida species: risk components in long-term geriatric care. Chemical and antimicrobial properties of calcium hydroxide combined with irrigating options. Degradation of human dentine collagen by an enzyme produced by the yeast Candida albicans. Subgingival strains of Candida albicans in relation to geographical origin and incidence of periodontal pathogenic micro organism. Phenotypic and genotypic characterization of oral yeasts from Finland and the United States. Comparison of the hydrophobic properties of Candida albicans and Candida dubliniensis. Genetic similarity and phenotypic variety of commensal and pathogenic strains of Candida albicans isolated from the oral cavity. Interactions of Candida albicans with bacteria and salivary molecules in oral biofilms. Clonal identity of Candida albicans within the oral cavity and the gastrointestinal tract of pre-school children. Candida yeasts in persistent periodontitis tissues and subgingival microbial biofilms in vivo. Coaggregation of Streptococcus sanguis and other streptococci with Candida albicans. The effects of sub-inhibitory concentrations of cationic, non-antibiotic, antimicrobial brokers on the morphogenesis of Candida albicans in vitro. Comparative adherence of Candida albicans and Candida dubliniensis to human buccal epithelial cells and extracellular matrix proteins. Isolation and traits of collagenolytic enzyme produced by Candida albicans. Influence of surface traits on the adhesion of Candida albicans to varied denture lining materials.






