Rumalaya liniment
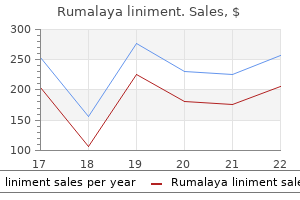
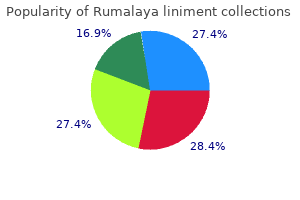
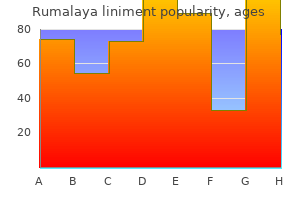
Rumalaya liniment
Rumalaya liniment dosages: 60 ml
Rumalaya liniment packs: 1 bottles, 2 bottles, 3 bottles, 4 bottles, 5 bottles, 6 bottles, 7 bottles, 8 bottles, 9 bottles, 10 bottles

They must be made conscious of the need for maintenance procedures to retighten the sutures on a yearly basis muscle relaxant bruxism rumalaya liniment 60 ml generic free shipping. The proponents of this method declare that it allows for reliable elevation of the malar fats pad in a relatively easy way muscle relaxant xanax rumalaya liniment 60 ml line. The morbidity is minor muscle relaxant antidote rumalaya liniment 60 ml with visa, and the procedure can be simply reversed, augmented or modified. A second mark is placed 1 cm inferolaterally alongside a line that passes via the primary dot and is parallel to the nasolabial fold. A 3 cm temporal incision is made on the path crossing these markings, 2 cm behind the headline. Through stab incisions alongside the relaxed pores and skin pressure strains over the inferior marks, the Keith needles are handed directed to the marks lateral to the orbital rim. The needles are retrieved via the temporal incision and the suture is fixated into the deep temporalis fascia. The outcomes are normally thought of good by the proponents of this system, with a high diploma of patient satisfaction. Complication rates ranges from 10 to 19%,77�79 the commonest of it, is cheek asymmetry, which was found to settle throughout the first three months. Barbed sutures are everlasting sutures which have small projections that radiate outward from the suture. They are often made of a 2-0 polypropylene materials and after the barbs are made the core becomes equivalent to a 4-0 suture. The suture is launched into the tissue in the different way of the barbs so the suture glides simply along the trail; and, when the suture is gently pulled, the barbs will then interact the surrounding soft tissue. This system was primarily based in a 2-0 polypropilene suture with barbs in opposing instructions began on the middle. In the preliminary report, no clear objective measurement was provided, and it was unclear how many patients had prolonged follow-up. Another examine, nevertheless, reported that most sufferers had a "completely passable end result" with about 60% sustaining their initial correction after 12 months. The period of time required for stabilization of the suture with the encircling tissues is unclear and also prone to be variable amongst individuals. The few clinical research obtainable lack evidence for confirming the claims of affected person satisfaction and the longevity of effect. Nevertheless, for the majority of surgeons, the carry was considered to be brief lived and was extensively deserted. Transorbital Approach for Mid-face Lift In 1998, Hester42 described a way for midface elevation via a lower blepharoplasty method. Its proponents exalts that, since midface growing older usually occurs from the lower eyelid to the perioral area, the surgeon can with a single publicity counteract the effects of soft-tissue descent. The dissection is carried on a suborbicularis and preseptal plane to the inferior orbital rim. The deep temporal fascia is encountered by dissecting laterally and superiorly to the lateral canthus in a supraperiosteal airplane. At the level of the rim, the periosteum is incised and subperiostal dissection is carried inferiorly below the origin of the zygomaticus minor and main. The infraorbital and the zygomaticofacial nerves are identified and preserved through the subperiosteal elevation. Laterally, the dissection proceeds to the anterior portion of the zygomatic arch extending superolaterally to just above the lateral canthus. At the inferior end of the dissection, the periosteum is again incised to facilitate mid-facial delicate tissue launch. Following this incision, bimanual manipulation is completed to ensure that all the constraints to the elevation are free. Most commonly, quite than excised, the fat pads are draped over the inferior orbital rim to augment soft-tissue coverage. This coverage is achieved by suturing this tissue to the posterior side of the cheek flap. Once all these preliminary maneuvers are carried out, the mid-face soft tissue is repositioned and fixated to the deep temporalis fascia posterior to the orbital rim at some extent just above the lateral canthus. The undermined skin-muscle flap elevated with the subciliary strategy is then re-draped, and its extra removed. The tarsal plate is fixated into the inside aspect of the orbital periosteum, inserting the lower lid at about 1 to 2 mm above the inferior limbus. Advocates for this system declare that has the advantage of its dissection to avoid threat to branches of the facial nerve and create a vertical vector of pull, avoiding the danger of a "lateral sweep" that would occur with a more lateral strategy. Moreover, help with both a canthopexy or canthoplasty has to be fastidiously thought-about. The want for canthoplasty in a number of patients brings concerns due to the danger for lower-lid shortening and creation of an unnatural look, which is why surgeons adept to this method extra often choose canthopexy instead. The authors acknowledge a high incidence of issues, mostly within the lower lid. This excessive price of complications has led them to suggest a quantity of modifications to the approach to achieve extra pure outcomes with less frequent issues. This method has not gained the recognition of the trans-temporal endoscopic approach. While a significant number of problems that could be challenging to appropriate occur with the trans-orbital method, the trans-temporal route offers plentiful help for the lower eyelid and increase in lower-lid tension. In addition, it prevents bunching within the malar area and avoids incisions that traverse the orbicularis oculi. The trans-temporal, also identified as endoscopic mid-face lifting, is our preferred approach. Multiple planes of dissection should be traversed, and a thorough understanding of the anatomy of the fascial planes within the temporal/zygomatic region, as described beforehand, is a prerequisite to avoid damage to the frontal department of the facial nerve. The patient is examined preoperatively in an upright position, and the forehead is assessed. The amount of desired medial brow elevation is measured; in most patients with mild to average forehead ptosis, 2 to four mm of brow elevation is required to convey the medial side of the forehead to the extent of the supraorbital rim. When making the incision, the surgeon has to bevel the scalpel parallel to the hair follicles, to obtain maximal scar camouflage as transecting the hair follicles leads to a few millimeters of permanent alopecia. The incision is carried down via the superficial temporal fascia to the deep temporal fascia. A dissector is used to elevate the superficial temporal fascia and overlying tissue off the deep temporal fascia to the temporal line. The dissection is continued superiorly in a subperiosteal airplane after dissection through the tenacious fascia of the temporal line and ends at the degree of the occiput. This dissection ensures that the elevated brow and lateral temporal tissues will redrape and not bunch anteriorly once suspended. Inferior to the incision, dissection on top of the deep temporal fascia is performed blindly for two to 3 cm. The temporal line is marked after palpating the temporalis-muscle contraction because the patient clenches his or her enamel. The medial incisions for forehead suspension are marked a number of millimeters behind the hairline centered over the lateral canthus and lengthen posteriorly for 2 cm. Markings are placed at the supraorbital notches on the Pitanguy line as drawn out as beforehand described. The arcus marginalis often could be released from lateral to within 1 cm of the superficial marking made for the supraorbital neurovascular bundle. Bimanual dissection typically is helpful, and the hand positioned on the surface of the skin helps prevent injury to the orbit with inferior dissection. The medial incision is then made right down to the frontal bone, and screw holes are drilled. This approach allows actual measurement of the quantity of brow elevation from the preoperative brow position. The suspension interprets into the quantity of medial brow elevation, as the forehead flap between the 2 medial incisions strikes as a sheet superiorly and translates primarily to the mid- and medial forehead. We use temporary fixation with chrome steel screws which are eliminated one week after surgery.
Although the step-off deformity is a common complication of the over-resected nasal hump (since over-resected nasal bones can seldom be narrowed sufficiently) muscle relaxant before massage cheap rumalaya liniment 60 ml mastercard, the deformity can be seen in patients with a normal rhinion projection spasms post stroke rumalaya liniment 60 ml order on-line. In these sufferers muscle relaxant brand names rumalaya liniment 60 ml purchase with amex, the steady bony vault remains wider than the pinched cartilaginous vault producing a disparity in nasal width. Treatment of the inverted-V deformity entails restoration of dorsal height (when appropriate) and elimination of the nasal sidewall width discrepancy. This can be achieved by bodily narrowing the bony vault if bony infracture is cosmetically acceptable. Alternatively, the cartilaginous sidewall can be repositioned utilizing cartilage augmentation grafts to remove pinching of the middle vault. Spreader Grafts Perhaps one of the versatile and essential grafts in rhinoplasty is the spreader graft. When placed endonasally, spreader grafts are immobilized by creating a exact longitudinal pocket beneath the upper septal mucoperichondrium. When placed by way of the exterior rhinoplasty approach, spreader grafts can be sutured directly to the dorsal septum with mattress sutures at each ends. In revision rhinoplasty, relying upon the deformity at hand, grafts may be applied to one or each parasaggital spaces to present will increase in mid-vault width, improved rigidity or alignment of the dorsal septum, or small increases in height of the dorsal septum. When prolonged caudally, the spreader graft becomes a septalextension graft able to elongating the foreshortened nose. Although spreader grafts have quite a few beauty functions, placement of bilateral spreader grafts will do little to increase nasal valve patency in sufferers with lateral nasal sidewall collapse since only modest lateralization of the upper nasal sidewall is achieved. However, a variation of the traditional spreader graft, generally identified as the butterfly spreader graft, uses an oval- or trapezoid-shaped cartilage onlay graft to carry the collapsed lateral nasal sidewall utilizing the inherent spring of the flexed cartilage graft. The butterfly spreader graft can also be used to augment the center vault profile in sufferers with modest saddle nostril deformities. Dressing Once the varied maneuvers of the surgical procedure are complete and wound closure has concluded, dressing of the nostril is performed promptly to restrict swelling and keep alignment of the fragile nasal framework. Sterile tape is applied across the dorsum and across the lobule followed by a molded plastic or contoured aluminum splint. Blood pressure control is closely maintained and anti-emetic precautions are continued. Ice packs are applied intermittently for one to two days, and elevation of the pinnacle is continued for 2 to three weeks. Vigorous exercise, heavy sun exposure, sun shades, and platelet-inhibiting medications are all avoided for several additional weeks until acute inflammation subsides. Revision Rhinoplasty Without doubt, a few of the most vexing problems in nasal surgical procedure outcome from the necessity for revision rhinoplasty. Severe collapse of the nasal skeleton, often accompanied by symptomatic nasal airway obstruction, can challenge even the most gifted rhinoplasty surgeon. However, even daunting anatomic deformities can be overshadowed by the turbulent emotional issues which attend the patient needing revision. Instead of the promised end result of a beautiful new nostril, the patient must first address the preliminary shock and disappointment of a newly acquired physical deformity. Coupled with sizeable investments in money and time, the ensuing emotional responses range from shame and embarrassment to anger and distrust of the medical group. Moreover, many sufferers report serial rhinoplasty failures, having undergone multiple unsuccessful revisions, every yet one more disfiguring and extra disappointing than the final. Not surprisingly, most patients needing revision rhinoplasty are apprehensive and reluctant to risk further nasal surgery without sufficient justification, assist, and encouragement. Sadly, the overwhelming majority of failed rhinoplasties are the outcomes of surgical error, whereas poor therapeutic tendencies account for the remainder. Although an incomplete operative procedure is often liable for the unsatisfactory consequence, (for instance, a residual hump,) over-aggressive excision of the nasal skeleton is a a lot more frequent cause of the unsatisfactory rhinoplasty outcome. Indeed, badly misshapen cartilage, gross skeletal asymmetries, and overresected bony remnants are the standard findings in the multiply-operated nose. To make issues even worse, surplus septal or auricular cartilages necessary to graft the collapsed nostril are sometimes absent, having been depleted during earlier makes an attempt at surgical restoration. Because misguided makes an attempt at surgical restore only enlarge the surgical challenge, complex revision surgical procedure must be reserved for the accomplished rhinoplasty surgeon with abundant experience in revision rhinoplasty. For advanced revision circumstances, the exterior rhinoplasty approach is obligatory; and sluggish, deliberate, and meticulous dissection are required to expose the skeletal remnants without inflicting additional injury. Emphasis is positioned upon first restoring the midline skeletal constructions of the dorsal septum and columella. Once the central assist structures are reconstituted, lateral skeletal parts of the middle and decrease vault are then suspended from the central advanced to restore width, symmetry, and airway patency. When necessary, lacking or severely damaged skeletal components are reconstituted with substitute grafts of similar tissue sort. Onlay augmentation grafts of cartilage and/ or soft tissue are then used to good and refine the outer-nasal contour. Because augmentation grafts are associated with donor website morbidity and are typically in brief provide, the experienced surgeon will use these materials in a inventive and smart manner to conserve tissue and optimize the surgical end result. Moreover, the results of preexisting scar tissue must be anticipated, and compensatory measures have to be applied every time potential to forestall delayed skeletal distortion from shrink-wrap contracture. Although failed rhinoplasty appears to be a rising downside worldwide, the vast majority of revision sufferers may be restored to a standard, if not attractive-nasal contour, when appropriate reconstructive techniques are undertaken. However, a "perfect" nostril is all but unimaginable, and careful evaluation of the deformity, tissue characteristics, healing capability, and affected person motivation are essential to determine the prognosis for a successful outcome. Of notice, a small minority of patients needing revision rhinoplasty possesses unusually poor therapeutic traits and should expertise unfavorable outcomes even when the operation is executed correctly. Signs of unfavorable therapeutic response, such as hypertrophic scarring, cicatricial stenoses, ischemic tissue loss, and so forth, ought to be diligently sought; and, when recognized, these patients must be counseled accordingly. On the opposite hand, sufferers with favorable therapeutic tendencies have an excellent prognosis when correct surgical method is mixed with abundant and quality graft materials. For this reason, surgical consent for all anticipated graft supplies is essential. The time-honored adage "as goes the septum, so goes the nostril" underscores the importance of correcting septal deformities to achieve a symmetric and cosmetically appealing nasal contour. Because a uncared for septal deviation may prohibit correct realignment of the scoliotic nostril, septal deformities are greatest corrected prior to management of the deviated bony vault. Septal surgery has been historically regarded as a useful self-discipline, however its mastery is equally essential for the beauty surgeon. Because the nasal septum supports each the interior nasal airway and the external nasal framework, deformities of the nasal septum may cause functional disturbances, cosmetic disturbances, or mixtures therein. When confined to the inner nasal septum, functional disturbances are normally treated by way of septoplasty without alteration of the exterior nasal contour. In distinction, functional disturbances of the septum are frequently accompanied by seen deformities of the outer nostril, and rhinoplasty methods may be required to remove both the practical and aesthetic problems. In both case, care must be taken to protect adequate septal support since an overaggressive septoplasty or an overzealous rhinoplasty can lead to symptomatic nasal obstruction from unsightly skeletal collapse. Since joint beauty and functional disturbances are anatomically interrelated, combined therapy with septorhinoplasty sometimes offers the most effective technique of evaluating and eliminating advanced septal deformities. Moreover, as a outcome of discount rhinoplasty will inevitably diminish breathing area, correction of coexisting airway blockage is usually wanted to stop symptomatic nasal airway obstruction arising from a purely aesthetic process. Combined therapy is also preferable since it spares the patient from the extra discomfort, down-time, and expense of a second operation. Although the nasal septum is commonly thought to be a practical entity, complicated septal deformities almost always affect nasal cosmesis; and correction of external septal deformities usually improves nasal contour. Clearly, septoplasty and rhinoplasty are permanently intertwined, and septal deformities must be regarded as an anatomic malformation with variable cosmetic and functional manifestations. The nasal septum is a skeletal partition that bisects the nasal cavities in the midline-sagittal airplane. However, the "regular" nasal septum, found inside a healthy nostril, is seldom perfectly straight. Minor septal irregularities are typical and must be thought-about surgically inconsequential offered they create no symptomatic obstruction and produce no external nasal deformity. The exception to this rule is the functionally delicate nasal valve region where even minor septal deformities can produce vital will increase in nasal airway resistance. The exterior border of the upper part of the nasal septum, known as the dorsal septum, is the structural basis for the nasal bridge. Deflections, scoliosis, or saddle deformities of the dorsal septum could severely compromise aesthetics of the nasal bridge and/or patency of the nasal valve.
Early craniofa muscle relaxant high rumalaya liniment 60 ml generic with visa, cial morphology and progress in children with unoperated isolated cleft palate spasms gerd discount rumalaya liniment 60 ml line. Cephalometric evaluation of the posterior airway house in patients with cleft palate after palatoplasty spasms down left leg rumalaya liniment 60 ml buy discount line. Sleep-related breathing disorder in Duchenne muscular dystrophy: illness spectrum in the paediatric population. Surgical remedy of obstructive sleep apnea in neurologically compromised sufferers. Prader-Willi syndrome: finding out the relationships between obesity, hypersomnia, and sleep apnea. Intranasal budesonide therapy for youngsters with delicate obstructive sleep apnea syndrome. Montelukast for youngsters with obstructive sleep apnea: a double-blind, placebo-controlled research. Montelukast, a leukotriene receptor antagonist, for the therapy of persistent asthma in children aged 2 to 5 years. Safety and tolerability of montelukast in placebo-controlled pediatric studies and their open-label extensions. A modified monobloc for the remedy of obstructive sleep apnoea in paediatric sufferers. Effect of a high-flow open nasal cannula system on obstructive sleep apnea in children. Randomized, double-blind medical trial of two completely different modes of optimistic airway strain therapy on adherence and efficacy in children. Updated systematic review of tonsillectomy and adenoidectomy for therapy of pediatric obstructive sleep apnea/hypopnea syndrome. Adenotonsillectomy for obstructive sleep apnea in kids: outcome evaluated by pre- and postoperative polysomnography. Intracapsular tonsillar discount (partial tonsillectomy): reviving a historic process for obstructive sleep disordered breathing in youngsters. Radiofrequency treatment of turbinate hypertrophy in topics utilizing steady constructive airway stress: a randomized, double-blind, placebo-controlled medical pilot trial. Improved objective outcomes and high quality of life after adenotonsillectomy with inferior turbinate discount in pediatric obstructive sleep apnea with inferior turbinate hypertrophy. Surgical correction of anatomic abnormalities in obstructive sleep apnea syndrome: uvulopalatopharyngoplasty. Effects of uvulopalatopharyngoplasty on sleep architecture and patterns of obstructed respiration. Results of sleep apnea recordings and subjective evaluation 6 months and a pair of years after surgery. The efficacy of surgical modifications of the upper airway in adults with obstructive sleep apnea syndrome. Is uvulopalatopharyngoplasty still an possibility for the therapy of obstructive sleep apnea Surgical remedy of obstructive sleep apnea in children with severe psychological insufficiency. Lingual tonsillectomy: a review of 5 years experience and evolution of surgical method. Transoral robot-assisted lingual tonsillectomy and uvulopalatopharyngoplasty for obstructive sleep apnea. Oropharyngeal stenosis: a complication of multilevel, single-stage higher airway surgical procedure in children. Radiofrequency ablation for the therapy of obstructive sleep apnea: a meta-analysis. Neonatal and toddler mandibular distraction as a substitute for tracheostomy in extreme obstructive sleep apnea. A fall of the bottom of the tongue thought of as a model new cause of nasopharyngeal respiratory impairment: Pierre Robin sequence, a translation. Obstructive sleep apnea syndrome and perioperative issues: a systematic review of the literature. Practice pointers for the perioperative management of patients with obstructive sleep apnea: a report by the American Society of Anesthesiologists Task Force on Perioperative Management of sufferers with obstructive sleep apnea. Non-steroidal anti-inflammatory medication and perioperative bleeding in paediatric tonsillectomy. Dexamethasone and postoperative bleeding after tonsillectomy and adenotonsillectomy in children: a meta-analysis of prospective research. Perioperative dexamethasone administration and risk of bleeding following tonsillectomy in children: a randomized controlled trial. The position of the genial bone development trephine system along side uvulopalatopharyngoplasty in the multilevel management of obstructive sleep apnea. Any condition or anatomic anomaly that disrupts the components of regular deglutition may end up in dysphagia. If a baby is unable to adapt to the continuous adjustments that happen in oral anatomy in the course of the first several years of life, or if neuro logic operate is impaired, the swallow shall be compromised. The improved survival rates of untimely infants and those with complicated medical condi tions affecting the construction and performance of the swallowing mechanism have led to an elevated incidence of pediatric dysphagia1�4 and the con comitant probability of encountering dysphagic sufferers in clinical practice. This article pro vides an overview of the swallowing course of, touching upon airway protective mechanisms and the incessantly associated issues of aspira tion and sialorrhea (drooling). Impact of Anatomic Changes In early infancy, oral anatomy facilitates suck ling, a reflexive activity regulated at the subcor tical stage. Suckling is characterised by rhythmic extension and retraction motions of the tongue. The small size and form of the oral cavity relative to the tongue facilitates early suckling in addition to the gradual improvement of more mature sucking abilities during the first four months of life. The oral cavity varieties a relatively rigid suction chamber with thick buccal fats pads laterally and the palate superiorly. The buccal fats pads present lateral stability, and the tongue fills most of this sucking chamber, contacting all surfaces. The nipple is drawn into the oral cavity and the lips seal over the nipple anteriorly while the tongue seals towards the palate posteriorly. The mid tongue descends in a pistonlike movement, making a negative pressure in the oral cavity. As toddler suckling transitions into mature suck ing, lip closure on the nipple increases and tongue movements turn into vertical with accompanying slight vertical motion of the jaw, resulting in improved sucking efficiency. The adjustments in vary and variation of total tongue motion assist the eventual transition to ingestion of food apart from liquid. In infants, the larynx is in a high position within the neck, residing adjacent to the cervical verte brae C1 to C3. This allows the epiglottis to pass superior to the free margin of the taste bud, pro jecting into the nasopharynx. The excessive place of the larynx functionally separates the respiratory and digestive tracts till 4 to six months of age in time period infants (or the ageadjusted equiva lent in preterm infants) by minimizing the overlap of the hypopharyngeal airway and the digestive tract. This position forces a bolus to divert across the epiglottis because the pharynx fills with the bolus and contracts sequentially for swallowing. Preterm infants (< 32 weeks of gestation) lack the ability to coordinate suck ing, swallowing, and respiration due to neurologic cessation of respiration throughout swallowing and minimizes the risk of aspiration. Over time, the outstanding buc cal pads lower, the oral cavity becomes bigger, and the relative dimension of the tongue decreases. More house is available for differentiated tongue actions in addition to softpalate motion. During this gradual descent, help is provided by elevated neuro muscular control of the structural components of the hypopharynx, as opposed to the positional stabil ity offered earlier by the proximity of structures. Maintenance of continued airway protection dur ing swallowing is determined by normal neuromuscu lar development. Both mechanoreceptors and chemoreceptors throughout the laryngeal and pharyngeal walls are associated with this reflex. The glottic closure response is initiated at the nucleus ambiguus, which sends an efferent sign through the vagus nerve to the recurrent laryngeal nerve. This signal leads to adduction of the true and false vocal folds and protects the air means. Neural impairment or a structural irregular ity that interferes with glottic closure can hinder this airway protective mechanism and leave the kid at increased danger of aspiration with feeding. During maturation of the swallow response, extra anatomic modifications occur along side the development of neuromuscular head and neck management.
Details of this flap as a free tissue switch flap are lined later in this chapter spasms in your back purchase rumalaya liniment 60 ml amex. As a pedicled rotational flap for reconstruction of the neck or inferior scalp defects spasms near kidney 60 ml rumalaya liniment order with visa, the latissimus dorsi muscle has a wide range of rotational motion and may be employed even when the muscle remains connected at its insertion on the humerus muscle relaxant guardian pharmacy purchase rumalaya liniment 60 ml without a prescription. When reconstruction with a pedicled flap is feasible, the requirement for microvascular anastomosis is eradicated, reducing operative time and the need for technical expertise. The donor defect can usually be closed primarily, avoiding the need for a pores and skin graft. As a pedicled flap essentially the most vital disadvantage is the limitation in positioning of the flap in the recipient website. The place of a pedicled flap is restricted by the arc of rotation of the muscle and the orientation of the vascular pedicle, so the final positioning of the pedicled flap is much less versatile than when the flap is transferred as a free flap. The thick pores and skin of the cutaneous paddle (up to four mm) and its poor shade match with the pores and skin of the top and the neck, although acceptable, reduce the subtlety of this flap within the recipient web site. The blood provide to this kind of flap relies on prefascial and subfascial plexuses at the subcutaneous level. Typically, these stem from regional arteries that feed the subcutaneous plexus through musculocutaneous or septocutaneous perferators. Examples by which a pedicled fasciocutaneous flap would be required for reconstruction would include massive skin only defects of the neck or parotid area, for facial contouring or intraoral defects, or to be used in stomaplasty. Reportedly, flap size could be as giant as 24 cm, which extends over the deltoid muscle and into the upper arm. The advantages of the flap embody a minimal donor site morbidity (usually closed primarily) and ease of harvest. The flap is a true island flap and is pedicled on the supracavicular fatty tissue, Moving the distal end of the flap to reconstruct the defect includes propellering/rotating the flap across the vascular pedicle. The flap can be utilized to reconstruct surface defects of the neck quite easily and with good success. While the colour match is great the lack of muscle bulk and tenuous provide to probably the most distal end of the skin paddle make it a secondary choice for reconstruction in most surgeons armamentariums. It has reportly been used for pharyngeal reconstruction with fistula rates (3 out of 9 patients) just like reported literature. The use of free tissue from a distant site permits for reconstruction with comparable tissues. In general, one can envision the three dimensional defect that will be created after resection of the neoplasm. Knowledge of varied tissue elements of varied free tissue transfer flaps will enable the reconstructive surgeon to select a flap that can greatest mimic the volume as well as the tissue composition of the resected tissue. Even with this capacity, sufferers should be made aware that multiple revisions are sometimes essential to obtain the desired practical as nicely as cosmetic objectives. Although over 40 donor sites at no cost tissue transfer have been described and utilized, a smaller quantity have been persistently utilized for routine reconstruction of huge head and neck defects. The radial forearm fasciocutaneous, radial forearm osteocutaneous, and fibular osteocutaneous free flaps account for over 80% of head and neck microvascular reconstructions. This is due largely to the particular advantages of the traits of those flaps that embody versatility, high success fee, and low donor-site morbidity. Function of the flap in the recipient web site is also thought of, as nerve anastomosis may be carried out to reestablish sensation and mobility to transferred tissue. This is especially related in reconstruction of the oral cavity, wherein sensation and mobility may be restored to a reconstructed tongue, significantly bettering postoperative perform. With all these components thought-about, surgical flaps are divided into a quantity of classes based mostly on the type of tissues included in the flap: fasciocutaneous, myocutaneous (musculocutaneous), myogenous, and osteocutaneous. Each of these categories shall be mentioned, with examples of reconstructive choices out there within every class. Fasciocutaneous Flaps the fasciocutaneous flap is a composite flap that features pores and skin, subcutaneous tissue, and fascia. The blood provide to the fasciocutaneous flap sometimes consists of perforating vessels arising from regional arteries coursing through fascial septa, often identified as septocutaneous perforators. Cadaveric studies have demonstrated that the fasciocutaneous perforators and their fascial plexus lie in the longitudinal axis, and therefore the length-tobreadth ratio is dictated by a longitudinally oriented pattern of blood flow. Fasciocutaneous flaps have the advantage of being thin and pliable and performance nicely for reconstruction of low volume, moderate surface space defects. Many totally different areas of the physique are appropriate for harvesting of a fasciocutaneous free flap (Table 64-1). The radial forearm fasciocutaneous flap may be elevated as an osteocutaneous flap, inclusive of a segment of vascularized radius bone. This flap relies on the radial artery with its paired venae comitantes and/or the cephalic vein (Table 64-2). The vascular pedicle is long (up to 20 cm) and the vessels are of huge caliber (2. This allows a selection of orientations while sustaining adequate pedicle length for vascular anastomosis to the bigger caliber exterior carotid branch vessels in the neck (facial, superior thyroid, or lingual arteries). The radial artery, with its paired venae comitantes, programs in the lateral intermuscular septum and has several fascial branches within the forearm that provide the fascia and skin. The proximal extent of the pedicle is defined by the radial recurrent artery and by the convergence of the 2 venae comitantes right into a single vein, which happens close to the antecubital fossa in over 80% of sufferers. The skin paddle is incised within the distal forearm, and the dissection is taken to the subfascial degree. The cephalic vein may also be harvested to supplement superficial venous drainage of the flap. When a sensate flap is desired, for example, for tongue reconstruction, the lateral antebrachial cutaneous nerve is recognized because it programs close to the cephalic vein and is harvested along with the vascular pedicle for anastomosis at the recipient site. Once the flap is completely divided from the forearm, the flap is fastidiously inset into the recipient site and vascular anastomosis is carried out underneath the microscope. The forearm donor site is roofed with a splitthickness pores and skin graft and a volar splint is left in place for 5 days postoperatively. Five to fifteen % of sufferers may have no much less than partial lack of the pores and skin graft. Functional deficits within the donor arm are unusual, with a prospective examine demonstrating some extent of practical deficit in the donor arm in 16% of patients at 1 12 months. This could also be attributable to operative trauma to the nerve, traction damage, or ischemia associated to tense closure of the surgical site. A devastating complication of radial forearm free flap elevation is the event of hand ischemia. Critical to the number of donor website is the accurate performance of a preoperative Allen test. This take a look at is an easily executed medical examination that evaluates the perfusion of the hand by each the ulnar and the radial arterial techniques. The radial artery may not be harvested safely in sufferers with an incomplete palmar arch or compromised perfusion by the ulnar artery, and alternate reconstructive choices should be explored. The ulnar fasciocutaneous free flap shares lots of the advantageous characteristics of the radial forearm fasciocutaneous flap (see Table 64-2). The ulnar flap could additionally be selected when preoperative bodily examination (Allen test) of the nondominant hand is suggestive of insufficient radial arterial perfusion. In this setting, reconstructive surgeons typically elect to pursue harvest of a radial forearm free flap from the dominant facet. As a result, this flap may be elevated more quickly than do more technically challenging free flaps such as the anterolateral thigh flap. Elevation of the flap can typically be performed simultaneously with the resective process when a two-team strategy is applied. These factors lead to shorter operative times, decreased anesthetic time for the patient, and decrease working room prices. The main drawback related to use of the radial forearm free flap is unacceptable cosmetic look of the forearm following flap harvest and pores and skin grafting. A latest examine demonstrated the ulnar flap is predicated on the ulnar artery and its two venae comitantes. The dimensions of the vascular pedicle are quite consistent, with average ulnar artery diameter measuring 2. Pedicle length is persistently greater than 10 cm, which allows for versatility in positioning the flap in its recipient location. Advantages of the ulnar flap, like its radial counterpart, are its reliable, soft, pliable, and moldable in three dimensions characteristics and possibility of further bulk with inclusion of the underlying palmaris longus tendon.
Other predisposing elements embody race spasms vs fasciculations 60 ml rumalaya liniment buy with amex, pores and skin sort back spasms 26 weeks pregnant 60 ml rumalaya liniment cheap amex, and prior history of abnormal scarring muscle relaxant lodine purchase 60 ml rumalaya liniment fast delivery. Most generally positioned within the postauricular area, these scars often develop in the first three months after surgery. Initial remedy consists of intra-lesional corticosteroid injections (triamcinolone 5 to 10 mg/mL) at threeweek intervals. Excision of those scars should be delayed for six to 12 months, and potential recurrence of lesions could be lessened with considered use of deep sutures. Alopecia and Earlobe Deformity Alopecia is usually as a end result of extreme closure line rigidity causing transient shock of the hair follicles (telogen effluvium). The use of hair transplantation strategies can additionally be employed to fill in bare areas or restore lack of the temporal tuft. Post rhytidectomy earlobe deformity (pixie ear) can be a sequelae of poor incision placement, malpositioning of the lobule at closure, and tension on the closure. Correction of this complication could be challenging, usually requiring an development flap technique with closure rigidity supported by deeper layers. The subsequent formation of a glandular pseudocyst (sialocele) or salivary fistula is seldom seen however is a possible concern. If parotid parenchyma is exposed during the dissection, the overlying fascia ought to be sewn over the defect. Postoperative seroma formation in the space of the mandibular angle should elevate suspicion of sialocele formation. Conservative measures such oral anticholinergics, serial aspirations and strain dressing are first line therapies, with intra-glandular botulinun toxin injections reserved for refractory sialoceles. A thorough understanding of the relevant anatomy coupled with an correct preoperative analysis of the growing older anatomy are important to determine which procedures are to be beneficial in addition to reaching the optimum surgical result. Neck Recontouring with suture suspension and liposuction: another for the early rhytidectomy candidate. Improving surgical procedure on the getting older neck with an adjustable expanded polytetrafluoroethylene cervical sling. I even have one myself above my left knee which is a perfect map of the London Underground. Facial scars, in particular, could be emotionally devastating and will affect selfesteem in some patients. The goal of scar revision is to reorient the scar for maximal camouflage, to not simply "take away" the scar. Most scar revision methods require excision of tissue and repositioning of the scar. This is often carried out on mature scars a minimum of 6 to 12 months after the preliminary damage. The scar is excised sharply, undermined within the subdermal aircraft, and closed meticulously in a layered style. Occasionally, scar tissue is left within the deeper planes to stop a concavity within the skin from delicate tissue loss. After six to eight weeks, the tissue has regained enough power and elasticity to undergo one other excision. These excisions are carried out every six to eight weeks till the scar is totally removed. The results of serial excisions is to produce one slender scar which is cosmetically acceptable. Techniques to lessen rigidity on the closure, such as subcutaneous sutures or taping, can lower the possibility for postoperative widening of the model new scar. Dissection ought to be carried out within the subdermal airplane for ease in flap transposition. When a multiple Z-plasty method is performed, the ultimate scar is lengthened, the scar is irregularized for maximal camouflage, and wound tension is extra evenly distributed within the final scar. Multiple Z-plasty excisions can be used to improve pincushioned or trap-door deformities. Each limb of the triangle ought to be roughly 3 to 5 mm in length and the base of the triangle must be approximately 5 mm in width. The triangles become slightly smaller on the ends of the wound to permit closure with out standing cone or "dog ear" formation. The scar itself could be excised with the W-plasty design or can be excised before the flaps are designed. The wound edges are undermined and closed in a layered trend to minimize wound tension. The resultant scar is normally barely longer than the unique scar which aids in the prevention of standing cones. Running W-plasty strategies have been used to camouflage coronal browlift incisions, particularly within the frontal hairline. They are additionally used to enhance the looks of long linear facial scars, brow vertical scars, and alongside concave facial areas which have formed a webbed scar. Each limb ought to be three to 7 mm in size as a result of longer limbs turn into tough to camouflage and shorter limbs produce flaps that are difficult to shut. Next the geometric shapes are drawn in each segment, together with its mirror picture on the alternative aspect. Dermabrasion could also be carried out on mature scars, similar to acne scars or scars with elevated and uneven wound edges. The technique involves using a low pace powered sanding burr (either wire brush or diamond fraise) to aircraft down the scar. The endpoint of sanding is usually when pinpoint bleeding is famous from the capillary plexus of the dermal papillae. Scarring could additionally be worsened if dermabrasion is carried out too deeply into the reticular dermis. Postoperative Wound Care Poor postoperative wound care can contribute to a poor surgical result. Adhesive strips (Steri-strips) may be placed to minimize wound tension within the early postoperative interval. The affected person is generally seen at one week, when the non-absorbable pores and skin sutures are eliminated. The triangles on the ends of the design are drawn progressively smaller to stop standing cone deformities. Nonsurgical Treatments for Scars Depressed scars may be improved by means of filler brokers like collagen and hyaluronic acid. The use of filler brokers in these scars removes the shadowing effect from the depressed scar and improves cosmesis. The surgeon can pull the pores and skin taught and if the scar elevates, it doubtless shall be improved by filling the dermis and subcutaneous tissues. Keloids and hypertrophic scars end result from irregular deposition of collagen and glycoprotein throughout wound healing. Wounds closed underneath rigidity can widen or necrose, so adequate undermining is critical to stop a closure under tension. Relaxed Skin Tension traces directions for wound care, all agree that solar publicity should be minimized for six months to one yr after scar revision surgical procedure. Corticosteroids reduce blood vessel formation and reduce fibroblast proliferation and fibrosis in therapeutic wounds. Mature hypertrophic scars and small keloid scars could reply to a collection of corticosteroid injections given 4 to six weeks apart. Larger keloids should be excised, and corticosteroids injected both intraoperatively, or within the early postoperative period, in addition to each four to six weeks. Low dose exterior beam radiation has additionally been used for the remedy of recurrent keloids. Mechanical compression may be used to flatten some hypertrophic scars and keloids. Hyperpigmented scars can be treated with skin bleaching agents similar to hydroquinone 4%; however, they occasionally enhance with no treatment. Components of living tissue that absorb explicit wavelengths of laser gentle are known as chromophores. At this wavelength, the laser energy is best absorbed by the chromophore hemoglobin. This principle of selective photothermolysis permits for treatment of vascular lesions without harming the surrounding tissues.
Kakmachi (Bittersweet Nightshade). Rumalaya liniment.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96584
Tip projection refers to the extent of forward protrusion of the nose parallel to the Frankfort horizontal plane of the face muscle relaxant uk rumalaya liniment 60 ml purchase with visa. Patients could better perceive this concept because the extent of "Pinocchio" elongation exhibited by the nostril muscle relaxant chlorzoxazone side effects discount rumalaya liniment 60 ml online. As a common rule of thumb spasms shoulder generic 60 ml rumalaya liniment amex, tip projection ought to be roughly equal to the vertical height of the upper lip. Like its analog the nasofrontal angle, the nasolabial angle, also referred to as the columellalabial junction, is a vital parameter of profile aesthetics. The apex must also relaxation slightly posterior to the labial tubercle creating a mild backward slope to the higher lip. In patients with the caudal extra nasal deformity, the nasolabial apex is shifted each anteriorly and caudally, creating an obtuse or "webbed" nasolabial angle and foreshortening the higher lip. When nasal tip place shifts caudally alongside this arc of rotation, the tip turns into counterrotated or ptotic. From the front view, the nostril openings become less visible or could additionally be hidden totally, and the space from the sellion to the tip defining points, often recognized as the dorsal line, increases in length. In basic, a long dorsal line and ptotic nasal tip are associated with an aged appearance as nasal elongation is a common manifestation of human growing older. In contrast, when nasal tip position shifts cephalically alongside the identical arc of rotation, the dorsal line is shortened and nostril show is increased from the front. In ladies, a larger degree of tip rotation equates to a extra obtuse nasolabial angle of approximately ninety five to 110�, whereas in males an extended dorsal line with an acute nasolabial angle of 90� to 100� is typical. Although tip rotation could be gauged by nasolabial angle size, like tip projection, this method of assessment could show unreliable in the presence of columellar retraction or nasolabial protrusion (webbing) as often happens within the caudal excess nasal deformity. Another facet of profile aesthetics involving the nasal base is the columella alar relationship. In women, and to a lesser diploma in males, the columella has a mild downward curvature, the so-called double break, created by divergence of the underlying medial crura. In the cosmetically appealing nose, the alar rim possesses a reciprocal curvature resulting in 2 to 5 mm of columellar reveal, also called columellar show. Both congenital anomalies and purchased deformities could account for disturbances in the columellar alar relationship. Over-resection of the nasal dorsum typically exacerbates width discrepancies and is often related to formation of the inverted-V deformity. Frontal View and Lower Vault the nasal tip, or lobule, is among the most important cosmetic options of the nostril. From the entrance, the lobule must be easily distinguished from the adjacent nostrils, separated by faint shadows that blend smoothly into the adjacent alar crease. The ideal lobular width varies considerably based on a number of aesthetic factors including personal desire, nostril measurement, and dorsal width; however as a rule, the lobule should be about 10 to 20% wider than the aesthetically pleasing nasal dorsum. Overly broad nasal domes, extreme convexity of the lateral crura, or absence of domal divergence, end in broad, bulbous, or "uni" tip deformities, respectively. Excessive grooving between the alar domes, a condition often known as bifidity, is widespread in sufferers with skinny pores and skin and powerful, round alar cartilage. A modest degree of bifidity inside the infratip lobule is cosmetically desirable, however conspicuous bifidity within the lobule itself is mostly thought-about cosmetically undesirable. In most sufferers, the outer-alar margin should fall inside a few millimeters of the medial-canthal line, equating nasal base width to the intercanthal distance. Although surgical narrowing of the nasal base is occasionally fascinating, care have to be taken to avoid nostril deformity by confining nasal skin excision to the nasal sill. Sagittally oriented fusiform excisions of the nasal sill successfully narrow the nasal base with out distorting nostril shape. In distinction, pores and skin excision from the lateral ala as with the so-called "Weir incision," usually results in unsightly blunting of the nostril/cheek interface and ought to be prevented in most circumstances. Moreover, as a result of excessive tip width is often mistakenly confused with excessive alar width, alar base reductions are often performed unnecessarily. Although refinement of the oversized lobule is a frequent objective of cosmetic rhinoplasty, over-resection of the lateral crura in an ill-conceived try to slender the lobule will incessantly lead to stigmatic deformity of the nasal tip. In addition to pinching of the diamond-shaped lobule, cephalic malposition of the lateral crus usually ends in a conspicuous notching of the nostril rim resulting in undesirable distortion of the perfect "gull wing" configuration. In common, these tip deformities are greatest prevented by limiting excision of alar cartilage and preserving sufficient crural energy. Base View Examining the nose from the base view can significantly augment the nasal evaluation and reveal problems not all the time seen on the frontal or profile views. Assuming that the nasal base width is approximately equal to intercanthal width, the triangular-base configuration will provide a cosmetically acceptable tip configuration and insures a cosmetically pleasing diploma of tip projection. However, as with all aesthetic guidelines, allowances must be made for morphologic variants such as the affected person with extremely wideset eyes or extraordinarily narrow-set eyes. In both instances, the ideal nasal base width may not coincide with the existing intercanthal distance, and the nasal width must be calibrated to the general facial bone structure for optimal-cosmetic results. Other necessary features of the nasal base evaluation embrace the width and alignment of the columella, the columella to lobule ratio, and the form of the alar sidewall. Ideally, the columella lies within the midline and widens gently at its base as a end result of the flared footpods of the medial crura. Thus, lateral osteotomy bone cuts sometimes lie within the maxilla and only briefly traverse the nasal bone at its cephalic extent. During osteotomy of the nasofacial groove, dense bone of the anterior maxillary buttress positioned immediately lateral to the nasofacial groove, serves to help protect the adjoining lacrimal fossa from inadvertent damage. Beyond the rhinion, the nasal bones give rise to the cartilaginous nasal dorsum, also called the center nasal vault. The resulting osseocartilaginous pyramid is a structurally uniform and anatomically contiguous vault, which constitutes the whole nasal dorsum. Nasal deformities affecting the keystone area are notably challenging because of the increased potential for skeletal instability. The nasal valve is the narrowest segment of the human airway and it plays a significant function in creating enough airway resistance to facilitate filtration, warming, and humidification of the inspired air. Distally the nasal bones are thin and delicate, whereas their dense cephalic union with the nasal strategy of the frontal bone is seldom vulnerable to injury. Collectively, the nasal bones and the adjoining processes of the maxillae comprise the bony (or upper) nasal vault. The nasal bones are supported in the midline, from beneath, by the perpendicular plate of the ethmoid bone; and so they usually comprise roughly one-third to one-half of the nasal dorsum. The union of the nasal bone with the maxilla lies medial to the nasofacial groove, which is shaped by the anatomic junction of the nasal sidewall with the adjoining cheek. Note typical placement of lateralosteotomy reduce (blue line) for infracture of the nasal sidewall. Because anatomic reductions in nasal valve cross sectional area are related to an exponential enhance in nasal airway resistance, reductions in valve width as little as 1 mm can produce signs of nasal airway obstruction. These paired, mirror picture cartilages are intently approximated inside their medial (columellar) segment, but fold sharply at the nasal tip diverging in nearly reverse directions to span the decrease nasal sidewall. Although the nomenclature varies slightly amongst totally different authors, the designations lateral and medial crura are used commonly all through the medical literature. Moreover, certain descriptive phrases are used consistently throughout all classification systems and these include the nasal domes and the columellar foot pods. Clinically, the nasal domes correspond to the purpose of maximum tip projection, and their form and spacing govern the general contour of the nasal tip or lobule. The lateral crura comprise the "alar wings," which prolong superolaterally, connecting the nasal domes medially to the pyriform apertures laterally, simply above the alar creases. The power and rigidity of the lateral crura are integral to the help and functional integrity of the nasal sidewalls; and anatomic deformities, accidents, or improper surgical alterations can profoundly impair nasal respiration. Aesthetically, the lateral crura are likely to be most pleasing when flat, and in large unsightly noses Alar domes (tip defining points) they usually possess pure convex or concave curvatures in both their long and/or their short axes. Analogous to an automotive roll bar, the nasal scroll resists inward collapse from trans mural stress generated by mild (resting) inspiration. Since the nasal scroll defines the anatomic outer border of the nasal valve area and because the scroll supports the only mobile section of the valve perimeter, it also governs the brink for dynamic nasal valve collapse during extra vigorous inspiration. If the nasal scroll is damaged, corresponding to may occur with aggressive "cephalic resections" typical of conventional discount rhinoplasty, the remaining cartilage may be too weak to support the nasal sidewall. External manifestations of static nasal valve dysfunction embrace lobular pinching, alar retraction, and dimpling of the alar crease.
The general status of the hypopharynx with respect to the quantity of retained secretions muscle relaxant clonazepam buy 60 ml rumalaya liniment overnight delivery, tongue posi tion spasms jaw 60 ml rumalaya liniment cheap with amex, and sensation can additionally be ascertained muscle relaxant methocarbamol addiction discount 60 ml rumalaya liniment amex. Clinical Observation Observation of a feeding session by skilled multidisciplinary team members supplies perception into the underlying feeding downside. These observations focus on behavior problems, allowing for future structuring of behavioral interventions. If lip closure is poor, food mate rials may spill out of the mouth throughout feeding. In the presence of decreased orofacial tone, food materials could are inclined to acquire in the anterior or lateral sulci. Improper tongue management might pro pel food materials out of the mouth quite than posteriorly for swallowing. A child with a weak suck or poor coordination of the sucking process tends to current with multiple sucks per swallow to compensate for the shortage of efficiency. Nasopharyngeal regurgitation may occur with poor timing of velopharyngeal closure in the course of the swallow, or may be attributable to muscular weakness or paralysis preventing sufficient closure. The bolus stays underneath strain, and may be expelled into the nasopharynx when the velum descends. Attention to the position and posture of the kid and the mechanics of feeding skills during the ingestion of varied textures also supplies clues regarding underlying structural or physio logic issues. Underlying neurologic or struc tural issues could additionally be identified by observing behaviors similar to the flexibility to deal with oral secre tions, the pace of feeding, escape of food from the mouth, tongue and jaw actions, variety of swallows to clear a bolus, noisy airway sounds after swallowing, coordination of suck and swal low, laryngeal elevation, gagging, coughing, or emesis related to feedings. Attention to articulation and voice quality also may present useful information in that the identical constructions used for the oropharyngeal phases of feeding are used for voice and speech production. Abnormalities in bolus formation, timing of the swallow, or nasopharyngeal reflux can be visualized. Assessment of compensatory strategies such as positioning alterations, oralmotor methods, or alternation of food and liquid consistencies adds to the general exposure time. Esophagram and Upper Gastrointestinal Study the esophagram and higher gastrointestinal examine look at the structure and function of the esoph agus, abdomen, and duodenum. Dynamic photographs are obtained because the bolus passes via the oropharynx, into the esophagus, and into the stomach. Careful assessment of a attainable tra cheoesophageal fistula requires an sufficient volume of distinction to distend the esophagus. Abnormalities such as esophageal stric tures, webs, vascular rings, or achalasia could additionally be identified. Chest Radiographs Chronic aspiration results in adjustments within the lung parenchyma that could be seen on plain chest radi ographs. Typical findings embody hyperinflation, segmental infiltrates, peribronchial thickening, and bronchiectasis. Aspiration events affect the basilar and superior segments of the decrease lobes and the posterior upperlobe segments. Findings generally associated with continual aspiration, although not specific to it, embody bronchiectasis, centrilobular opacities, air trapping, and bronchial thickening. Indications of chronic change may not mirror current aspiration problems, but somewhat, could replicate previous aspiration occasions. The swal lowing evaluation is carried out with liquids (thin and with varying levels of thickness) as properly as a selection of pureed, clean, and strong textures as developmentally acceptable. To aid with visuali zation, the liquid and meals gadgets are combined with green food coloring by the speech pathologist before the study. A parent or caretaker typically is given the opportunity to bottle feed infants during the research. Based on the findings in the course of the research, modifications are launched by the speech pathologist. Interpretation of the examination requires an intensive understanding of the clinical condi tions and initial feeding evaluation of the patient. Pooling of secretions occ urs when secretions produced within the oral cavity spill over the tongue base into the hypopharynx and accumulate because of the absence of an enough swallowing response. Excessive pooling and poor management of secretions are instantly apparent when the hypopharynx is considered endoscopically. Premature spillage is the es cape of fabric over the tongue base in the absence of purposeful oral transfer earlier than the initiation of swallowing. The degree of spillage needs to be evaluated with respect to the ability of the patient to initiate a clearing swallow. Premature spillage of a volume sufficient to begin filling the pyriform sinuses is of concern, as it might increase the danger of aspiration. Laryngeal penetration is the passage of food materials or secretions into the endolarynx. If meals materials swimming pools within the hypopharynx, it may rise to a level at which the natural barriers defending the endolarynx are breached. The significance of laryngeal penetration depends on the volume of fabric getting into the larynx and the frequency of penetration occasions. Thin supplies have a larger probability of flowing through the glottis than do thick materials. Frequent laryngeal penetration occasions of significant quantity have the identical clini cal implication as frank aspiration. Aspiration that happens in the course of the whit eout period could be deduced by visualizing the occasions that happen instantly after the swallow, when materials is expelled from the airway by a cough or by identification of stained subglottic constructions. Residue refers to the food material re maining in the hypopharynx after completion of the swallow. The amount of residue persisting after the swallow relates on to the danger of aspiration and the overall security of swallowing a given meals consistency. Dye Studies In a affected person with a tracheostomy tube, signs of an aspiration occasion may be instantly noticed. The ingestion of intensely coloured meals material usually stains tracheal secretions when the material is aspirated. Suctioning tracheal secretions throughout or after a meal might reveal traces of the coloured material, indicating that an aspiration event has occurred; nevertheless, figuring out whether or not the occasion is secondary to reflux or related to an air way drawback during the swallowing course of could be difficult. In sufferers with a feeding tube, dye could be positioned instantly into the abdomen, thereby clarifying the character of the aspiration. Nuclear Medicine Scans Nuclear drugs scans could additionally be used in the assess ment of gastric emptying and gastroesophageal reflux. Technetium scans are helpful in the analysis of youngsters with gastric motil ity problems. Frequent pictures are then obtained by a gamma camera for one hour; delayed images are obtained for as a lot as 24 hours. Reflux occasions may be demonstrated by identifying labeled material within the esophagus. The reflux event might deposit gastric contents into the hypopharynx, the place it can be cleared by way of regular pharyngeal contractions or aspirated. The functioning salivary gland tissues will con centrate the label, which is then excreted into the mouth with saliva. In regular studies, the label is found in the salivary glands and abdomen, with low ranges within the oral cavity, pharynx, and esophagus. In children who aspirate oral secretions, labeled secretions are also seen throughout the lung fields. A thallium scan is helpful in figuring out the need for surgical intervention to stop chronic, lifethreatening pulmonary disease. In the setting of advanced medical and developmen tal situations, selections are finest made by way of a multidisciplinary staff method. The treating clinician should have a clear understanding of the interplay between anatomic abnormalities, med ical situations, the extent of functioning, and behavioral components. Children with psychosocial or behavioral issues related to their dysphagia are gener ally responsive to behavior therapy. A structured therapeutic program contains techniques such as rewarding successive approximations of targeted behaviors and providing optimistic reinforcement by way of praise, entry to favourite toys or music, clapping, or any similar ageappropriate reward. Behavior remedy can also be used to overcome con ditioned meals refusal (ie, a realized aversion to feeding) associated with a previous anatomic abnormality that has been corrected. For many kids with neural or anatomic abnormalities, secure oral feeding is extremely dif ficult or inconceivable. Deciding whether to pursue efforts at oral feeding requires consideration of the potential risks of aspiration and continual lung illness versus the comfort and emotional rewards of oral feeding. Drooling that persists beyond age 4 is taken into account abnor mal and may stem from a wide range of issues, including impaired oromotor management, inefficient swallow, decreased frequency of swallow, devel opmental delay, malocclusion, or a structural or postural drawback.
In contrast muscle relaxant long term use rumalaya liniment 60 ml generic visa, the topography of the nostril is convex within the space of the tip and dorsum spasms knee rumalaya liniment 60 ml without a prescription. A needle with an hooked up suture is passed full-thickness via the nose at the level marked in the alar groove muscle relaxant bath rumalaya liniment 60 ml purchase with visa. The suture is draped from the purpose across the defect, and a clamp is applied to the suture on the heart of the defect. The clamp with attached suture is then rotated about its pivotal point to point out the primary arc, which is marked with a pen. The donor web site for the second lobe is closed first by major approximation of the muscle layer. The first lobe is then transposed to the nasal defect and secured with a few deep dermal sutures. The second lobe is transposed, trimmed of its extra height so that it suits snugly without redundancy in the donor defect of the primary lobe. The height of the primary lobe extends to the second arc so its height is equal to the distance between the 2 arcs. The first lobe has the configuration of the defect, and the second lobe is triangular. The linear axis passing through the center of each lobe is positioned at approximately 45� from each other, with the axis of the primary lobe positioned 45� from the central axis of the defect. This orientation of the lobes inevitably positions the axis of the second lobe along the center of the nasal sidewall or diagonally on the junction of the sidewall with the dorsum. The design also creates a triangular peninsula of pores and skin between each lobe with a 45� angle. The base of the triangle is the lateral border of the defect, and the height of the triangle is equal to the radius of the defect. The flap and the remaining skin of the the ala is greatest resurfaced with cheek skin from the world of the melolabial fold. Menick has famous that as melolabial flaps contract, they turn out to be rounded resembling the contour of the conventional ala. Skin of the melolabial fold is transferred to the ala as an interpolated flap, the pedicle of which crosses over however not by way of the alar-facial sulcus. Although three weeks is a lengthy interval for the patient to endure the deformity caused by the flap, this interval allows the surgeon to defat aggressively and sculpture the flap both on the time of the flap transfer and on the time of pedicle detachment and flap inset. When reconstructing the ala, the entire ala is resurfaced with the cheek flap, except for 1 mm of alar pores and skin just anterior to the alar facial sulcus. This small pores and skin tag preserves the alar-facial sulcus and infrequently offers a better scar than when the flap extends to the sulcus. Maintaining the excision outdoors of the alar-facial sulcus lessens the risk of growing a depressed scar. This strategy additionally avoids the technically difficult necessities of integrating the flap into the nasal sill at the time of flap inset. When using cheek flaps for repair, I typically delay excising the extreme-lateral portions of the residual-alar pores and skin until the time of pedicle detachment and flap inset. Standing-cutaneous deformity marked laterally so scar from excision of deformity will lie in alar groove. The template is positioned so that the medial border of the designed flap lies in the melolabial crease. This arrangement insures that the flap is harvested from the cheek, not from the lip, and that the donor website wound closure will lie within the melolabial crease, offering maximum-scar camouflage. The flap is designed to pivot 90� towards the midline in a clockwise path when harvested from the left cheek and counterclockwise when harvested from the best cheek. As the flap is pivoted and transferred to the recipient web site, the medial border of the in situ flap is sutured to the cephalic border of the nasal defect. This in turn causes the inferior border of the in situ flap to join the anterior border of the defect. The lateral border of the in situ flap becomes the inferior border of the reconstructed ala. A triangle of pores and skin is marked superior and inferior to the tracing to trend a crescent island of pores and skin. The inferior triangle of pores and skin is excised and discarded at the time of flap transfer, and the superior triangle of pores and skin is transferred with the flap and is excised and discarded at the time of pedicle detachment and inset of the flap. The superior triangle of skin is minimized to scale back lack of tissue from the superior-melolabial fold the place the fold is well developed. Removing skin from the superior portion of the fold may result in appreciable asymmetry of the medial features of the cheeks. The flap is incised, and the distal portion is elevated in the subcutaneous aircraft. The distal third of the flap is skinny, leaving 1 to 2 mm of subcutaneous fats attached to the undersurface. Superiorly based mostly subcutaneous tissue pedicle interpolated cheek flap designed to cover cartilage graft. Caudal border of cheek flap sutured to caudal border of bipedicle-advancement flap. Depending on the shape of the flap, the lateral border of the donor website could additionally be considerably longer than the medial border. For subcutaneous tissue pedicled flaps, the pedicle is transected at the base, and the cheek pores and skin is undermined for a distance of two cm across the periphery of the amputated pedicle. After freshening the skin margins with a scalpel, the wound is closed by advancing the borders together. The lateral portion of the flap hooked up to the nostril is launched from attachments to the adjacent nasal skin for a distance of 0. Release permits the surgeon to take away excessive-subcutaneous fats not trimmed at the time of flap switch. When the alar base is absent, the flap is tailored to exchange the missing base and is integrated with the nasal sill. When the sill requires reconstruction, the flap is trimmed in order that it has a tapered finish which will function the sill. The pedicle of fat is free of the surrounding-cheek fat by incising via borders of the pedicle perpendicular to the surface of the skin. The depth of the incision is carried to the extent of the superficial floor of the zygomatic main and levator labii muscles. On reaching the zygomatic main muscle, blunt dissection continues upward on the floor of the muscle, releasing the attachments of the pedicle to deeper constructions till the flap can attain the recipient site with out undue tension. The subcutaneous pedicle is excised, the pores and skin edges surrounding the pedicle are freshened and the wound closed primarily. However, harvesting the island flap is technically harder than harvesting a cutaneous-pedicle flap because the plane of dissection is considerably deeper, inserting the branches of the facial nerve supplying the zygomatic main and minor muscular tissues at higher risk of injury. A cutaneous pedicle interpolated melolabial flap is a peninsular flap with a linear axis centered on a cutaneous pedicle that connects the flap to the cheek. Whether a peninsular or island flap, the pedicle is developed at the superior side of the melolabial fold. The peninsular flap is determined by the dermal and subdermal vascular plexus of the cutaneous pedicle to provide vascularity to the distal flap. The cutaneous pedicle will need to have enough width and depth to insure this vascularity. When designing a peninsular flap, the orientation of the template stays the same as for designing an island flap. The peninsular flap is elevated in a subcutaneous-tissue plane, maintaining three mm of fats on the undersurface of the cutaneous pedicle. This is in contrast to the island design, based mostly on a subcutaneous-tissue pedicle that might be as a lot as 1. Thus, the airplane of dissection for the cutaneous-pedicle flap is considerably more superficial. Like the island flap, the peninsular flap pivots 90� toward the midline and is sutured to the nostril similarly. Like the island flap, the distal half of the peninsular flap could additionally be thinned as necessary to replicate the thickness of the recipient web site.






