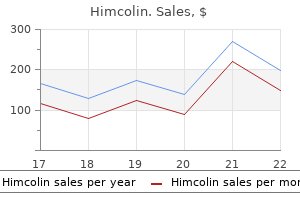
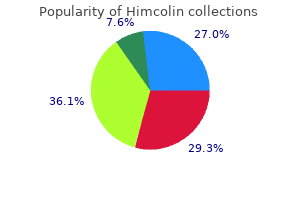
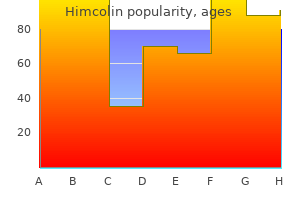
Himcolin
Himcolin
Himcolin dosages: 30 gm
Himcolin packs: 1 tubes, 2 tubes

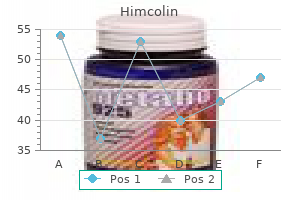
Similarly impotence gel himcolin 30 gm buy otc, bacterial infections of the chest proceed to symbolize a lot of cases on a global scale impotence antonym himcolin 30 gm purchase amex, however these have largely disappeared in the United States following the introduction of antibiotics and improved drainage procedures erectile dysfunction jokes order 30 gm himcolin overnight delivery. Constrictive pericarditis is a late complication of radiation therapy, typically occurring many years after the administration of radiation. Risk elements for development of constrictive pericarditis include length of therapy, whole quantity of radiation administered, and quantity of the heart in the radiation subject. In contrast to other causes of constrictive pericarditis, where the myocardium is usually regular in structure and performance, there could also be associated radiation harm to the myocardium. Constrictive pericarditis is a well-documented late complication of cardiac surgery, including coronary artery bypass grafting and valvular surgical procedure. Risk components for improvement of postoperative constrictive pericarditis embody intraoperative hemorrhage into the pericardium, postoperative pericarditis, and the prevalence of postpericardiotomy syndrome. End-stage renal illness, neoplastic disease (primarily breast, lung, and lymphoma), and connective tissue illness are much less widespread causes that must be considered within the initial differential. However, in a small percentage of patients with constrictive pericarditis, the pericardium may not seem thickened on noninvasive imaging. This enhance in strain impacts each ventricles equally and successfully decreases diastolic filling and thus end-diastolic quantity of both ventricles. The increased strain is transmitted backward and leads to elevated pulmonary venous and systemic venous pressures. Equalization of end-diastolic pressures in all four cardiac chambers then ensues and is a vital attribute of constrictive pericarditis. The myocardium is generally normal in structure and performance; due to this fact, systole is unimpaired. Diastolic perform, on the opposite hand, is markedly altered by the constrictive course of. The early signs of constrictive pericarditis are often insidious, and the patient may have nonspecific complaints corresponding to malaise, fatigue, and decreased exercise tolerance. As the illness progresses, signs according to systemic congestion and low cardiac output, such as marked jugular venous distention, ascites, peripheral edema, and worsening exercise tolerance, may predominate. Symptoms because of right-sided failure often predominate over left-sided failure because of equalization of pressures. Nearly all patients have jugular venous distention, which merely reflects the elevated right-sided pressures. Appreciation of the peak of the pressure might solely be evident on inspecting the affected person upright. Cardiac auscultation may reveal muffled heart sounds because of decreased transmission by way of the thickened pericardium. Because the mitral and tricuspid valves are nearly closed by the top of diastole, there may be a delicate first coronary heart sound (S1). Occasionally, one may hear a pericardial knock in early diastole (60 to 120 milliseconds after the second heart sound [S2]). This represents the abrupt cessation of diastolic filling that happens when further ventricular rest is impeded by the rigid pericardium. An opening snap may be related in frequency and timing but is almost always followed by a diastolic rumble. Auscultation of the lung fields may reveal decreased breath sounds at the bases, attributed to pleural effusions. The belly examination might reveal evidence of right-sided coronary heart failure, with hepatomegaly and splenomegaly being frequently famous. Confirming the prognosis of constrictive pericarditis often presents a problem, since no gold commonplace check exists. The clinician should depend on a set of findings from a quantity of diagnostic modalities to detect each anatomic and pathophysiologic abnormalities. The calcification is normally finest appreciated with a lateral movie and regularly entails the proper ventricle and atrioventricular groove. Pleural effusions happen incessantly, and there could additionally be proof of each left and right atrial enlargement. This is the sudden cessation of septal movement, as the center abruptly stops filling upon meeting the rigid pericardium. Although imaging findings could suggest pericardial constriction, most of the findings described beforehand are relatively low in sensitivity and specificity. Doppler assessment of diastolic flow patterns and the respiratory adjustments in these patterns may present vital proof for the presence of constrictive physiology and help in helping exclude competing diagnoses, similar to restrictive cardiomyopathy. In constrictive pericarditis, the thickened pericardium isolates the cardiac chambers from respiratory modifications in intrathoracic pressures. This reduces the pressure gradient required for diastolic filling of the left ventricle; subsequently, a lower in mitral circulate is observed throughout inspiration. Findings suggestive of constrictive physiology embrace the next: (a) Mitral valve inflow. Peak E velocity will increase by 44% or larger and peak A velocity increases by 38% or greater. The wide respiratory variation in peak E velocities helps to differentiate constrictive pericarditis from restrictive cardiomyopathy, in which minimal respiratory variation occurs. In a healthy particular person, pulmonary venous flow consists of a peak velocity during ventricular systole (S wave) and a smaller peak velocity during ventricular diastole (D wave). In constrictive pericarditis, there is a rise in early diastolic flow manifested as a bigger D wave; due to this fact, the pulmonary systolic/diastolic (S/D) circulate ratio is decreased. The peak early diastolic filling velocity is denoted as E and the height late diastolic filling velocity (from atrial contraction) is denoted as A. In constrictive pericarditis, inspiration results in increased peak E and peak A velocities across the tricuspid valve. The peak pulmonary venous velocities during systole are denoted because the S wave and peak diastolic velocities are denoted as the D wave. This enhance in expiratory pulmonary venous circulate assists in distinguishing constrictive pericarditis from restrictive cardiomyopathy. Hepatic venous move displays rightsided filling in much the same method that pulmonary venous move displays leftsided filling. Individuals with constrictive pericarditis and people with out have a extra prominent systolic flow than a diastolic circulate; nonetheless, people with out constrictive pericarditis have little respiratory variation in these move velocities. Doppler tissue imaging (a) Myocardial rest, and thus annular velocity, is usually reduced in restrictive cardiomyopathies, but the Doppler velocities of the medial mitral valve annulus in early diastole are normal or slightly increased in constrictive pericarditis. In regular individuals, peak early diastolic annular tissue velocity (E) on the lateral mitral annulus is larger than that at the medial mitral annulus. This relationship between the lateral and medial mitral annuli is reversed ("annulus reversus") in constriction, the place E on the lateral mitral annulus is usually lower than E at the medial mitral annulus. Similar to pulmonary vein move, the S wave represents peak systolic flow velocity and the D wave represents peak diastolic flow velocity. In both normal subjects and those with constrictive pericarditis, there is an increase in both S and D waves with inspiration. Differentiation of constrictive pericarditis from restrictive cardiomyopathy by Doppler transesophageal echocardiographic measurements of respiratory variations in pulmonary venous flows. The hemodynamics obtained within the catheterization laboratory assists in both diagnosing constrictive pericarditis and differentiating it from restrictive cardiomyopathy. In basic, each proper and left coronary heart catheterization are carried out to obtain simultaneous ventricular pressure readings. Note that tissue velocities are lower in restrictive cardiomyopathy compared with constrictive pericarditis. In addition, lateral E is decrease than septal E in constrictive pericarditis, which is attributable to perimyocardial tethering of the lateral left ventricular free wall. The preserved x descent and the prominent y descent contribute to the traditional W-shaped atrial waveform. The proper atrial pressure waveform has been described as having a W-shaped configuration. This morphology is produced by a prominent a wave as the atria contract towards an elevated ventricular stress, an exaggerated x descent, and a steep y descent, due to fast ventricular filling in early diastole. Ventricular pressures (1) Ventricular pressure waveforms reveal the traditional dip-and-plateau physiology, generally referred to as the square root signal. Note the equalization of left ventricular and right ventricular end-diastolic pressures, usually within 5 mm Hg of every other. The fast early diastolic filling and subsequent abrupt cessation of move because of the rigid pericardium produces a dip-and-plateau waveform (square root sign), appreciated finest in this waveform following the premature ventricular contraction.
Calcium channel blockers are most well-liked in patients with variant angina or cocaine-induced vasospasm erectile dysfunction at age 21 safe 30 gm himcolin. Overall erectile dysfunction wife himcolin 30 gm purchase amex, patients selected to have early invasive therapy may have coronary angiography carried out within 24 hours of admission erectile dysfunction nclex questions purchase himcolin 30 gm on-line, or sooner, relying on the scientific situation. Those patients elected to a conservative technique are managed with optimal medical therapy and undergo angiography solely in choose circumstances similar to growth of recurrent signs or goal evidence of ischemia while on appropriate medical therapy. The choice of which strategy to make use of ought to be based upon both physician and affected person preference. Women with low-risk features are beneficial to proceed with a conservative technique. This is especially true when the dangers of revascularization are prone to outweigh the benefits. These results recommend that even in moderate-risk sufferers, an early invasive strategy may be most well-liked. In basic, the decision of which brokers to use depends on (1) whether or not an early invasive strategy is used and (2) what post-angiography management strategy is employed. The antiplatelet and anticoagulant therapies out there for each of the next strategies are listed beneath. The specific doses, adverse results, and pharmacokinetics of these agents are then listed separately. After receiving aspirin, patients who endure an preliminary conservative strategy ought to obtain an anticoagulant and be began on clopidogrel remedy. Before continuing with catheterization, it is recommended to administer a second antiplatelet agent. Once angiography is performed, the suitable subsequent therapy is dependent upon the administration plan. There are several pathways that result in platelet activation, of which aspirin blocks only the cyclooxygenasederived thromboxane A2 pathway. Those sufferers allergic or illiberal to aspirin should obtain clopidogrel as quickly as attainable. Subsequent day by day aspirin doses may be reduced, with the preferred dose for secondary prevention being 81 to 162 mg day by day; this should be continued indefinitely. Ticlopidine and the opposite thienopyridines inhibit adenosine diphosphate� induced platelet aggregation. Clopidogrel was the second commercially obtainable thienopyridine and is the most extensively studied member of this group. Patients handled with this mix skilled lower rates of refractory ischemia, heart failure, or revascularization. Rarely, it can cause an allergic reaction typically resulting in diffuse urticaria. This decrease in ischemic end points got here at the price of an increase in main bleeding. In preclinical research, prasugrel has been proven to have a more potent antiplatelet impact than clopidogrel. However, the salutary advantages in discount of ischemic occasions with prasugrel came at the expense of an increase in late bleeding occasions, together with a big increase in charges of each major bleeding (2. It is an absolute contraindication to use prasugrel in patients with a history of transient ischemic attack or stroke and a relative contraindication in sufferers seventy five years of age or < 60 kg due to the absence of a net favorable benefit or perhaps a harmful impact in these affected person subgroups. Like clopidogrel, prasugrel is a prodrug and is quickly metabolized to a pharmacologically active metabolite and inactive metabolites. After a 60-mg loading dose of prasugrel is given, 90% of sufferers obtain 50% inhibition of platelet aggregation inside 1 hour, with most achieved platelet inhibition being approximately 80%. The loading dose for prasugrel is 60 mg adopted by a upkeep dose of 10 mg/d. This got here at the value of a rise in nonprocedural bleeding in sufferers who had been randomized to ticagrelor. The loading dose of ticagrelor is one hundred eighty mg followed by a maintenance dose of 80 mg twice daily. Studies have shown that this rebound ischemia can be attenuated with the concomitant use of aspirin. Initially, heparin should be given as a weight-adjusted bolus (60 U/ kg), adopted with an infusion (15 U/kg/h). Patients handled with enoxaparin also underwent fewer revascularization procedures and experienced related charges of major bleeding. Bivalirudin is an artificial derivative of hirudin, with a shorter half-life, that reversibly inhibits thrombin. Fondaparinux is a heparin pentasaccharide analog that selectively inhibits issue Xa within the coagulation cascade. These properties translate into more predictable and sustained anticoagulation, which allows fixed-dose, oncedaily administration. Fondaparinux is renally cleared and its use is contraindicated in those sufferers with a creatinine clearance (CrCl) < 30 mL/min. Fondaparinux can be utilized for anticoagulant therapy in these sufferers chosen to bear a conservative medical approach. Eptifibatide is a cyclic peptide inhibitor derived from snake venom, with rapid onset and a brief half-life. Because of its short half-life, steady drug infusion is required to sustain maximal inhibition of platelet aggregation. Patients treated with abciximab additionally had a better fee of thrombus decision and improved procedural success. The composite finish point, however, was not considerably totally different at 30 days, although the mortality was reduced (3. In sufferers not more likely to be treated with an early invasive technique, abciximab has proven no profit using the dosing protocol described in that trial. However, this benefit was observed solely in these sufferers with elevated troponin levels. Several studies have proven that the profit of these agents resides primarily with patients presenting with elevated cardiac troponins. The lack of efficacy of fibrinolytic agents in these patients could end result from the prothrombotic milieu induced by publicity of clot-bound thrombin after fibrin cleavage. Plasmin generation will increase, and platelets are activated, perpetuating this prothrombotic state. If anginal signs recur after hospital discharge, stress testing or cardiac catheterization may be carried out, relying on the medical presentation. An train routine in secure sufferers, smoking cessation efforts, and dietary changes have all been shown to enhance outcomes. Hypertension, dyslipidemia, and diabetes mellitus must be diagnosed and aggressively treated. Specific recommendations regarding a secondary prevention postdischarge medicine regimen are listed under: A. All patients should be given clear directions about what symptoms to look for which are suggestive of worsening myocardial ischemia. In addition, all patients ought to be given sublingual or spray nitroglycerin and instructions on how to use it. In those individuals randomized to eplerenone as in contrast with placebo, there was a major reduction in overall mortality (14. There is an elevated threat of hyperkalemia with use of this agent, particularly in these sufferers with irregular renal perform. Further evaluation from this trial demonstrated an early scientific profit, which correlated with concomitant reductions in C-reactive protein levels, at 30 days with use of intensive lipidlowering therapy. These early advantages from statin therapy are likely caused by the "pleiotropic" or nonlipid-lowering effects of statins similar to their anti-inflammatory, antioxidant, and antithrombotic properties. Outcomes in sufferers with acute non-Q-wave myocardial infarction randomly assigned to an invasive as compared with a conservative administration technique. Angiographic stenosis development and coronary events in sufferers with "stabilized" unstable angina. Early invasive versus selectively invasive management for acute coronary syndromes. A validated prediction model for all forms of acute coronary syndrome: estimating the risk of 6-month postdischarge death in an international registry. Effects of tissue plasminogen activator and a comparability of early invasive and conservative strategies in unstable angina and non-Q-wave myocardial infarction. Emergency room triage of patients with acute chest pain by the use of fast testing for cardiac troponin T or troponin I.
While not a direct toxic chemical impact erectile dysfunction treatment dubai purchase himcolin 30 gm overnight delivery, hypoxia can be an important cause of fish and invertebrate mortality in aquatic techniques; anthropogenic inputs of nutrients related to sewage or fertilizers that improve the expansion of phytoplankton could cause or exacerbate hypoxia (Paerl et al young living oils erectile dysfunction discount himcolin 30 gm with mastercard. While direct mortality may not be a commonplace effect of poisonous chemical substances in pure methods impotence age 40 himcolin 30 gm proven, mortality contains a significant end level in toxicity testing, discussed later. Reproduction and Development Impacts on reproduction and growth comprise maybe the best concern amongst potential sublethal results of xenobiotics on animals inhabiting natural methods. This is due to sensitivities of the physiological processes involved which were described for a quantity of pollution, and the significance of reproduction and improvement to population dynamics, a key ecological concern. Concern for reproductive and developmental effects has blossomed lately, with the widespread detection of endocrine disruptors within the environment. A number of environmental contaminants have been related to reproductive and/or developmental results in wildlife populations, with this association supported by managed laboratory research. Other examples embrace effluents from bleached paper mills in numerous locations, together with Canada (Munkittrick et al. Notably, selenium produced severe developmental effects in water birds feeding in a created wetland in central California (Kesterson National Wildlife Refuge) that concentrated naturally occurring selenium (Ohlendorf, 2002). Laboratory investigations, largely with fish and bird fashions, have proven that embryo development could be very delicate to these compounds, and such results probably underlaid the population crashes (Fairbrother et al. Contaminant results on improvement are often difficult to discern in field research, because of the small size of embryos and the fact that developmental impacts usually both are lethal or tremendously lowered survival. However, youth stages of most organisms are generally extra sensitive to xenobiotics than other life stages; thus, developmental impacts merit cautious attention by ecotoxicologists. Of nice concern are interactions between disease organisms and environmental contaminants, notably potential impacts of chemicals on immune systems that render organisms extra prone to illness. The question is often raised about how chemical pollution elevates the role of illness in inhabitants viability and dynamics. Both area observational and laboratory experimental research inspire this concern. In a case�control examine utilizing long-term knowledge from research of marine mammal strandings in the United Kingdom, Hall et al. In a research of free-ranging logger-head sea turtles (Caretta caretta) collected in North Carolina, Keller et al. They concluded that chemical and nonchemical stressors contributed equally to disease-induced mortalities that had been predicted to range from 3% to 18% of the population, depending on residence time. Numerous laboratory studies have demonstrated chemical impacts on immune systems in animals of ecological relevance. The potential results of chemical substances on immune function and illness susceptibility in wildlife is clearly a vital topic in ecotoxicology and one more doubtless to see significant advances in the near future as highly effective genomic tools turn out to be more out there for representative species. Behavior the impacts of chemical compounds on animal behavior have acquired vital consideration amongst ecotoxicologists. Relatively subtle results on behaviors related to, for example, mating and replica, foraging, predator�prey interactions, preference/ avoidance of contaminated areas, and migration have doubtlessly important ramifications for inhabitants dynamics. In some cases, however, biochemical mechanisms underlying behavioral results have been elucidated that may assist with these issues and supply useful biomarkers for behavioral toxicants in subject research. As noted by Rand (1985), chemical compounds inflicting behavioral results in wildlife are often known from mammalian research to be neurotoxicants. The results of pollutants, including pesticides, on fish behavior were reviewed by Scott and Sloman (2004). Mercury, particularly as methylmercury, contains another potent neurotoxicant that has been proven to perturb habits in wildlife. In a research using fish captured within the field and introduced into the laboratory for behavioral evaluation, Smith and Weis (1997) observed that killifish captured from a mercury-polluted tidal creek in New Jersey exhibited decreased feeding activity and greater mortality as a outcome of predation than killifish from an uncontaminated site. Using mercury concentrations in feathers as a marker for exposure, Heath and Frederick (2005) observed a adverse correlation between mercury publicity and nesting activity amongst White Ibises (Eudocimus albus) in the Florida Everglades that may be associated to behavioral results. The results of mercury on wildlife, together with behavioral impacts, had been reviewed by Wolfe et al. Environmental contaminants not usually thought of as neurotoxicants have also been shown to perturb behavior. For example, cadmium and copper have been shown to impression olfactory neurons and associated behaviors (preference/avoidance to chemical compounds, including pheromones) in a quantity of fish species (Saucier et al. Copper publicity in zebrafish additionally led to lack of neurons in the peripheral mechanosensory system ("lateral line"), which could result in altered behaviors associated with education, predator avoidance, and rheotaxis (physical alignment of fish in a current) (Linbo et al. Clearly, numerous mechanisms of chemical toxicity can lead to behavioral impacts, together with direct toxicity to neurons, alterations in hormones that modulate behaviors, and impaired energy metabolism. In some cases, impaired behavior may comprise a sublethal impact with substantive ecological consequence (Scott and Sloman, 2004). As in humans, most cancers in these animals occurs largely in relatively older age classes and subsequently is oftentimes thought of a disease unlikely to instantly impression population dynamics or different ecological parameters. However, this may not always be the case, particularly in species that require many years to attain sexual maturity and/or have low reproductive rates. In any event, the occurrence of excessive incidences of cancer in wildlife populations raises severe concerns for environmental high quality at those places experiencing these epizootics. For these reasons, in addition to for considerations for human health in these areas, and some great advantages of various models similar to fish for understanding chemical carcinogenesis, these epizootics have motivated substantial research in a quantity of areas related to human health and ecotoxicology. In subject studies of most cancers outbreaks in aquatic and marine techniques, usually solely selected species exhibit elevated cancer charges related to chemical contamination. A major contributor to this differential cancer susceptibility in wild fish populations is clearly way of life; benthic (bottom-dwelling) species such as brown bullhead (Ameriurus nebulosus) and white sucker (Catostomus commersoni) in freshwater systems, and English sole (Parophrys vetulus) and winter flounder (P. Thus, benthic fish expertise larger exposures to carcinogens than other species in these techniques. In their evaluation of cancer epizootics in fish, Harshbarger and Clark (1990) concluded that cancers of the liver (hepatocellular neoplasms) had the strongest associations with chemical air pollution, though cancers have been noticed in other tissues in wild fish as nicely (Ostrander and Rotchell, 2005). This recognition of shared pathways has partly contributed to the use of various fish models for learning chemical carcinogenesis from a human well being as well as from a broader environmental standpoint. An necessary historical occasion was the identification in Italy, France, and the United States in the course of the Fifties and Sixties of aflatoxin as a potent liver carcinogen in farm-raised rainbow trout (Sinnhuber et al. Thus, the rainbow trout observations led to the discovery of a new and important class of chemical carcinogens, and the popularity that fish could be very delicate to chemical carcinogenesis. Since that point, different fish species have been employed for laboratory research related to chemical carcinogenesis, particularly medaka (O. Compared with rodent models, fish models have benefits of lowered costs for propagation and housing, briefer time intervals between exposures and the expression of tissue modifications indicative of carcinogenesis, and larger feasibility of performing large-scale studies with many animals to quantify dose�response relationships. It is noteworthy that the nice bulk of reviews of elevated cancer rates in free-living animals occur in fish, with few reviews of probably chemically related cancers to our information in other vertebrates. The authors noted that beluga was the only species of marine mammal amongst 20 inhabiting this technique that exhibited elevated most cancers rates, and that cancers are uncommon worldwide in marine mammals. It is likely that elevated exposures play an important role within the comparatively high frequency of reviews of cancers in benthic fishes; relative inherent sensitivities amongst mammals, birds, reptiles, amphibians, and fishes are unclear. Assessment of toxicant results on populations has been important in ecotoxicology since its inception (Newman, 2001). A well-known, early occasion is the sharp drop after which sluggish recovery of coastal populations of osprey (Spitzer et al. Another was the enhanced, genetically primarily based tolerance of pest insect populations chronically sprayed with pesticides (Mallet, 1989). Industrial melanism, the premier example in biology textbooks of pure choice in wild populations, is another example of population ecotoxicology (Newman, 2001). Population ecotoxicology covers a variety of subjects with core research themes being (1) epidemiology of chemical-related illness, (2) effects on general inhabitants qualities together with demographics and persistence, and (3) inhabitants genetics. The degree of perception warranted for attainable contaminant-related effects in nonhuman populations is assessed by making use of routine epidemiological strategies. Consistency of affiliation long-standing commitment to understanding chemical publicity effects on natural population viability. Protecting populations is an explicitly stated objective of a number of Congressional and Agency mandates and regulations. Inconsistent the impact, or elevated level of temporal sequence impact, occurs before publicity to the hypothesized cause 6. Rules of thumb for gauging the level of belief warranted by proof that emerged from human epidemiology are also utilized in population ecotoxicology. As an instance, Fox (1991) (Table 30-1) modified such rules of thumb to accommodate slight variations in the topic material and approaches in population ecotoxicology. Logistic regression models had been additionally used to establish relationships between these lesions and chemical and organic risk elements (Myers et al. These fluctuations are characteristic of the species technique for maintaining itself in varied kinds of habitats and toxicant exposure could potentially change this vary (Simkiss et al.
In many sufferers who develop coronary heart failure bpa causes erectile dysfunction order 30 gm himcolin with amex, fatigue and decreased train capacity are the initial manifestations erectile dysfunction over 65 30 gm himcolin cheap free shipping. The prognosis is normally presumptive impotence young men purchase himcolin 30 gm, based on patient demographics and the medical course. Acute rheumatic fever (usually impacts coronary heart in 50% to 90%): related indicators similar to erythema marginatum, polyarthralgia, chorea, and subcutaneous nodules. Hypersensitive or eosinophilic myocarditis: pruritic maculopapular rash and history of onset temporally related to initiation of potential offender medications four. Disease-specific testing is indicated if the next circumstances are suspected: 1. Pericarditis can accompany myocarditis and is often manifested in pericarditislike changes seen in electrocardiography. In some instances, fascicular block or atrioventricular conduction disturbances and ventricular tachyarrhythmia may be hemodynamically vital. In a series of 23 patients with biopsy-proven myocarditis, significant reduction in proper ventricular perform was a robust predictor of dying or the need for cardiac transplantation. Gallium scanning identifies extreme myocardial cellular infiltration with excessive specificity (98%) but low sensitivity (36%). Cardiac angiography is commonly indicated to rule out coronary artery disease as the trigger of new-onset coronary heart failure, because the scientific presentation of myocarditis could mimic myocardial infarction. Cardiotropic viruses similar to enteroviruses (specifically the coxsackie group B and echoviruses) might cause direct cardiotoxic accidents, cytokine activation, cytoskeletal injury, and autoimmune responses. Cardiac involvement often appears decades after initial therapy and is the main cause of dying of persons aged 30 to 50 years in the endemic areas. Occasionally hepatosplenomegaly and lymphadenopathy happen, however concomitant meningoencephalitis is uncommon. Approximately 5% to 10% of affected sufferers may develop direct acute-to-chronic development. The hallmark characteristic is the presence of fused, multinucleated (> 20 nuclei) epithelioid big cells of histocytic origin within a diffuse, intramyocardial inflammatory infiltrate with lymphocytes. Consideration for early cardiac transplantation is acceptable (71% 5-year survival after successful transplantation). Often, mechanical support may be required as a short lived bridge to restoration or transplantation. Although observational sequence suggest potential scientific advantages of corticosteroid therapy, the most effective strategy is to take away the causative agent when known. Other causes include parasitic infection, drug hypersensitivity, and cellular rejection after cardiac transplantation, in addition to postvaccinia myocarditis after small pox vaccination. However, small retrospective surveys and case series have identified a big decrease in mortality and improved clinical course amongst cardiac sarcoid patients treated with corticosteroids and other immunosuppression strategies. On the premise of inhabitants studies, adults with myocarditis might present with few symptoms or with an acute poisonous state of cardiogenic shock or frank coronary heart failure. However, adults may present with coronary heart failure years after the preliminary index occasion of myocarditis (up to 12. The outlook is poor within the acute section, regardless of clinicopathologic classification, but these surviving the acute part have a extra favorable prognosis (except for these with chronic energetic myocarditis). Many patients could have full spontaneous medical restoration, even after weeks of mechanical help. In the Myocarditis Treatment Trial, the 1-year mortality price was 20% and the 4-year mortality rate was 56%. Standard coronary heart failure remedy consists of diuretics, angiotensin-converting enzyme inhibitors, -blockers, and aldosterone antagonists. Because of its proarrhythmic properties in animal models, digoxin must be avoided. Anticoagulation to forestall thromboembolic events is normally really helpful in patients with apical aneurysm with thrombus. Inotropic remedy is reserved for severe hemodynamic compromise, notably in fulminant myocarditis. Aggressive help with mechanical and surgical intervention is often indicated (see Chapters 8 and 12). Intra-aortic balloon counterpulsation for hemodynamic assist and afterload discount b. There is a theoretical elevated risk of myocardial inflammation and necrosis, cardiac reworking, and demise, as shown in animal fashions. Antiarrhythmics provide the first-line therapy using standard therapy such as -blockers, amiodarone, and sotalol. Clinical follow-up ought to be close as a end result of persistent continual inflammation could lead to dilated cardiomyopathy. More work is required to identify patient cohorts who will profit from tailor-made antiviral and immunosuppressive therapy. Incidence of biopsy-proven myocarditis in recent-onset, unexplained heart failure could be as little as 8% to 10%. False-negative rates are excessive (50% even in four or 5 biopsies) because of the small number of lymphocytes and difficulties in distinguishing cell types, with extensive interobserver variability. Rapidly progressive coronary heart failure signs despite typical therapy or new-onset frequent ventricular tachyarrhythmia or conduction disturbances b. Amount of cells: none (grade 0), gentle (grade 1), reasonable (grade 2), and severe (grade 3). Considerations are reserved for sufferers with new-onset, quickly deteriorating, superior heart failure with suspicion of the next situations: a. Oral cyclosporine: 5 mg/kg bid to achieve stage of 200�300 ng/mL � 1 wk; adjust oral dose to achieve degree of 100�200 ng/mL from weeks 2 to 4; regulate oral dose to achieve level of 60�150 ng/mL from weeks 4 to 24. Immunosuppressive therapy for active lymphocytic myocarditisd Prednisone 1 mg/kg/d for four wk; decreased to 0. Controlled trial of intravenous immune globulin in recent-onset dilated cardiomyopathy. Of those that failed conventional remedy, those sufferers who responded to immunosuppression had been significantly more more doubtless to have positive cardiac antibodies (90% vs. National Institutes of Health-sponsored workshop on inflammation and immunity in dilated cardiomyopathy. The role of endomyocardial biopsy within the administration of heart problems: a scientific assertion from the American Heart Association, the American College of Cardiology, and the European Society of Cardiology endorsed by the Heart Failure Society of America and the Heart Failure Association of the European Society of Cardiology. Immunosuppressive therapy for active lymphocytic myocarditis: virological and immunosuppressive profile of responders versus nonresponders. Current position of endomyocardial biopsy in the administration of dilated cardiomyopathy and myocarditis. Long-term consequence of fulminant myocarditis as in contrast with acute (non-fulminant) myocarditis. A potential, randomized, managed trial of prednisone for dilated cardiomyopathy. Cauthen Gonzalo Gonzalez-Stawinski Mazen Hanna Nontransplantation Surgical Treatment for Chronic Heart Failure I. Fortunately, there are multiple potential surgical interventions available for these patients which will assist to avoid or postpone the need for superior salvage therapies and transplantation. Despite the advance in surgical techniques and an enhanced understanding of the role of reconstructing structural abnormalities of the failing coronary heart, security and efficacy information are nonetheless restricted for lots of of those procedures. Surgical approaches to the administration of coronary heart failure should be accompanied by continued aggressive pharmacologic therapy. Loss of coronary flow reserve in extreme coronary artery disease results in reduction in myocardial perfusion, tissue hypoxia, and myocardial dysfunction. Myocardial infarction results in necrosis, scarring, and loss of contractile operate. Sites distal to infarction bear elevated mechanical stress and adverse remodeling over time. Progressive ventricular dilation and impairment of systolic and diastolic operate occur.
Obstructive sleep apnea and central sleep apnea are common comorbidities contributing adversely to the pathogenesis and prognosis of patients with heart failure erectile dysfunction quiz buy himcolin 30 gm fast delivery. The effective management of heart failure relies on appreciating the distinction between acute and persistent therapies erectile dysfunction options himcolin 30 gm best. The preliminary management goals include symptom improvement erectile dysfunction causes alcohol himcolin 30 gm otc, decongestion, and hemodynamic stabilization with optimization of tissue perfusion. It is necessary to attempt to determine and correct any precipitating factors (Table 8. Continuous blood strain monitoring with an arterial catheter may be helpful in circumstances with marginal blood strain and permits for optimum titration of intravenous vasodilators. In the absence of symptomatic hypotension, intravenous vasodilators are the first-line remedy for the management of cardiogenic pulmonary edema. Sodium nitroprusside is a potent vasodilator with balanced venous and arteriolar results. Nitroprusside is particularly useful in situations the place a fast and large discount in afterload is desired. While cyanide and thiocyanate toxicity is exceedingly rare with quick durations of remedy, nitroprusside should be used with warning in sufferers with extreme renal dysfunction. In sufferers with myocardial ischemia, nitroglycerin or a mixture of nitroglycerine and nitroprusside is most popular to avoid the theoretical risk of coronary steal. Nesiritide is an intravenous vasodilator that gained popularity in the acute care setting because of its ease of use in the absence of invasive hemodynamic monitoring. Typical dosing begins with 2 mg/kg delivered by intravenous bolus adopted by an infusion at a rate of zero. While providing some reassurance regarding previous security issues, these results have led most consultants to discourage its use on the premise of lack of efficacy. In addition to their ability to progressively cut back intravascular volume, diuretics have an instantaneous vasodilatory effect, which can be responsible for their immediate symptom relief. Patients without persistent exposure to loop diuretics often reply to 20 to 40 mg of intravenous furosemide. Patients present process long-term furosemide remedy usually need an intravenous bolus dose at least equivalent to their oral dose. Important adverse results embrace hypotension, hypokalemia, hypomagnesemia, and hypocalcemia. There can be in depth proof suggesting that intravenous diuretics might end in a minimum of transient neurohormonal activation which is theoretically disadvantageous. If a continuous diuretic infusion is opted for, it ought to be preceded by a bolus dose, as ought to any subsequent titration within the continuous fee. Diuretic resistance could be addressed with escalating doses of loop diuretics and subsequently with the addition of a thiazide diuretic (hydrochlorothiazide, metolazone, or chlorothiazide). Some diploma of worsening renal operate must typically be tolerated in order to obtain adequate decongestion. However, if progressive renal failure happens despite persistent congestion, ultrafiltration or the addition of an intravenous vasodilator or inotrope needs to be thought-about. When indicators and signs of decompensated coronary heart failure persist regardless of administration of vasodilators and diuretics, intravenous inotropes could also be considered. Their use must be restricted to patients with clear scientific or direct hemodynamic evidence of refractory elevated filling pressures and reduced cardiac output. For sufferers without vital hypotension, the intravenous inodilators dobutamine or milrinone can be utilized to augment cardiac output. Both medicine are related to increased myocardial oxygen demand and cardiac arrhythmias and ought to be used with excessive caution in sufferers with ischemia and preexisting arrhythmias. In cases of extreme hypotension (especially because of administration of vasodilators or -blockers), short-term use of vasopressors similar to dopamine, norepinephrine, and phenylephrine could additionally be necessary. It has a shorter half-life than milrinone and usually is the drug of alternative in the acute setting. On the idea of hemodynamic response, it might be titrated by 1 to 2 g/kg/min every 30 minutes until the specified effect or a dosage of 10 g/kg/min is reached. For sufferers who need an immediate inotropic response, a loading dose of fifty g/ kg over 10 minutes is adopted by an infusion of 0. Ultrafiltration has been used as an alternative alternative to pharmacologic diuresis in acute decompensated coronary heart failure. Whether ultrafiltration must be considered a first-line various to normal intravenous diuretics will rely upon the outcome of future trials assessing the relative security, efficacy, and cost-effectiveness. Currently the use of ultrafiltration is reserved for patients refractory to intravenous diuretic therapy or with diuresis difficult by worsening renal function. This occurred without a reduction in long-term coronary heart failure morbidity or mortality. Tolvaptan and the nonselective intravenous vasopressin receptor inhibitor conivaptan are each permitted for the management of hypervolemic or euvolemic hyponatremia that may accompany decompensated heart failure. Patients with refractory cardiogenic shock and cardiogenic pulmonary edema could profit from the momentary use of intraaortic balloon counterpulsation or another short-term means of mechanical circulatory assist. Diagnosis and administration of atrial and ventricular tachyarrhythmias is crucial to the care of sufferers with acute decompensated coronary heart failure, as these regularly precipitate exacerbations and alter the disease course. The targets of chronic medical remedy are to extend survival and to enhance symptoms and functional status. While there have been few latest major developments in pharmacotherapy, the evolution of therapies with profound survival profit for sufferers with heart failure represents a triumph of modern drugs. It tends to be nonproductive and involuntary, not often resolving with altering the dose or particular agent. It involves delicate tissue edema of the lips, face, tongue, and, sometimes, the oropharynx and epiglottis. The combination of hydralazine and isosorbide dinitrate could provide a reduction in morbidity and mortality in chosen coronary heart failure patients. Side effects of hydralazine could include reflex tachycardia and rarely drug-induced lupus erythematosus. Only carvedilol, bisoprolol, and metoprolol succinate have been permitted for the medical treatment of chronic coronary heart failure. It is important to note that these are relative contraindications and significantly in the setting of reactive airway illness and peripheral arterial disease, the risks of -blocker therapy have to be weighed against their identified benefits. Current recommendations are to start -blockers in those who are clinically euvolemic. Significant bradycardia mandates dose reduction of -blockers and other rate-lowering agents corresponding to digoxin and amiodarone. In follow, carvedilol (with its nonselective, 1-blocking vasodilator effects) may have greater blood pressure reducing than selective 1 agents similar to metoprolol succinate. Both drugs are well tolerated in up to 70% of heart failure patients in our clinics. Intensification of diuretic therapy and dose reduction or slower titration may be needed. Aldosterone receptor antagonists have long been used as weak, potassiumsparing diuretics in patients with coronary heart failure. A basic metabolic panel should be checked inside 1 week after initiation and monitored at common intervals. Our strategy is to initiate remedy with spironolactone as a outcome of its low cost and to transition to eplerenone only within the setting of great gynecomastia. Diuretics are used to preserve euvolemia and to improve symptoms, however their overuse can lead to quantity contraction, hypotension, and renal dysfunction. If this routine fails, a day by day dose of a thiazide diuretic corresponding to metolazone or hydrochlorothiazide may be added 30 minutes previous to furosemide dosing. Very usually, this is contributed to by a failure to adhere to a low-sodium (< 2,000 mg/d) food plan. This is most reliably achieved in patients who document every day weights and make physician-supported adjustments in diuretic dosing on an as-needed basis. Despite a fairly narrow therapeutic window, digoxin is protected and considerably reduces coronary heart failure hospitalizations. Statins ought to be used in the secondary prevention of atherosclerotic cardiovascular disease with out regard to the presence of coronary heart failure.
Laboratory evaluation of a patient probably poisoned with acetaminophen is essential to assess what hepatic injury could have already occurred and to determine plasma concentrations of acetaminophen for prognostic purposes erectile dysfunction medication does not work buy 30 gm himcolin with mastercard. Accurate estimation of acetaminophen in the plasma must be carried out on samples drawn at least 4 hours after ingestion erectile dysfunction smoking himcolin 30 gm purchase overnight delivery, when or previous the time that peak plasma ranges could be anticipated erectile dysfunction history buy himcolin 30 gm amex. Once an correct plasma focus of acetaminophen has been obtained, it must be plotted on the Rumack�Matthew nomogram. This nomogram is based on a collection of patients with and without hepatotoxicity and their corresponding acetaminophen plasma concentrations at presentation. It ought to be noted, nevertheless, that proper use of this nomogram is required, specifically that sure circumstances should be met to apply the nomogram to a selected medical case. The nomogram was validated for a single acetaminophen ingestion, the time of ingestion is critically important to establish the X-axis coordinate for the information point and the plasma concentration should have been obtained at least four hours after ingestion to guarantee that the peak plasma concentration of father or mother acetaminophen has occurred. Similar, though, perhaps much less well established, predictive relationships of drug plasma focus and medical end result and/ or instructed concentrations that require therapeutic interventions can be found for several different medicine together with lithium, salicylates, digoxin, iron, phenobarbital, and theophylline. Some authors have identified "motion ranges" or poisonous threshold values for the measured plasma concentrations of various medicine or chemicals (Ellenhorn, 1997a,b). Generally, these values characterize imply concentrations of the respective substance which have been shown to produce a major harmful effect throughout a retrospective analysis of clinical case series. The pharmaco- (or toxico-) dynamic variability for a given toxicant or for a mix of toxicant is significant, nonetheless. For instance, a patient with a "normal" or "unhazardous" digoxin level may display vital toxic effects and conversely a patient with an elevated or "toxic" plasma focus of digoxin might not show any sign of dangerous effects. The clinical toxicologist is required to critically evaluate the measured drug concentration in context of the medical presentation of the patient and never react to the measured value alone. Because of the restricted clinical availability of "diagnostic" laboratory checks for poisons, toxicologists can gain important perception into a suspected listing of ingested medicine and different chemical substances by performing easy calculations based on routine medical laboratory knowledge. For example, despite the very fact that a affected person could have ingested a large, significantly toxic quantity of methanol, if measured late within the scientific course of the publicity, the osmol gap is in all probability not significantly elevated as most of the osmotically lively methanol has left the plasma and has been biotransformed or cleared but is still producing serious clinical results. Table 33-5 lists several substances that when ingested may be associated with an elevated osmol gap in humans. This is due primarily to the dearth of radiopacity of many oral types of medicine. These and other research have shown that comparatively few formulations of drugs are radiopaque and would likely be detectable by plain X-ray of the abdomen. Generally, plain radiographs can detect a big amount of ingested oral medicine containing ferrous or potassium salts. However, a research of the in vitro and in vivo visualization of chewable oral formulations of iron supplements showed that after the chewable iron was ingested, it was no longer detectable by plain stomach radiograph (Everson et al. However, sure formulations that have an enteric coating or certain kinds of sustained release products are radiopaque and can be visualized (Savitt et al. The most useful radiographs ordered in an overdose or poisoned patient include the chest and stomach radiographs and the computed head tomography examine. The belly radiograph has been used to detect current lead paint ingestion in children because of pica for a couple of years. Although the presence of radiographic evidence of lead-based paint chips in all probability underrepresented the proportion of youngsters with moderate-to-severe lead poisoning in a single research, an belly radiograph exhibiting pica was related to significantly elevated blood lead concentrations (McElvaine et al. Another state of affairs during which an abdominal radiograph may be helpful is the setting of a halogenated hydrocarbon corresponding to carbon tetrachloride or chloroform. Finally, stomach plain radiographs have been useful within the setting the place foreign bodies are detected within the gastrointestinal tract. An example of this is within the situation where an international traveler coming to the United States becomes acutely unwell with indicators of severe sympathomimetic excess and numerous overseas our bodies are visualized all through the gastrointestinal tract. This type of patient is referred to as a physique packer who smuggles illegal substances, similar to cocaine or heroin, by swallowing latex or plastic storage vesicles full of the substance (Beerman et al. Occasionally, these storage gadgets rupture and the drug is released into the gastrointestinal tract with severe and generally fatal results. Aside from these comparatively uncommon conditions, the overall scientific utility for detection and prognosis of poisons by radiography is restricted. In distinction to the restricted medical utility of plain radiography for the identification of a specific poison or to diagnose poisoning, plain radiography and different kinds of diagnostic imaging in scientific toxicology may be extremely useful for the diagnosis of toxicantinduced pathology and to help the scientific toxicologist in the ongoing remedy and patient-management phases of the drug overdose. Detection of drug-induced noncardiac pulmonary edema is related to critical intoxication with salicylates and opioid agonists (Stern et al. Plain chest radiography can detect this abnormality, which would probably correlate with the findings observed during bodily examination of the lungs. This radiographic finding would improve the severity stratification of the poisoning case and potentially alter the deliberate therapeutic strategy for the affected person. The initial clinical evaluation of the poisoned patient is a critically essential section of the therapeutic course of to deal with poisoned people. The physical, laboratory, and radiological examination all contribute to the initial diagnostic steps for poison therapy. The physical and laboratory examinations are generally utilized more from a diagnostic and acute management standpoint, whereas the radiological examination tends to be more useful for detection and management of toxicant-induced pathology. Prevention of Further Poison Absorption During the early phases of therapy of a poisoned affected person who has had a poisonous publicity via the oral, inhalation, or the topical route, the chance to stop further absorption of the poison to reduce the entire quantity of chemical that reaches the systemic circulation may be possible. For chemical compounds introduced by the inhalation route, the principle intervention to stop further absorption is removal of the patient from the surroundings where the toxin is found and to present adequate ventilation and oxygenation for the affected person. For topical exposures, affected person clothing containing the chemical must be eliminated and properly disposed in hermetic wrappings or containers to make sure that the rescuers and healthcare suppliers are adequately shielded from secondary exposure. Most topical exposures require light washing of the skin with water and delicate cleaning soap taking care not to trigger cutaneous abrasions of the pores and skin that will improve dermal absorption. The optimal time to intervene to prevent continued absorption of an oral poison is as soon as attainable after the ingestion. The four major strategies are presently out there for this objective: induction of emesis with syrup of ipecac, gastric lavage, oral administration of activated charcoal, and whole-bowel irrigation. Historically, induction of emesis was accomplished by a wide range of concoctions similar to tartar emetic, an antimony salt, mustard blended in water, concentrated options of copper and zinc salts, and varied botanical substances. In hospitals, apomorphine injection was given even in the 1980s to cause emesis in sufferers with a historical past of probably toxic ingestion. At present, syrup of ipecac is the one agent out there for induction of emesis within the remedy of a probably poisonous ingestion. Syrup of ipecac as a chemical for the prevention of toxicant absorption has largely been changed by activated charcoal, which is discussed below. As stated, the efficacy to take away gastric contents, and therefore reduce subsequent absorption of the chemical declines with enhance within the time interval between poison ingestion and syrup of ipecac administration (Neuvonen et al. An essential space of concern with the decline in use and finally availability of syrup of ipecac is that, for chemical compounds not adsorbed by activated charcoal, there exists a potential void for efficient remedy to prevent additional absorption of orally ingested toxins. Many scientific toxicologists consider that there remains a limited role for the medical use of syrup of ipecac, mainly is rural areas where the length of time earlier than a poisoned affected person can attain medical care is significant, especially when the chemical ingested is poorly adsorbed to activated charcoal. The use of gastric lavage, the technique of putting an orogastric tube into the stomach and aspirating fluid then cyclically instilling fluid and aspirating till the effluent is obvious, has also diminished significantly in current years. The causes for the decline in use of this system embody a growing appreciation of the risk of aspiration in the course of the lavage process and rising evidence that the effectiveness of gastric lavage could additionally be more limited than originally thought. Like induction of emesis, the place the efficacy of the procedure declines with increasing time interval between use of the procedure and the time of ingestion, gastric lavage too has this necessary limitation. It is essential that the orogastric tube be of enough dimension (40�44 French for an adult) to be helpful. Even with a big bore orogastric tube some tablets or capsules could not be capable of move through the tube. In the pediatric affected person, there are practical limitations to the use of giant bore tubes. In this case, orogastric lavage may solely be helpful to try removing of liquid toxins or presumably dissolved tablets or capsules. As described earlier, the medicinal use of charcoal dates again greater than one hundred fifty years. The first reported medicinal use of oral charcoal to adsorb an ingested toxin is credited to the American doctor, Hort, who, in 1834, used massive amounts of powdered charcoal to efficiently deal with a patient poisoned with a chloride salt of mercury.
The elevated cardiac pressures and diminished diastolic filling result in erectile dysfunction doctors mcallen texas buy discount himcolin 30 gm line increased venous stress erectile dysfunction and diabetes a study in primary care 30 gm himcolin generic fast delivery, each pulmonary and systemic erectile dysfunction best pills himcolin 30 gm generic without prescription, and thus to progressive indicators and signs of proper and left heart failure. Although constrictive pericarditis is a relatively unusual cause of coronary heart failure, recognition of this entity is necessary, as its prevalence appears to be increasing and the diagnosis is often missed. The factors concerned within the development of constrictive pericarditis are varied and are just like these of acute pericarditis (Table 40. Neoplastic illness is an exception as a end result of tumor infiltration of the pericardium is usually answerable for constriction. The causes of constrictive pericarditis within the decreasing order of frequency are idiopathic factors, radiation remedy, postsurgical remedy, and infectious illness. This represents a big change from a century ago when infectious illness, specifically tuberculosis, predominated. Since the arrival of effective antitubercular medicines, the number of cases attributable to tuberculosis has dropped precipitously within the United States. However, tuberculosis remains the first reason for constrictive pericarditis in most developing areas of the world. The terminal plateau represents the cessation of flow that happens once the restrict of the rigid pericardium has been reached. It is critical to differentiate between the 2 due to the different treatment strategies. Constrictive pericarditis is a doubtlessly curable illness, whereas remedy options in restrictive cardiomyopathy are sometimes limited to medical remedy. Some surgeons want a preoperative right heart catheterization not solely to verify the diagnosis but additionally to get an correct evaluation of the cardiac index, which may help in surgical planning. There is emerging evidence supporting medical remedy with anti-inflammatory treatment as an preliminary strategy in a patient with inflamed constrictive pericarditis or effusive�constrictive illness. Pericardiectomy is most well-liked generally, although there are particular affected person populations in which medical remedy is appropriate. Medical therapy is also appropriate in patients with severe comorbid diseases that limit life expectancy and/or place them at an unacceptably excessive risk for operative mortality. In addition trial of medical therapy maybe appropriate in inflammatory constrictive pericarditis. More than 90% of patients will report symptomatic enchancment following the process. The presenting syndrome depends on the quantity, the speed of accumulation, and the characteristics of the fluid. Large effusions could also be found unexpectedly and be asymptomatic, whereas rapidly accumulating small effusions might result in tamponade. An unstretched pericardium accommodates solely 80 to 200 mL of quickly accumulating fluid, without a vital change in hemodynamics. In contrast, the pericardial area may accumulate up to 2 L of fluid with none hemodynamic or medical sequelae if this happens slowly. Compressive physiology might happen with rapid accumulation of smaller quantities of fluid if the pericardium is stiff from fibrosis or infiltration by a tumor. Slowly developing pericardial effusions, with no elevation of intrapericardial pressures, are normally asymptomatic. There can also be quite a lot of symptoms from the space-occupying effects of the pericardial fluid on different organs within the chest. These embody dysphagia from esophageal compression, dyspnea from lung compression and atelectasis, hiccups from compression of the phrenic nerve, and nausea and stomach fullness from pressure on adjacent stomach organs. The total intrapericardial volume is mounted; therefore, throughout inspiration, filling of the proper ventricle pushes the septum into the left ventricle. Patients with tamponade will have jugular venous distention, and the x descent is usually the predominant waveform. Common causes of enormous continual effusions embody idiopathic pericarditis, uremia, pericarditis from malignancy or myxedema, congestive coronary heart failure, nephrotic syndrome, cirrhosis, hypothyroidism, postcardiac surgical procedure, and sure medicines. Increase in cardiothoracic ratio with a large distinguished superior vena cava, azygous vein, and decreased pulmonary vascularity should suggest the analysis of pericardial effusion. It allows for accurate analysis, ensures the adequacy of drainage procedures, and permits a qualitative evaluation in following pericardial effusions. Two-dimensional echocardiographic findings are as follows: (1) An echo-free space is discovered between the visceral and parietal pericardium in each systole and diastole. A reasonable effusion could also be categorized as one that surrounds the heart however is 1 cm or much less at its greatest width. Here, although the posterior accumulation continues, the heart seems to settle posteriorly with a larger growth of the pericardial house laterally, apically, and anteriorly. The following might mimic a pericardial effusion on two-dimensional echocardiography. Unless loculated, a pericardial effusion localized to the anterior wall could be very rare. If the fluid relies in the pericardium, the aorta is displaced posteriorly to the effusion, away from the posterior wall of the left atrium. If the fluid is pleural based mostly, the aorta retains its place immediately under the left atrium. It outlines the distribution and supplies an estimate of the pericardial fluid volume that correlates properly with echocardiography. It is very efficient in facilitating detection of loculated pericardial effusions and pericardial thickening. It can even differentiate simple from advanced effusions and pericardial fat from pathologic thickening. The dimension and distribution of the pericardial effusion are easily obtained utilizing this technique. Moreover, differentiation among blood, exudate, chyle, and serous fluid may be achieved owing to the totally different attenuation coefficients for these substances. Diagnostic pericardiocentesis and pericardial fluid examination should be thought of in sufferers with large effusions without clear etiology. Aspirated pericardial fluid must be rigorously inspected and immediately placed in sterile tubes for biochemical, microbiologic, and cytologic examination. The administration of pericardial effusions is dependent upon the underlying etiologic issue, volume, and hemodynamic significance. Although the cause for the effusion is essential, it could usually be determined with out pericardiocentesis by advantage of the medical, systemic, and laboratory options of the presenting condition. Pericardiocentesis is indicated if malignant, bacterial, mycobacterial, or fungal pericardial effusion is suspected. Pericardiocentesis is an indication in the setting of huge pericardial effusion with associated pericardial tamponade (see subsequent text). With massive effusions of recent onset, shut medical and echocardiographic follow-up is warranted. Pericardiocentesis could additionally be warranted in giant asymptomatic pericardial effusions when there are echocardiographic features of early tamponade. Cardiac tamponade occurs when an increase in pericardial fluid raises intrapericardial strain and impairs diastolic filling. Cardiac tamponade is characterized by elevated intracardiac pressures, a progressive limitation of ventricular diastolic filling, and a discount in cardiac output. There seems to be an inverse relationship between the quantity of the pericardial effusion and the cardiac output as quickly as a important quantity is reached. Beyond this, small increments in pericardial quantity end in large will increase in intrapericardial strain. This important quantity depends on the compliance of the pericardium, the speed of fluid accumulation, and the standing of the pericardial lining (infiltrations, calcification, or fibrosis). The raised intrapericardial strain results in a decreased transmural distending pressure that results in decreased diastolic filling. In severe tamponade, the compensatory mechanisms fail, leading to a decreased cardiac output. Reduced coronary perfusion may trigger subendocardial hypoperfusion, further compromising the stroke volume and the cardiac output. The finite space across the heart chambers additionally ends in the equalization of filling pressures with that in the pericardium. Following cardiac surgery, localized pericardial hematoma quite than fluid might impair filling of the heart. The indicators and signs of cardiac tamponade all replicate a low cardiac output: restlessness, agitation, drowsiness, or stupor; decreased urine output; dyspnea; chest discomfort and syncope or near syncope; and weak spot, anorexia, and weight loss with a continual effusion. An echocardiogram might recommend findings consistent with cardiac tamponade, but the medical prognosis requires synthesis of both bedside and echocardiographic findings.






